You might also like
- Treatment of Old Unreduced Posterior Dislocation of ElbowDocument4 pagesTreatment of Old Unreduced Posterior Dislocation of Elbowwenny hildaNo ratings yet
- MG 1Document7 pagesMG 1Cristobal Ramirez FacusseNo ratings yet
- Surgical Treatment of Chronic Elbow Dislocation Allowing For Early Range of Motion: Operative Technique and Clinical ResultsDocument8 pagesSurgical Treatment of Chronic Elbow Dislocation Allowing For Early Range of Motion: Operative Technique and Clinical ResultsLuis Carlos HernandezNo ratings yet
- 10 1093@asj@sjaa018Document60 pages10 1093@asj@sjaa018Luiggi FayadNo ratings yet
- Jurnal Fracture RadiusDocument6 pagesJurnal Fracture RadiusYu PrdnyNo ratings yet
- Clinical and Radiological Outcomes of Osteoarth 2019 Orthopaedics TraumatoDocument6 pagesClinical and Radiological Outcomes of Osteoarth 2019 Orthopaedics TraumatodrelvNo ratings yet
- Paper 48Document4 pagesPaper 48Dr Vineet KumarNo ratings yet
- Chimeric Groin Free Flaps Design and Clinical Application - Microsurgery, Vol. 36 Issue 3 (BZ 22588160)Document10 pagesChimeric Groin Free Flaps Design and Clinical Application - Microsurgery, Vol. 36 Issue 3 (BZ 22588160)Manny TrujilloNo ratings yet
- TOORTHJ 11 452 DikonversiDocument8 pagesTOORTHJ 11 452 DikonversiEndah StyaNo ratings yet
- Experiencia Clinica en Protesis Reversa de Hombro en Centro Medico NavalDocument4 pagesExperiencia Clinica en Protesis Reversa de Hombro en Centro Medico NavalIJAR JOURNALNo ratings yet
- The Surgical Bilio-Digestive Bypass Before Cephalic Pancreaticoduodenectomy, Report of Eight CasesDocument4 pagesThe Surgical Bilio-Digestive Bypass Before Cephalic Pancreaticoduodenectomy, Report of Eight CasesIJAR JOURNALNo ratings yet
- Articulo 2Document6 pagesArticulo 2Maria Alejandra VillaNo ratings yet
- Coccygectomy Z PlastyDocument5 pagesCoccygectomy Z PlastyJayesh BhanushaliNo ratings yet
- SH 3Document8 pagesSH 3ع الNo ratings yet
- Seguimiento A 5 Años PTGH ReversaDocument7 pagesSeguimiento A 5 Años PTGH Reversamarcelogascon.oNo ratings yet
- Primary Total Shoulder Arthroplasty Performed Entirely Thru The Rotator Interval - Technique and Minimum Two-Year OutcomesDocument10 pagesPrimary Total Shoulder Arthroplasty Performed Entirely Thru The Rotator Interval - Technique and Minimum Two-Year OutcomesmotohumeresNo ratings yet
- A New Instrument For Surgical Stabilization of Multiple Rib FracturesDocument9 pagesA New Instrument For Surgical Stabilization of Multiple Rib Fracturesduke3443No ratings yet
- Operative Treatment of Terrible Triad of TheDocument8 pagesOperative Treatment of Terrible Triad of TheAndrea OsborneNo ratings yet
- Closed Intra - Articular Fractures of The Distal End of Humerus Surgically Treated by Trans - Olecranon Approach Using The Chevron OsteotomyDocument4 pagesClosed Intra - Articular Fractures of The Distal End of Humerus Surgically Treated by Trans - Olecranon Approach Using The Chevron OsteotomyIJAR JOURNALNo ratings yet
- Autoinjerto de La Vaina Del Recto Anterior en WRAP-Aumento de La Ruptura Del Tendón de AquilesSDocument5 pagesAutoinjerto de La Vaina Del Recto Anterior en WRAP-Aumento de La Ruptura Del Tendón de AquilesSVillateAngelaNo ratings yet
- Arthroscopic Revision Rotator CuffDocument10 pagesArthroscopic Revision Rotator CuffPujia Cahya AmaliaNo ratings yet
- Mallet Finger Suturing TechniqueDocument5 pagesMallet Finger Suturing TechniqueSivaprasath JaganathanNo ratings yet
- Evaluation of The Results From Surgical Treatment of The Terrible Triad of The ElbowDocument8 pagesEvaluation of The Results From Surgical Treatment of The Terrible Triad of The ElbowBruno FellipeNo ratings yet
- Comparative Study: Lichtensteins Tension-Free Mesh Repair vs. Stoppas Repair For Bilateral Inguinal HerniasDocument6 pagesComparative Study: Lichtensteins Tension-Free Mesh Repair vs. Stoppas Repair For Bilateral Inguinal HerniasIJAR JOURNALNo ratings yet
- Cu Adric Ep Last I Are Vista RobinsonDocument8 pagesCu Adric Ep Last I Are Vista RobinsontomimacagnoNo ratings yet
- Radial Nerve PalsyDocument4 pagesRadial Nerve PalsyRamziNo ratings yet
- Evaluation of Efficacy of Barbed Sutures in Intraoral Wound ClosureDocument9 pagesEvaluation of Efficacy of Barbed Sutures in Intraoral Wound ClosureIJAR JOURNALNo ratings yet
- Nose 2Document11 pagesNose 2Ali MusaNo ratings yet
- Acta 92 26Document14 pagesActa 92 26Gustavo BECERRA PERDOMONo ratings yet
- JR 26 16Document5 pagesJR 26 16ilomurtalaNo ratings yet
- To Study The Necessity of Clamping Versus Non Clamping in Short Duration Urinary Catheter Removal in Operated Orthopaedic PatientsDocument4 pagesTo Study The Necessity of Clamping Versus Non Clamping in Short Duration Urinary Catheter Removal in Operated Orthopaedic PatientsIJAR JOURNALNo ratings yet
- Rotator Cuff Repairs: Mary Schuler MurphyDocument14 pagesRotator Cuff Repairs: Mary Schuler Murphyalexander panduNo ratings yet
- Orthopedics in OrthodonticsDocument7 pagesOrthopedics in OrthodonticsFourthMolar.comNo ratings yet
- 10 1016@j Jse 2019 10 013Document12 pages10 1016@j Jse 2019 10 013Gustavo BECERRA PERDOMONo ratings yet
- Articulo CoronarioDocument7 pagesArticulo CoronarioDayana cipagauta fernandezNo ratings yet
- Duarte Junior 2021Document11 pagesDuarte Junior 2021fumblefumbleNo ratings yet
- Massive Rotator Cuff Tears: Pathomechanics, Current Treatment Options, and Clinical OutcomesDocument13 pagesMassive Rotator Cuff Tears: Pathomechanics, Current Treatment Options, and Clinical OutcomesFillipe AgraNo ratings yet
- The Open Orthopaedics JournalDocument9 pagesThe Open Orthopaedics JournalEndah StyaNo ratings yet
- Jpras Open: Original ArticleDocument11 pagesJpras Open: Original ArticlerchristevenNo ratings yet
- Autologous Fat Transfer in Secondary Carpal Tunnel Release PDFDocument7 pagesAutologous Fat Transfer in Secondary Carpal Tunnel Release PDFdrbantmNo ratings yet
- The Use of Intra Operative Brilliance Amplifier by Novice Surgeons To Improve Bone Tunnels Placement in Anterior Cruciate Ligament Reconstruction During Residency Curriculum Useful or NotDocument7 pagesThe Use of Intra Operative Brilliance Amplifier by Novice Surgeons To Improve Bone Tunnels Placement in Anterior Cruciate Ligament Reconstruction During Residency Curriculum Useful or NotAthenaeum Scientific PublishersNo ratings yet
- Exam Corner - September 2012: The Bone & Joint Journal September 2012Document3 pagesExam Corner - September 2012: The Bone & Joint Journal September 2012Mohamad RamadanNo ratings yet
- 2013artpolsi ActaBiomedicaDocument7 pages2013artpolsi ActaBiomedicaAli MoustafaNo ratings yet
- Adding Mobilisation With Movement To Exercise ... Reid Vicenzino 2022Document8 pagesAdding Mobilisation With Movement To Exercise ... Reid Vicenzino 2022patinoomar67No ratings yet
- Replantation Current Concepts and Outcomes: Clinics in Plastic Surgery July 2014Document12 pagesReplantation Current Concepts and Outcomes: Clinics in Plastic Surgery July 2014Mudassar SattarNo ratings yet
- Injury: Jian Zou, Wei Zhang, Chang-Qing ZhangDocument5 pagesInjury: Jian Zou, Wei Zhang, Chang-Qing Zhangfebyan yohanesNo ratings yet
- Opth 8 1039Document7 pagesOpth 8 1039ririNo ratings yet
- Klin T Berg 2009Document18 pagesKlin T Berg 2009Andrea QuilamanNo ratings yet
- Paper 38Document6 pagesPaper 38Dr Vineet KumarNo ratings yet
- Chapter 69Document24 pagesChapter 69نمر نصارNo ratings yet
- Use of A Static Progressive Stretch Orthosis To Treat Post-Traumatic Ankle StiffnessDocument5 pagesUse of A Static Progressive Stretch Orthosis To Treat Post-Traumatic Ankle StiffnessNararyo anantoNo ratings yet
- MainDocument8 pagesMainRamy ElmasryNo ratings yet
- Aaos 2010Document220 pagesAaos 2010Yusufa ArdyNo ratings yet
- Prosthodontic Rehabilitation of A Mandibulectomy Patient - A Clinical ReportDocument4 pagesProsthodontic Rehabilitation of A Mandibulectomy Patient - A Clinical ReportNeha ChughNo ratings yet
- Current Trends in Preservation RhinoplastyDocument43 pagesCurrent Trends in Preservation RhinoplastyJulls ApouakoneNo ratings yet
- Surgical Repair and Rehabilitation ProtocolsDocument28 pagesSurgical Repair and Rehabilitation ProtocolsSiti FahwizaNo ratings yet
- Injury: Jérôme Pierrart, Thierry Bégué, Pierre Mansat, GeecDocument5 pagesInjury: Jérôme Pierrart, Thierry Bégué, Pierre Mansat, GeecJair FigueroaNo ratings yet
- Engel 2018Document11 pagesEngel 2018GonzaloNo ratings yet
- Artrhoscopic Resection of Volar Wrist Ganglion: Surgical Technique and Case SeriesDocument10 pagesArtrhoscopic Resection of Volar Wrist Ganglion: Surgical Technique and Case SeriesazevedoNo ratings yet
- Anesthesiology Resident Manual of Procedures: A Step-by-Step GuideFrom EverandAnesthesiology Resident Manual of Procedures: A Step-by-Step GuideNo ratings yet
- The Disabled Throwing Shoulder: Spectrum of Pathologyd10-Year UpdateDocument47 pagesThe Disabled Throwing Shoulder: Spectrum of Pathologyd10-Year UpdateSandro RolimNo ratings yet
- S 0749806321003212Document12 pagesS 0749806321003212Sandro RolimNo ratings yet
- The Insertional Footprint of The Rotator Cuff: An Anatomic StudyDocument8 pagesThe Insertional Footprint of The Rotator Cuff: An Anatomic StudySandro RolimNo ratings yet
- Merolla 2015Document8 pagesMerolla 2015Sandro RolimNo ratings yet
- Venipuncture WorksheetDocument5 pagesVenipuncture WorksheetAmy YmaNo ratings yet
- Healing of Intrabony Defects Following Regenerative SurgeryDocument13 pagesHealing of Intrabony Defects Following Regenerative SurgeryYou're Just As Sane As DivaNo ratings yet
- The Effect of Intraoral 2940 Upper Lipp NatachapdfDocument3 pagesThe Effect of Intraoral 2940 Upper Lipp NatachapdfguidepNo ratings yet
- Case ScenarioDocument3 pagesCase ScenarioKhyress Kyla BalalaNo ratings yet
- Advances in Hip Arthroplasty: James Bried, M.DDocument45 pagesAdvances in Hip Arthroplasty: James Bried, M.DErik FisherNo ratings yet
- Appendicitis - Causes, Symptoms, Treatment & PreventionDocument2 pagesAppendicitis - Causes, Symptoms, Treatment & PreventionJr MateoNo ratings yet
- Know About Pediatric Cardiac SurgeryDocument8 pagesKnow About Pediatric Cardiac SurgeryAshish DolasNo ratings yet
- ICO Advanced 115 MCQs 2015-2019Document69 pagesICO Advanced 115 MCQs 2015-2019mrs eleven100% (1)
- An Anatomic Technique For Establishing Leg Length During The Anterior Approach To Total Hip ArthroplastyDocument5 pagesAn Anatomic Technique For Establishing Leg Length During The Anterior Approach To Total Hip Arthroplasty阿欧有怪兽No ratings yet
- Gallstone Ileus PDFDocument4 pagesGallstone Ileus PDFmonika100% (1)
- Post Removal Techniques Part 1: DentistryDocument7 pagesPost Removal Techniques Part 1: DentistryYessenia SarabiaNo ratings yet
- 腰椎间盘突出症诊疗指南Document11 pages腰椎间盘突出症诊疗指南Fu CuNo ratings yet
- Oet 2.0 Writing Practice and Exercises Book For Nurses Vol 2Document184 pagesOet 2.0 Writing Practice and Exercises Book For Nurses Vol 2Dandlers MurrayNo ratings yet
- SurgeryDocument6 pagesSurgeryEthan HuntNo ratings yet
- Wound Ostomy Continence Skills ChecklistDocument4 pagesWound Ostomy Continence Skills ChecklistnorthweststaffingNo ratings yet
- Convergys Emea 2018 HandbookDocument49 pagesConvergys Emea 2018 HandbookFouad LahlouNo ratings yet
- Res Ipsa Loquitor-Application in Medical Negligence: Journal of South India Medicolegal Association January 2014Document13 pagesRes Ipsa Loquitor-Application in Medical Negligence: Journal of South India Medicolegal Association January 2014Ian GreyNo ratings yet
- Post-Operative Instructions: Laparoscopic CholecystectomyDocument2 pagesPost-Operative Instructions: Laparoscopic Cholecystectomyrizwan234No ratings yet
- Implant SystemsDocument103 pagesImplant SystemsBharathi GudapatiNo ratings yet
- Toriumi Et Al 2023 Auricular Composite Graft Survival in RhinoplastyDocument11 pagesToriumi Et Al 2023 Auricular Composite Graft Survival in RhinoplastydrapatriciacieloorlNo ratings yet
- China Care Medical Equipment Co., LTD: 18inch Touch Screen Wireless Ultrasound 15inch Multi LanguageDocument52 pagesChina Care Medical Equipment Co., LTD: 18inch Touch Screen Wireless Ultrasound 15inch Multi Languageالعقار امين عيسىNo ratings yet
- OSCE Notes in Otology Surgery by DrtbaluDocument85 pagesOSCE Notes in Otology Surgery by DrtbaluDrAli JafarNo ratings yet
- Nosocomial Infection Surveillance Methods: Masud Yunesian, M.D., EpidemiologistDocument28 pagesNosocomial Infection Surveillance Methods: Masud Yunesian, M.D., EpidemiologisthendriNo ratings yet
- Comparison of The Effect of Three Treatment Interventions For The Control of Meniere 'S Disease: A Randomized Control TrialDocument6 pagesComparison of The Effect of Three Treatment Interventions For The Control of Meniere 'S Disease: A Randomized Control Trialian danarkoNo ratings yet
- Eb-580s - Operation ManualDocument80 pagesEb-580s - Operation Manualkeng suttisangchanNo ratings yet
- Manual Nobel ActiveDocument56 pagesManual Nobel ActiveJoe PragerNo ratings yet
- FEM Analysis of Bones-1Document5 pagesFEM Analysis of Bones-1Muhammad Daud AliNo ratings yet
- The Process Flowchart at Arnold Palmer HospitalDocument3 pagesThe Process Flowchart at Arnold Palmer HospitalherrajohnNo ratings yet
- Crestal Bone Changes On Platform - Switched Implants and Adjacent Teeth When The Tooth-Implant Distance Is Less Than 1.5 MMDocument10 pagesCrestal Bone Changes On Platform - Switched Implants and Adjacent Teeth When The Tooth-Implant Distance Is Less Than 1.5 MMJuanOso Gutierrez ArayaNo ratings yet
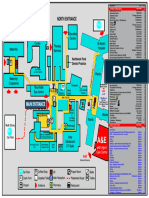
- Northwick Park Hospital Site MapDocument1 pageNorthwick Park Hospital Site MapHasaan KhanNo ratings yet