You might also like
- Infection of Skin Muscles, Bone FinalDocument90 pagesInfection of Skin Muscles, Bone FinalNoelani-Mei Ascio100% (1)
- Fungal InfectionsDocument9 pagesFungal InfectionsCoral Srinivasa RamaluNo ratings yet
- Mycology 2019Document8 pagesMycology 2019Angellie100% (1)
- Infection of The Skin, Soft Tissue, Etc.Document84 pagesInfection of The Skin, Soft Tissue, Etc.fmds100% (1)
- Fungal Infection of The SkinDocument74 pagesFungal Infection of The Skinary_puraNo ratings yet
- BOILS (Furuncle) : Shashank JoshiDocument10 pagesBOILS (Furuncle) : Shashank JoshiKapil LakhwaraNo ratings yet
- Folliculitis, A Simple Guide To the Condition, Treatment And Related DiseasesFrom EverandFolliculitis, A Simple Guide To the Condition, Treatment And Related DiseasesNo ratings yet
- Cutaneous Mycoses GuideDocument55 pagesCutaneous Mycoses GuideAlpana Laisom100% (2)
- Medical Mycology: Fungal Diseases and Cutaneous MycosesDocument54 pagesMedical Mycology: Fungal Diseases and Cutaneous MycosessuwarnyNo ratings yet
- Immunologic Diseases of Oral Cavity: - by Saurabh AhujaDocument34 pagesImmunologic Diseases of Oral Cavity: - by Saurabh AhujaSaurabh AhujaNo ratings yet
- PsoriasisDocument61 pagesPsoriasisWilliam WongNo ratings yet
- Manual IiDocument78 pagesManual IiDaniel Joy ChandranNo ratings yet
- Microbial Diseases of The Skin & EyesDocument52 pagesMicrobial Diseases of The Skin & EyesAna100% (3)
- Candidosis A New ChallengeDocument7 pagesCandidosis A New ChallengeSalvador contreras huertaNo ratings yet
- Bacterial Infections of The SkinDocument41 pagesBacterial Infections of The Skinleenaloveu100% (2)
- Chapter22 LectureDocument45 pagesChapter22 Lecturecee_prasetyo100% (1)
- Pyodermas 2014Document41 pagesPyodermas 2014Dudy Humaedi100% (6)
- Microbial Diseases of the Nervous System: An OverviewDocument30 pagesMicrobial Diseases of the Nervous System: An OverviewBangtan SonyeondanNo ratings yet
- Micr Biology: Microbial Diseases of The Skin and EyesDocument62 pagesMicr Biology: Microbial Diseases of The Skin and EyesIvy L VonierNo ratings yet
- Joshua Radke, MD UC Davis Emergency MedicineDocument47 pagesJoshua Radke, MD UC Davis Emergency MedicineNguyễn Hoàng DungNo ratings yet
- Lecture Note 2A DISEASES OF THE SKIN AND EYEDocument8 pagesLecture Note 2A DISEASES OF THE SKIN AND EYERAFAELLA SALVE MARIE GAETOSNo ratings yet
- Bacterial Disease of The SkinDocument54 pagesBacterial Disease of The SkinsalmaNo ratings yet
- Dermatology Primer: Selected Skin Diseases and Treatment Tailored For The Athletic TrainerDocument64 pagesDermatology Primer: Selected Skin Diseases and Treatment Tailored For The Athletic TrainerSilviu100% (1)
- Diseases of Skin and EyesDocument27 pagesDiseases of Skin and EyesBangtan SonyeondanNo ratings yet
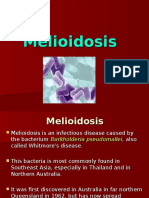
- Melidiosis FDocument24 pagesMelidiosis FVyramuthu AtputhanNo ratings yet
- Microbial Diseases of The Skin and WoundsDocument34 pagesMicrobial Diseases of The Skin and WoundsDagnachew kasayeNo ratings yet
- PSORIASISDocument4 pagesPSORIASISAMOS MELINo ratings yet
- 3.1_FUNGI AND PARASITES_5NOV2021Document50 pages3.1_FUNGI AND PARASITES_5NOV2021haiqalfariq07No ratings yet
- Kuliah Pioderma DR Asih BudiastutiDocument56 pagesKuliah Pioderma DR Asih BudiastutiunisoldierNo ratings yet
- Fungal ClassificationDocument109 pagesFungal ClassificationMirza Shaharyar BaigNo ratings yet
- Microbio Short LessonDocument86 pagesMicrobio Short LessonJom-jom FongNo ratings yet
- Dermatomycosis GuideDocument114 pagesDermatomycosis GuideQonita Qurrota AyunNo ratings yet
- Microbial Diseases of The SkinDocument6 pagesMicrobial Diseases of The SkinIza FaboresNo ratings yet
- Bacterial Skin Infections GuideDocument37 pagesBacterial Skin Infections GuideAngelie PedregosaNo ratings yet
- 16-12-2014 Kuliah Pioderma - Dr. AsihDocument56 pages16-12-2014 Kuliah Pioderma - Dr. AsihSilvia SudjadiNo ratings yet
- Ssti 2021Document65 pagesSsti 2021Ausu OfficialNo ratings yet
- Infectious Dermatosis (Bacterial Skin Infections)Document31 pagesInfectious Dermatosis (Bacterial Skin Infections)Melch PintacNo ratings yet
- RingwormDocument7 pagesRingwormSAMSON, MAXZENE ANICKANo ratings yet
- Skin DisorderDocument82 pagesSkin DisorderPaula Grace MorfeNo ratings yet
- Skin & Eye Infection GuideDocument4 pagesSkin & Eye Infection GuideAdam MoncktonNo ratings yet
- GEJALA KLINIK MIKOSIS DAN PENEGAKAN DIAGNOSA LABORATORIUMDocument36 pagesGEJALA KLINIK MIKOSIS DAN PENEGAKAN DIAGNOSA LABORATORIUMH PNo ratings yet
- Bacterial InfectionsDocument31 pagesBacterial InfectionsWendielynne MillomedaNo ratings yet
- Gram Positive Cocci: StaphylococciDocument57 pagesGram Positive Cocci: StaphylococciJill PardoNo ratings yet
- MIKOLOGI Fungal InfectionDocument31 pagesMIKOLOGI Fungal InfectionAkbar Ahya PutraNo ratings yet
- PYODERMADocument45 pagesPYODERMAAiman Tymer80% (5)
- Shingles Rash Caused by Varicella-Zoster VirusDocument16 pagesShingles Rash Caused by Varicella-Zoster VirusColleen De la RosaNo ratings yet
- Invasive Fungal InfectionsDocument55 pagesInvasive Fungal InfectionsPrincewill SmithNo ratings yet
- M13 v2 Dermatology & STI - LO6Document8 pagesM13 v2 Dermatology & STI - LO6medipro clinicNo ratings yet
- Atopic Dermatitis: Unit 3: Diseases of The Integumentary & Musculoskeletal SystemsDocument21 pagesAtopic Dermatitis: Unit 3: Diseases of The Integumentary & Musculoskeletal Systemsunclet12No ratings yet
- Dermatitis & Urticaria: Department of Dermato Venereology Faculty of Medicine Gadjah Mada UniversityDocument34 pagesDermatitis & Urticaria: Department of Dermato Venereology Faculty of Medicine Gadjah Mada UniversityadystiNo ratings yet
- Bacterial InfectionDocument87 pagesBacterial InfectionYOSEF DERDESAWENo ratings yet
- Microbio Skin and Eyes LectureDocument30 pagesMicrobio Skin and Eyes LecturesweetiepotamusNo ratings yet
- Pathogens that Invade SkinDocument6 pagesPathogens that Invade SkinKarla Karina Dela CruzNo ratings yet
- Care of Clients With Integumentary ProblemsDocument26 pagesCare of Clients With Integumentary ProblemsjeshemaNo ratings yet
- Tinea Cruris Imp Points With ReferencesDocument35 pagesTinea Cruris Imp Points With ReferencesSyed Saqib AliNo ratings yet
- Ectoparasites and Parasites On Human'S Skin/Body Surface: Parasitology DepartmentDocument36 pagesEctoparasites and Parasites On Human'S Skin/Body Surface: Parasitology DepartmentmiaraissaNo ratings yet
- Skin and Soft Tissue Infectons 1Document51 pagesSkin and Soft Tissue Infectons 1AISHWARYA T DNo ratings yet
- (JURNAL) Update Terapy MycosesDocument51 pages(JURNAL) Update Terapy MycosesHabibah Nurla LumiereNo ratings yet
- Ectoparasites and Parasites On Human'S Skin/Body Surface: Parasitology DepartmentDocument36 pagesEctoparasites and Parasites On Human'S Skin/Body Surface: Parasitology DepartmentJimmy Fran IINo ratings yet
- Overview of Skin InfectionsDocument53 pagesOverview of Skin Infectionsadamu mohammadNo ratings yet
- Bio 20 Second Long HandoutsDocument3 pagesBio 20 Second Long HandoutsEmmanuel PlazaNo ratings yet
- CHN Fungal InfectionDocument14 pagesCHN Fungal InfectionChrysteline FabrezNo ratings yet
- Dengue FeverDocument24 pagesDengue FeverSNN100% (1)
- Dermatology Resident NotesDocument37 pagesDermatology Resident Notesedgar mandengNo ratings yet
- Microbial Diseases of The Skin and EyesDocument230 pagesMicrobial Diseases of The Skin and Eyesone_nd_onlyuNo ratings yet
- Bullous Disorders, Bacterial and Fungal Skin InfectionsDocument95 pagesBullous Disorders, Bacterial and Fungal Skin InfectionsDeborah ChemutaiNo ratings yet
- M13 - Dermatology - Chapter 4Document11 pagesM13 - Dermatology - Chapter 4Idham BaharudinNo ratings yet
- Synthesis and Antifungal Activity of Isatin-3-Semicarbazone: S.N. P, K T and S KDocument4 pagesSynthesis and Antifungal Activity of Isatin-3-Semicarbazone: S.N. P, K T and S KzainNo ratings yet
- 1.mycology 1Document36 pages1.mycology 1azoooz502No ratings yet
- MycologyDocument68 pagesMycologyANCHELANo ratings yet
- Fungal Infections of the Skin, Hair and NailsDocument120 pagesFungal Infections of the Skin, Hair and NailsmissirenaNo ratings yet
- Fungal Lung DiseaseDocument9 pagesFungal Lung DiseaseHipsipilasNo ratings yet
- Introduction To FungiDocument4 pagesIntroduction To Fungikep1313No ratings yet
- MycologyDocument117 pagesMycologybanteng wibisonoNo ratings yet
- Pharmaceutical Microbiology and Parasitology (PHMP211)Document59 pagesPharmaceutical Microbiology and Parasitology (PHMP211)Crisamor Rose Pareja ClarisaNo ratings yet
- 07 Mycology00.NewDocument61 pages07 Mycology00.NewvriliadiarNo ratings yet
- MycologyDocument115 pagesMycologyRam Prasad AdhikariNo ratings yet
- Summer Diseases and Its PreventionDocument6 pagesSummer Diseases and Its PreventionJithin M Krishna EzhuthachanNo ratings yet
- Superfical and CutaneousDocument53 pagesSuperfical and CutaneousmulatumeleseNo ratings yet
- Microbial Diversity: Eukaryotic Microbes from Algae to ProtozoaDocument6 pagesMicrobial Diversity: Eukaryotic Microbes from Algae to ProtozoaShane TamilNo ratings yet
- Anti-Fungal Drugs Guide for Mycosis TreatmentDocument6 pagesAnti-Fungal Drugs Guide for Mycosis Treatmentbilal ahmadNo ratings yet
- Review of Literature on Skin DiseasesDocument4 pagesReview of Literature on Skin Diseasesleah manuelNo ratings yet
- Single Dose Fluconazole Effective for Pityriasis VersicolorDocument4 pagesSingle Dose Fluconazole Effective for Pityriasis VersicolorImamatul HikmahNo ratings yet
- Tousif Thesis 2010Document158 pagesTousif Thesis 2010Kristine Dwi PuspitasariNo ratings yet
- Anti-Fungal Drugs SushDocument31 pagesAnti-Fungal Drugs SushCheng XinvennNo ratings yet
- Pathogenesis of Viral InfectionDocument64 pagesPathogenesis of Viral InfectionAnonymous dZowexwHNo ratings yet
- Virulence Factors & Pathogenesis of Fungal InfectionsDocument28 pagesVirulence Factors & Pathogenesis of Fungal InfectionsNipun ShamikaNo ratings yet
- Medical Mycology Arthur F. Di Salvo, MD Reno, NevadaDocument124 pagesMedical Mycology Arthur F. Di Salvo, MD Reno, Nevadablue_blooded23No ratings yet
- Superficial and Cutaneous Mycoses Diagnosis and TreatmentDocument36 pagesSuperficial and Cutaneous Mycoses Diagnosis and TreatmentMich BagamanoNo ratings yet
- Fungal ClassificationDocument109 pagesFungal ClassificationMirza Shaharyar BaigNo ratings yet