You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Hospital SopsDocument12 pagesHospital Sopspratimaz80% (5)
- Pathophysiology of Cardiogenic Pulmonary Edema - UpToDateDocument14 pagesPathophysiology of Cardiogenic Pulmonary Edema - UpToDateStefani AtlleNo ratings yet
- PHCP FinalsDocument75 pagesPHCP FinalsSamantha SantosNo ratings yet
- 072 Insular Life Assurance Co. v. Serafin FelicianoDocument2 pages072 Insular Life Assurance Co. v. Serafin FelicianoJovelan V. Escaño100% (1)
- The Effects of Alcoholism and SmokingDocument1 pageThe Effects of Alcoholism and SmokingFERNANDA EDITH QUIROZ SANTOSNo ratings yet
- Dance Aerobics RoutineDocument28 pagesDance Aerobics RoutineHillary Dwainee R. LorenzoNo ratings yet
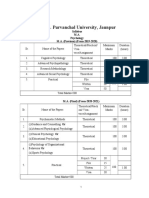
- M.A. I II Psychology SyllabusDocument14 pagesM.A. I II Psychology SyllabusArunodaya Tripathi ArunNo ratings yet
- Otsulip 10%, 20% Soybean Oil (C) : Each 1000ml ContainsDocument4 pagesOtsulip 10%, 20% Soybean Oil (C) : Each 1000ml ContainsDaniel OktavianusNo ratings yet
- MS - Periop POST TESTDocument19 pagesMS - Periop POST TESTJe KirsteneNo ratings yet
- (1957) 1 Q.B. 399Document10 pages(1957) 1 Q.B. 399RPNo ratings yet
- The Efficacy of N-Acetylcysteine in Severe COVID-19 Patients A Structured Summary of A Study Protocol For A Randomised Controlled TrialDocument3 pagesThe Efficacy of N-Acetylcysteine in Severe COVID-19 Patients A Structured Summary of A Study Protocol For A Randomised Controlled TrialTisaNo ratings yet
- Awareness and Use of Malaria Prevention Measures Among Child-Bearing Aged Women in Jere Local Government Area, Borno State, NigeriaDocument21 pagesAwareness and Use of Malaria Prevention Measures Among Child-Bearing Aged Women in Jere Local Government Area, Borno State, NigeriaIJMSRTNo ratings yet
- Restless Development ZimbabweDocument11 pagesRestless Development ZimbabwetaisekwaNo ratings yet
- Quantitative Survey InstrumentDocument15 pagesQuantitative Survey Instrumentسانو روديلNo ratings yet
- Trayopasthambas: Three Supportive Pillars of Ayurveda: October 2013Document6 pagesTrayopasthambas: Three Supportive Pillars of Ayurveda: October 2013Susan SVNo ratings yet
- Cerumen Management A Practical Guide On The.6Document3 pagesCerumen Management A Practical Guide On The.6KoasNo ratings yet
- Zdravlje Izbožije Bašte: Health From God'S GardenDocument3 pagesZdravlje Izbožije Bašte: Health From God'S GardenDrmex GroupNo ratings yet
- Pediatric Tympanoplasty: Factors Affecting Success: Aaron C. Lin and Anna H. MessnerDocument5 pagesPediatric Tympanoplasty: Factors Affecting Success: Aaron C. Lin and Anna H. MessnerAcoet MiezarNo ratings yet
- Population Pharmacokinetics of Rituximab in PatienDocument9 pagesPopulation Pharmacokinetics of Rituximab in PatienGregorius HocevarNo ratings yet
- A Huge Completely Isolated Duplication CystDocument6 pagesA Huge Completely Isolated Duplication CystNurlyanti RustamNo ratings yet
- Telltale Signs of Skin Trespassers - Clues To Superficial MycosisDocument5 pagesTelltale Signs of Skin Trespassers - Clues To Superficial Mycosiskahkashanahmed065No ratings yet
- Liver Abscess ThesisDocument7 pagesLiver Abscess Thesisjenniferalexanderfortlauderdale100% (1)
- Challenge - Stage 9 - Can Disease Be Prevented - tcm143-660703Document5 pagesChallenge - Stage 9 - Can Disease Be Prevented - tcm143-660703victorNo ratings yet
- Module in Mapeh 7 Fourth Quarter/ Week 6 Music Accompaniment in Relation To A Particular Philippine FestivalDocument12 pagesModule in Mapeh 7 Fourth Quarter/ Week 6 Music Accompaniment in Relation To A Particular Philippine FestivalChamp Salcena PerezNo ratings yet
- Tuscola County Health DepartmentDocument2 pagesTuscola County Health DepartmentCourtney BennettNo ratings yet
- CHN Pnle Board Exam Practice-Part 3Document5 pagesCHN Pnle Board Exam Practice-Part 3jerarddaria.elakNo ratings yet
- Decent Work Employment & Transcultural Nursing SAS Session 16Document12 pagesDecent Work Employment & Transcultural Nursing SAS Session 16King NavsunNo ratings yet
- Pephalo Pelvicdisproportion &contracted PelvisDocument38 pagesPephalo Pelvicdisproportion &contracted PelvisAltynaiNo ratings yet
- Hong Et Al, 2022Document7 pagesHong Et Al, 2022Bruno KudekenNo ratings yet
- Life Span Development: A Six-Unit Lesson Plan For High School Psychology TeachersDocument52 pagesLife Span Development: A Six-Unit Lesson Plan For High School Psychology TeachersAndreia AlmeidaNo ratings yet