You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Grammar Tests Upper Intermediate Determiners ...Document4 pagesGrammar Tests Upper Intermediate Determiners ...silvia0% (1)
- Blood TransfusionDocument29 pagesBlood TransfusionNonu Kims100% (1)
- ACG Clinical Guideline Diagnosis Treatment and Prevention of Acute Diarrheal Infections in AdultsDocument14 pagesACG Clinical Guideline Diagnosis Treatment and Prevention of Acute Diarrheal Infections in AdultsMara Medina - BorleoNo ratings yet
- Mandated Reporter FormDocument2 pagesMandated Reporter FormLex TalamoNo ratings yet
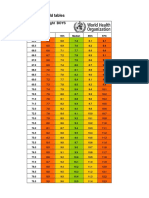
- Boys Simplified Field Tables Weight For Length 2 To 5 Years (Percentiles)Document4 pagesBoys Simplified Field Tables Weight For Length 2 To 5 Years (Percentiles)Gabrielly LopesNo ratings yet
- Health10 q3 Mod1 Healthtrendsissues v5Document27 pagesHealth10 q3 Mod1 Healthtrendsissues v5Wensyl Mae De GuzmanNo ratings yet
- Accuracy of Focused Assessment With Sonography For Trauma (FAST) in Blunt Trauma Abdomen - A Prospective StudyDocument5 pagesAccuracy of Focused Assessment With Sonography For Trauma (FAST) in Blunt Trauma Abdomen - A Prospective StudyEdison HernandezNo ratings yet
- Mine? ? ??Document16 pagesMine? ? ??Samskruthi ChallaNo ratings yet
- Epa HQ Oppt 2016 0231 0241Document109 pagesEpa HQ Oppt 2016 0231 0241Taylor LacyNo ratings yet
- TFN Reviewer PrelimsDocument8 pagesTFN Reviewer PrelimsCUBILLAS, JASMIN G.No ratings yet
- Who Health System Building BlocksDocument2 pagesWho Health System Building BlocksPiny Elleine CesarNo ratings yet
- EFFECTS OF ALUGBATI (Basella Alba) On The Growth Performance of Mallard DuckDocument7 pagesEFFECTS OF ALUGBATI (Basella Alba) On The Growth Performance of Mallard DuckCyLo PatricioNo ratings yet
- Analysis of The Health Financing Structure of BotswanaDocument5 pagesAnalysis of The Health Financing Structure of BotswanaOlusola Olabisi OgunseyeNo ratings yet
- AAAAA - Family Developmental TaskDocument2 pagesAAAAA - Family Developmental TaskMaevan BacolNo ratings yet
- NJSHA NJABA Collaborative Practice GroupDocument4 pagesNJSHA NJABA Collaborative Practice GroupBruno PontesNo ratings yet
- T Manufacturing ProcessesDocument34 pagesT Manufacturing ProcessesMirceaNo ratings yet
- Benjamin P. Solder: EducationDocument3 pagesBenjamin P. Solder: Educationapi-519801593No ratings yet
- EU Approved Units EIA - MaharashtraDocument7 pagesEU Approved Units EIA - MaharashtragibinkumarNo ratings yet
- Jurnal Ckd-EpiDocument6 pagesJurnal Ckd-EpinezaNo ratings yet
- General Practitioner - Endocrinology MCQsDocument17 pagesGeneral Practitioner - Endocrinology MCQsAsif Newaz100% (3)
- Community Needs Assessment Questionnaire 101 1Document12 pagesCommunity Needs Assessment Questionnaire 101 1Dianne NuñalNo ratings yet
- 4.ethico - Legal in Older AdultDocument46 pages4.ethico - Legal in Older AdultShazich Keith LacbayNo ratings yet
- THE Maharashtra Factories Rules, 1963Document19 pagesTHE Maharashtra Factories Rules, 1963arvindtsarkarNo ratings yet
- Gordons Caminade - DoxDocument4 pagesGordons Caminade - DoxZachary CaminadeNo ratings yet
- Lesson Plan PerdevDocument7 pagesLesson Plan PerdevPatzAlzateParaguyaNo ratings yet
- DysgraphiaDocument7 pagesDysgraphiaTehseen Khan100% (1)
- Sabarimala: Virtual-Q Booking CouponDocument2 pagesSabarimala: Virtual-Q Booking CouponST COMMNICATIONNo ratings yet
- Multi-Mechanism Skin Brightening Sabi WhiteDocument6 pagesMulti-Mechanism Skin Brightening Sabi WhiteMuhammad Akhyar RosyidiNo ratings yet
- Principles of CGMP in Pharmaceutical IndustriesDocument6 pagesPrinciples of CGMP in Pharmaceutical IndustriesSamer SowidanNo ratings yet
- INTERSALT Study Findings Public Health and Medical Care ImplicationsDocument9 pagesINTERSALT Study Findings Public Health and Medical Care ImplicationsMore Force CompanyNo ratings yet