You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Case Study 120 (Week2)Document6 pagesCase Study 120 (Week2)Cheska PalomaNo ratings yet
- Case Study #117Document4 pagesCase Study #117Cheska Paloma100% (1)
- AHA - Working On Slope RoofDocument2 pagesAHA - Working On Slope RoofTopsun EnergyNo ratings yet
- Legal Memorandum For ProsecutionDocument5 pagesLegal Memorandum For ProsecutionAnge Buenaventura Salazar88% (8)
- Pediatric Meningitis Case StudyDocument5 pagesPediatric Meningitis Case StudyCheska PalomaNo ratings yet
- This Study Resource WasDocument5 pagesThis Study Resource WasCheska PalomaNo ratings yet
- Family Case StudyDocument7 pagesFamily Case StudyCheska PalomaNo ratings yet
- PHYSICAL and FANCAP Assessment FORMAT 1Document1 pagePHYSICAL and FANCAP Assessment FORMAT 1Cheska PalomaNo ratings yet
- Case Study Antepartum Due May 27thDocument4 pagesCase Study Antepartum Due May 27thCheska PalomaNo ratings yet
- Module 2 Chapter 02 LabDocument3 pagesModule 2 Chapter 02 LabGlecyl Erika Cinco50% (2)
- Case Study 114: InstructionsDocument3 pagesCase Study 114: InstructionsCheska PalomaNo ratings yet
- A. Case in Point-Jeffrey: Planning A Healthy DietDocument4 pagesA. Case in Point-Jeffrey: Planning A Healthy DietCheska PalomaNo ratings yet
- Contraceptives Most Effective (More Than 99%) : Types of Contraceptives Pictures Advantages DisadvantagesDocument4 pagesContraceptives Most Effective (More Than 99%) : Types of Contraceptives Pictures Advantages DisadvantagesCheska PalomaNo ratings yet
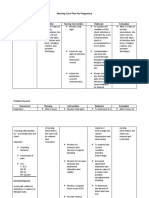
- Nursing Care Plan For Pregnancy: Risk Diagnosis Nursing Diagnosis Objective Nursing Intervention Rationale EvaluationDocument2 pagesNursing Care Plan For Pregnancy: Risk Diagnosis Nursing Diagnosis Objective Nursing Intervention Rationale EvaluationCheska PalomaNo ratings yet
- Case Study: ScenarioDocument5 pagesCase Study: ScenarioCheska PalomaNo ratings yet
- Case Study: ScenarioDocument4 pagesCase Study: ScenarioCheska PalomaNo ratings yet
- Case Simulation in Pediatric Nursing Case Study 2 InstructionsDocument2 pagesCase Simulation in Pediatric Nursing Case Study 2 InstructionsCheska PalomaNo ratings yet
- Case Simulation 115Document6 pagesCase Simulation 115Cheska PalomaNo ratings yet
- Case Simulation in Pediatric Nursing Case Study 1Document4 pagesCase Simulation in Pediatric Nursing Case Study 1Cheska PalomaNo ratings yet
- Worksheet Analytical ExpositionDocument4 pagesWorksheet Analytical Expositionanis mujiNo ratings yet
- Trainee Eye 18 Spring 2023Document14 pagesTrainee Eye 18 Spring 2023MubeenRahmanNo ratings yet
- Gazpromneft Reductor CLP - 68, 100, 150, 220, 320, 460 and 680Document2 pagesGazpromneft Reductor CLP - 68, 100, 150, 220, 320, 460 and 680Jonathan HansenNo ratings yet
- Standa Modules 2022Document39 pagesStanda Modules 2022vlado_314No ratings yet
- Anticoagulation Workshop 7-8 August 2010: Case StudiesDocument11 pagesAnticoagulation Workshop 7-8 August 2010: Case Studieskhangsiean89No ratings yet
- Environmntal Internal & External IssueDocument1 pageEnvironmntal Internal & External IssueMalar KandasamyNo ratings yet
- Unit 12 Asking For The BillDocument3 pagesUnit 12 Asking For The BillPan DaNo ratings yet
- TOR SOCIAL Protection Reform RevisedDocument7 pagesTOR SOCIAL Protection Reform RevisedVesna27No ratings yet
- Hydraulic Pump Unit 1 15Document2 pagesHydraulic Pump Unit 1 15azry_alqadryNo ratings yet
- Hotel Soumyaditi Dated 29.05.2017Document16 pagesHotel Soumyaditi Dated 29.05.2017CA Malay Kumar GiriNo ratings yet
- MKT1 DHM2 211Document9 pagesMKT1 DHM2 211Anyone SomeoneNo ratings yet
- Laparoscopic CatalogDocument44 pagesLaparoscopic CatalogAhmad NuraliNo ratings yet
- Seliwanoff's TestDocument16 pagesSeliwanoff's Testishiyamithe2No ratings yet
- Nov Radiagreen MSDSDocument4 pagesNov Radiagreen MSDSArifin IsawisemanNo ratings yet
- Ideacion Suicida BeckDocument10 pagesIdeacion Suicida BeckLesly Fiorella Vargas BalvinNo ratings yet
- 293005Document10 pages293005elsayedNo ratings yet
- Area Chart Presentation Slides: Lorem Ipsum Dolor Sit Amet, Consectetur Adipiscing Elit. Aliquam Eu Lobortis ErosDocument14 pagesArea Chart Presentation Slides: Lorem Ipsum Dolor Sit Amet, Consectetur Adipiscing Elit. Aliquam Eu Lobortis ErosRahman IskandarNo ratings yet
- Dissertation On Bronchial AsthmaDocument7 pagesDissertation On Bronchial AsthmaInstantPaperWriterSpringfield100% (1)
- The Best Broccoli Cheese Soup (Better-Than-Panera Copycat) - Averie CooksDocument1 pageThe Best Broccoli Cheese Soup (Better-Than-Panera Copycat) - Averie CooksEmily WillisNo ratings yet
- Guidelines For Valve QuantificationDocument1 pageGuidelines For Valve QuantificationZoltán Tirczka100% (1)
- CBAHI-2024-SurveyAgend 3 Days-1Document14 pagesCBAHI-2024-SurveyAgend 3 Days-1rhferanielNo ratings yet
- EAU Guidelines On Urological Infections 2022Document78 pagesEAU Guidelines On Urological Infections 2022Annia KurniawatiNo ratings yet
- Rubrica - Speaking U3 6thDocument1 pageRubrica - Speaking U3 6thmireiaNo ratings yet
- AssamerrrDocument15 pagesAssamerrrVipul SharmaNo ratings yet
- Carburattor Set UpDocument3 pagesCarburattor Set Uppalotito_eNo ratings yet
- Proposal Letter New1Document2 pagesProposal Letter New1api-242445476No ratings yet
- Pruritus in Kidney DiseaseDocument10 pagesPruritus in Kidney DiseaseBrian CastanaresNo ratings yet
- 1 MCM PDFDocument88 pages1 MCM PDFKingsely.shuNo ratings yet