You might also like
- Peptide and Protein DeliveryFrom EverandPeptide and Protein DeliveryChris Van Der WalleRating: 2 out of 5 stars2/5 (1)
- Am J Clin Nutr 2006 Bose 1089 96Document8 pagesAm J Clin Nutr 2006 Bose 1089 96DinisadwNo ratings yet
- Antibiotic Treatment Outcomes in Community-Acquired Pneumonia (#576717) - 734320Document7 pagesAntibiotic Treatment Outcomes in Community-Acquired Pneumonia (#576717) - 734320tofanNo ratings yet
- 10 1097@ftd 0b013e3181898b6f PDFDocument8 pages10 1097@ftd 0b013e3181898b6f PDFintan wahyuNo ratings yet
- Does Antenatal Corticosteroid Therapy Improve Neonatal Outcomes in Late Preterm Birth?Document8 pagesDoes Antenatal Corticosteroid Therapy Improve Neonatal Outcomes in Late Preterm Birth?faikaoesmaniaNo ratings yet
- Supplements Effect of Virgin Coconut OilDocument6 pagesSupplements Effect of Virgin Coconut Oiladitya pratamaNo ratings yet
- Hypertensive Disorders of Pregnancy and Long-TermDocument1 pageHypertensive Disorders of Pregnancy and Long-Termdw21541No ratings yet
- Journal Reading AnakDocument19 pagesJournal Reading AnakPutra Priambodo WibowoNo ratings yet
- Annex 48 Clinical Guidelines For Covid in Malaysia 4th Edition 19102021 FinaleDocument175 pagesAnnex 48 Clinical Guidelines For Covid in Malaysia 4th Edition 19102021 FinaleEfendi AnuarNo ratings yet
- Perioperative Nutrition in Extremely Preterm Infants Undergoing Surgery For Patent Ductus ArteriosusDocument12 pagesPerioperative Nutrition in Extremely Preterm Infants Undergoing Surgery For Patent Ductus ArteriosusOctavianus KevinNo ratings yet
- JN 212308Document8 pagesJN 212308Ivhajannatannisa KhalifatulkhusnulkhatimahNo ratings yet
- PYMS TamizajeDocument6 pagesPYMS TamizajeKevinGallagherNo ratings yet
- NAC en NiñosDocument14 pagesNAC en NiñosAnonymous DxJyWJwtNo ratings yet
- 10.1515 - JPM 2022 0066Document11 pages10.1515 - JPM 2022 0066FETUS10No ratings yet
- A Case of PCAP-C (Individual INP)Document44 pagesA Case of PCAP-C (Individual INP)Preiane PayladoNo ratings yet
- 1471 230X 7 9 PDFDocument5 pages1471 230X 7 9 PDFivanhariachandraNo ratings yet
- Artículo Original / Original ArticleDocument10 pagesArtículo Original / Original ArticleJesu JesuNo ratings yet
- Pone 0209353 PDFDocument23 pagesPone 0209353 PDFFranklin Howley-Dumit SerulleNo ratings yet
- Blood Pressure and Endothelial Function in Healthy, Pregnant Women After Acute and Daily Consumption of Flavanol-Rich ChocolateDocument13 pagesBlood Pressure and Endothelial Function in Healthy, Pregnant Women After Acute and Daily Consumption of Flavanol-Rich ChocolateEstefania Jimenez CruzNo ratings yet
- Association Between Pre-Pregnancy Calcium Intake and Hypertensive Disorders During The First Pregnancy: The Japan Environment and Children 'S StudyDocument8 pagesAssociation Between Pre-Pregnancy Calcium Intake and Hypertensive Disorders During The First Pregnancy: The Japan Environment and Children 'S StudyHanna 1253No ratings yet
- A. Brief Resume of Intended WorkDocument6 pagesA. Brief Resume of Intended WorkRabi DhakalNo ratings yet
- BMJ 33 2 193Document5 pagesBMJ 33 2 193Ami Novianti SubagyaNo ratings yet
- Impact of Coenzyme Q10 On Inflammatory Biomarkers and Its Role in Future Therapeutic StrategiesDocument6 pagesImpact of Coenzyme Q10 On Inflammatory Biomarkers and Its Role in Future Therapeutic StrategiesMichael Kohlberger, BSc MScNo ratings yet
- Lower Vitamin D Levels Are Associated With Increased Risk of Early-Onset Neonatal Sepsis in Term InfantsDocument7 pagesLower Vitamin D Levels Are Associated With Increased Risk of Early-Onset Neonatal Sepsis in Term InfantsMohamed Abo SeifNo ratings yet
- 10 1210@clinem@dgaa336 PDFDocument37 pages10 1210@clinem@dgaa336 PDFAuliya BintanNo ratings yet
- Mypublicationin Int JResearchand Med SC Oct 2015Document9 pagesMypublicationin Int JResearchand Med SC Oct 2015Dr-Dalya ShakirNo ratings yet
- Am J Clin Nutr 2013 Wadhwa 1387 94Document8 pagesAm J Clin Nutr 2013 Wadhwa 1387 94annisanadyapNo ratings yet
- Children 09 01031Document12 pagesChildren 09 01031AIRA MARIE DOROTEONo ratings yet
- The Impact of Kangaroo Mother Care On The Outcome of Premature Babies at The Regional Hospital BueaDocument7 pagesThe Impact of Kangaroo Mother Care On The Outcome of Premature Babies at The Regional Hospital BueaAthenaeum Scientific PublishersNo ratings yet
- Food Safety Knowledge and Practices PDFDocument9 pagesFood Safety Knowledge and Practices PDFRameesha AhmedNo ratings yet
- Clinical Assessment of Fetal Well-Being and FetalDocument12 pagesClinical Assessment of Fetal Well-Being and Fetalhenri kaneNo ratings yet
- Đặc tính bảo vệ chuyển hóa và chống viêm của huyết thanh giàu dưỡng chất cho con người sau khi hấp thụ chiết xuất từ lá atisô Kết quả từ một thử nghiệm lâm sàng Ex Vivo cải tiếnDocument23 pagesĐặc tính bảo vệ chuyển hóa và chống viêm của huyết thanh giàu dưỡng chất cho con người sau khi hấp thụ chiết xuất từ lá atisô Kết quả từ một thử nghiệm lâm sàng Ex Vivo cải tiếnLại Ngọc MaiNo ratings yet
- Piis1036731421001144 PDFDocument7 pagesPiis1036731421001144 PDFvaloranthakam10No ratings yet
- Daily Quercetin Supplementation Dose Dependently Increases Plasma Quercetin Concentration in Healthy HumanDocument7 pagesDaily Quercetin Supplementation Dose Dependently Increases Plasma Quercetin Concentration in Healthy HumanNguyen Thuy100% (1)
- Gupta2013 Article TherapeuticRolesOfCurcuminLess PDFDocument24 pagesGupta2013 Article TherapeuticRolesOfCurcuminLess PDFBadiu ElenaNo ratings yet
- PIIS2405457722004831Document4 pagesPIIS2405457722004831Karla Rosángel CordónNo ratings yet
- Pneumonia in Infants and ChildrenDocument52 pagesPneumonia in Infants and ChildrenMikeyNo ratings yet
- Ebn Pneumonia 3Document12 pagesEbn Pneumonia 3Nadhiratul LayliNo ratings yet
- 4 FarahdinaDocument6 pages4 Farahdinazaki ahmadNo ratings yet
- 11111Document19 pages11111Nejc KovačNo ratings yet
- Akin Et Al Diabetes Vaccination Cost EffectivenessDocument14 pagesAkin Et Al Diabetes Vaccination Cost Effectivenessreza_adrian_2No ratings yet
- Probiotics and Preterm Infants A Position Paper.26 ShareDocument17 pagesProbiotics and Preterm Infants A Position Paper.26 Shareendy tovarNo ratings yet
- 2011 Ispad NeumoníaDocument14 pages2011 Ispad NeumoníaAaron Nureña JaraNo ratings yet
- Nac Idsa PDFDocument52 pagesNac Idsa PDFYULIETH ANDREA SAAVEDRA COGOLLONo ratings yet
- The Effect of Topical Ointment On Neonatal Sepsis in Preterm InfantsDocument4 pagesThe Effect of Topical Ointment On Neonatal Sepsis in Preterm InfantsJill R SendowNo ratings yet
- 1ap83sDocument15 pages1ap83sAmanda Figueiredo LimaNo ratings yet
- 10 1016@j Earlhumdev 2020 104984Document5 pages10 1016@j Earlhumdev 2020 104984Ahmed BaghdadiNo ratings yet
- ESPEN Guideline On Clinical Nutrition in Inflammatory Bowel DiseaseDocument28 pagesESPEN Guideline On Clinical Nutrition in Inflammatory Bowel DiseaseAi NurfaiziyahNo ratings yet
- Supplementation of Vitamin E, Vitamin C, and Zinc Attenuates Oxidative Stress in Burned Children: A Randomized, Double-Blind, Placebo-Controlled Pilot StudyDocument8 pagesSupplementation of Vitamin E, Vitamin C, and Zinc Attenuates Oxidative Stress in Burned Children: A Randomized, Double-Blind, Placebo-Controlled Pilot StudyBruna Do CarmoNo ratings yet
- Usefulness of Screening Tests For Diagnosis of Latent Tuberculosis Infection in ChildrenDocument22 pagesUsefulness of Screening Tests For Diagnosis of Latent Tuberculosis Infection in ChildrenLinda MaylianaNo ratings yet
- Antibiotic Resistance Patterns of Urinary Tract Pathogens in Turkish ChildrenDocument5 pagesAntibiotic Resistance Patterns of Urinary Tract Pathogens in Turkish ChildrenLavfy NjlaaNo ratings yet
- Using of Iron, Vitamin D, Multivitamin in Pregnant Women and The Related FactorsDocument9 pagesUsing of Iron, Vitamin D, Multivitamin in Pregnant Women and The Related FactorsUswatun HasanahNo ratings yet
- สารในเห็ดการบูรต้านมะเร็ง10Document12 pagesสารในเห็ดการบูรต้านมะเร็ง10patarapen.mNo ratings yet
- Operational Guidelines-Use of Antenatal Corticosteroids in Preterm LabourDocument32 pagesOperational Guidelines-Use of Antenatal Corticosteroids in Preterm LabourPriyaancaHaarshNo ratings yet
- Jaqt 05 I 3 P 215Document3 pagesJaqt 05 I 3 P 215Patrick RamosNo ratings yet
- ESPEN Practical Guideline Clinical Nutrition in Inflammatory Bowel DiseaseDocument22 pagesESPEN Practical Guideline Clinical Nutrition in Inflammatory Bowel DiseaseChico MotaNo ratings yet
- Kefir AlzheimersDocument14 pagesKefir AlzheimersAnanyaNo ratings yet
- AlzheimerDocument15 pagesAlzheimerMillicent SongsterNo ratings yet
- Nutritional Management of The Critically Ill.29Document16 pagesNutritional Management of The Critically Ill.29Ririn Muthia ZukhraNo ratings yet
- The S2 Subunit of QX-type Infectious Bronchitis CoronavirusDocument14 pagesThe S2 Subunit of QX-type Infectious Bronchitis CoronavirusmmNo ratings yet
- Yang2014 Article CoronavirusDocument10 pagesYang2014 Article CoronavirusmmNo ratings yet
- Wuhan Engineered CoronavirusDocument13 pagesWuhan Engineered CoronavirusmmNo ratings yet
- Decoding Covid-19 With The Sars-Cov-2 GenomeDocument12 pagesDecoding Covid-19 With The Sars-Cov-2 GenomemmNo ratings yet
- in Response YanDocument13 pagesin Response Yaninappropriate entertainmentNo ratings yet
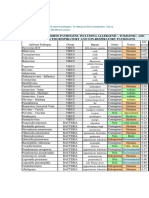
- List of Airborne Pathogens, Including Allergenic, Toxigenic, and Suspected Respiratory and Non-Respiratory PathogensDocument4 pagesList of Airborne Pathogens, Including Allergenic, Toxigenic, and Suspected Respiratory and Non-Respiratory PathogensmmNo ratings yet
- NSSM 200 Kissinger Genocide Report 1974Document123 pagesNSSM 200 Kissinger Genocide Report 1974Guy Razer100% (12)
- Technical Briefing 21Document36 pagesTechnical Briefing 21Alan KauthNo ratings yet
- SQuay - Bayesian Analysis of SARS-CoV-2 FINAL v.2Document193 pagesSQuay - Bayesian Analysis of SARS-CoV-2 FINAL v.2Natalie Winters100% (18)
- Sensory Neuronal Sensitisation Occurs Through HMGB-1-RAGEDocument10 pagesSensory Neuronal Sensitisation Occurs Through HMGB-1-RAGEmmNo ratings yet
- Air Polution and CovidDocument66 pagesAir Polution and CovidmmNo ratings yet
- JPNR - S09 - 1114Document7 pagesJPNR - S09 - 1114arunkumar kumararunNo ratings yet
- Deaths Involving COVID-19 by Vaccination Status, England Deaths Occurring Between 1 April 2021 and 31 May 2023Document7 pagesDeaths Involving COVID-19 by Vaccination Status, England Deaths Occurring Between 1 April 2021 and 31 May 2023Mihai MotorgaNo ratings yet
- Reflection Paper: "The Next Outbreak? We Are Not Ready?" by Bill GatesDocument2 pagesReflection Paper: "The Next Outbreak? We Are Not Ready?" by Bill GatesKyla CastroNo ratings yet
- Knowledge, Attitude, and Practice During The COVID-19 Pandemic: A ReviewDocument7 pagesKnowledge, Attitude, and Practice During The COVID-19 Pandemic: A ReviewilhamNo ratings yet
- #Coronavirus Protocols Society of Dowsers Heather WilksDocument2 pages#Coronavirus Protocols Society of Dowsers Heather WilksAivlysNo ratings yet
- 20 de Tieng Anh On Thi Vao 10 Nam 23 24Document63 pages20 de Tieng Anh On Thi Vao 10 Nam 23 24Ánh NguyễnNo ratings yet
- Middle East Respiratory Syndrome Coronavirus (MERS-CoV)Document24 pagesMiddle East Respiratory Syndrome Coronavirus (MERS-CoV)Nurul Falah KalokoNo ratings yet
- Maternal Respiratory Sars-Cov-2 Infection in Pregnancy Is Associated With A Robust Inflammatory Response at The Maternal-Fetal InterfaceDocument31 pagesMaternal Respiratory Sars-Cov-2 Infection in Pregnancy Is Associated With A Robust Inflammatory Response at The Maternal-Fetal InterfaceAllan Depieri CataneoNo ratings yet
- Daszak Letter 6 Feb 2020Document18 pagesDaszak Letter 6 Feb 2020Jim HoftNo ratings yet
- Covid Reference: Bernd Sebastian Kamps Christian HoffmannDocument172 pagesCovid Reference: Bernd Sebastian Kamps Christian HoffmannZubair Mahmood KamalNo ratings yet
- English: First Quarter - Module 4Document20 pagesEnglish: First Quarter - Module 4Mercy Villanueva Pineda100% (1)
- Wipo Pub 1075 en Covid 19 Related Vaccines and Therapeutics - 221203 - 205822Document84 pagesWipo Pub 1075 en Covid 19 Related Vaccines and Therapeutics - 221203 - 205822Omar TananeNo ratings yet
- COVID-19 Schools Summary PDFDocument18 pagesCOVID-19 Schools Summary PDFActionNewsJaxNo ratings yet
- The Epidemiological Triangle On COVID 19Document2 pagesThe Epidemiological Triangle On COVID 19Pinku KhanNo ratings yet
- Formato de GlosarioDocument19 pagesFormato de GlosarioArturo Saavedra VargasNo ratings yet
- COVID-19 Ag Test Kit: (For Medical Professional Use Only)Document2 pagesCOVID-19 Ag Test Kit: (For Medical Professional Use Only)threwawayNo ratings yet
- The Covid-19 Pandemic and Haemoglobin Disorders: Vaccinations & Therapeutic DrugsDocument53 pagesThe Covid-19 Pandemic and Haemoglobin Disorders: Vaccinations & Therapeutic DrugsJuanGabrielVillamizarNo ratings yet
- COVID BIology, by Godwin Paul v. EfondoDocument2 pagesCOVID BIology, by Godwin Paul v. EfondoGodwin Paul EfondoNo ratings yet
- Soal Bahasa Inggris XI-2 1920Document10 pagesSoal Bahasa Inggris XI-2 1920ameliaNo ratings yet
- Origin, Transmission, Diagnosis and Management of Coronavirus Disease 2019 (COVID-19)Document6 pagesOrigin, Transmission, Diagnosis and Management of Coronavirus Disease 2019 (COVID-19)Alfitrah NurjayaNo ratings yet
- Tell Why: A Persuasive Writing: Selected Topic EN6WC-Ivb-2.2Document12 pagesTell Why: A Persuasive Writing: Selected Topic EN6WC-Ivb-2.2Maricar MagallanesNo ratings yet
- Geert Vanden Bossche Open Letter WHO March 6 2021Document5 pagesGeert Vanden Bossche Open Letter WHO March 6 2021tim4haagensen100% (1)
- Wpsar.2013.4.3 International Health RegulationsDocument66 pagesWpsar.2013.4.3 International Health RegulationsEric WhitfieldNo ratings yet
- The Impact of COVID-19 On The Indian EconomyDocument17 pagesThe Impact of COVID-19 On The Indian EconomySiddid MishraNo ratings yet
- GD Topic - Coronavirus - 'Black Swan' of Global Economy How It Impacts India - PDFDocument10 pagesGD Topic - Coronavirus - 'Black Swan' of Global Economy How It Impacts India - PDFAshutosh Sharma100% (1)
- Module 1 1 PDFDocument12 pagesModule 1 1 PDFSsa RiNo ratings yet
- Student Assessment During COVID-19 - Center For American ..Document4 pagesStudent Assessment During COVID-19 - Center For American ..maria evangelistaNo ratings yet
- IP Project Covid-19 ImpactDocument24 pagesIP Project Covid-19 Impactameysoni76No ratings yet
- Genomic Evolution 2024 FBDocument35 pagesGenomic Evolution 2024 FBtpm8zjjw59No ratings yet
- Avian Flu in South East AsiaDocument160 pagesAvian Flu in South East AsiaMaria Sri PangestutiNo ratings yet