You might also like
- Journal ReadingDocument45 pagesJournal ReadingArief FakhrizalNo ratings yet
- Atelectasis 2Document12 pagesAtelectasis 2Arief FakhrizalNo ratings yet
- Acoustic Reflex: Presented by Arief Fakhrizal, DR Supervisor: Dr. Wijana, SP - THTKL (K)Document48 pagesAcoustic Reflex: Presented by Arief Fakhrizal, DR Supervisor: Dr. Wijana, SP - THTKL (K)Arief FakhrizalNo ratings yet
- Rano - JR - SSHLDocument29 pagesRano - JR - SSHLArief FakhrizalNo ratings yet
- Atelectasis 1Document17 pagesAtelectasis 1Arief FakhrizalNo ratings yet
- Nitric Oxide and OSA FixDocument45 pagesNitric Oxide and OSA FixArief FakhrizalNo ratings yet
- The Preoperative Sinus CT: Avoiding A "Close" Call With Surgical ComplicationDocument28 pagesThe Preoperative Sinus CT: Avoiding A "Close" Call With Surgical ComplicationArief FakhrizalNo ratings yet
- Laryngitis: Wahyu Priatmoko 1301 1207 0197 Ilman Fathony 1301 1207 007Document74 pagesLaryngitis: Wahyu Priatmoko 1301 1207 0197 Ilman Fathony 1301 1207 007Arief FakhrizalNo ratings yet
- Tugas AntonDocument10 pagesTugas AntonArief FakhrizalNo ratings yet
- Skin Prick Test & Modified Quantitative TestDocument27 pagesSkin Prick Test & Modified Quantitative TestArief FakhrizalNo ratings yet
- LR QOL Qusstionnaire THTKOM WD (Autosaved)Document25 pagesLR QOL Qusstionnaire THTKOM WD (Autosaved)Arief FakhrizalNo ratings yet
- NSR 7 3 22 Corpal KoinDocument10 pagesNSR 7 3 22 Corpal KoinArief FakhrizalNo ratings yet
- WD LaryngitisDocument80 pagesWD LaryngitisArief FakhrizalNo ratings yet
- NSR Abses 2 Okt 21Document23 pagesNSR Abses 2 Okt 21Arief FakhrizalNo ratings yet
- Laryngitis: Yanti NurrokhmawatiDocument73 pagesLaryngitis: Yanti NurrokhmawatiArief FakhrizalNo ratings yet
- Piter - LR - Peripheral Balance Examination1Document29 pagesPiter - LR - Peripheral Balance Examination1Arief FakhrizalNo ratings yet
- Obstructive Sleep Apnea: Arief Fakhrizal Supervisor: Dr. Dr. Sinta Sari Ratunanda, M. Kes., Sp. T.H.T.K.L. (K)Document61 pagesObstructive Sleep Apnea: Arief Fakhrizal Supervisor: Dr. Dr. Sinta Sari Ratunanda, M. Kes., Sp. T.H.T.K.L. (K)Arief FakhrizalNo ratings yet
- Piter - LR - Pure Tone Audiometry and MaskingDocument44 pagesPiter - LR - Pure Tone Audiometry and MaskingArief FakhrizalNo ratings yet
- Pediatric - Hearing - Loss Lau 3-17-10Document45 pagesPediatric - Hearing - Loss Lau 3-17-10Arief FakhrizalNo ratings yet
- Sejarah Dan Perkembangan Ilmu Bedah September 2017Document18 pagesSejarah Dan Perkembangan Ilmu Bedah September 2017Arief Fakhrizal100% (1)
- Keamanan Dan Toksisitas Cempedak.Document13 pagesKeamanan Dan Toksisitas Cempedak.Arief FakhrizalNo ratings yet
- Bone and Soft Tissue HealingDocument28 pagesBone and Soft Tissue HealingArief FakhrizalNo ratings yet
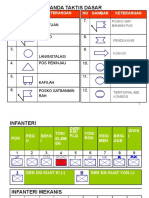
- Tanda Taktis Dasar: 1. Kesatuan 2. Posko 7Document8 pagesTanda Taktis Dasar: 1. Kesatuan 2. Posko 7Arief FakhrizalNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Specialty Pharmaceutical Biotechnology Sales in Sarasota FL Resume Jeffrey MinettDocument1 pageSpecialty Pharmaceutical Biotechnology Sales in Sarasota FL Resume Jeffrey MinettJeffreyMinettNo ratings yet
- Henry Schein Orthodontics Catalog - General SuppliesDocument8 pagesHenry Schein Orthodontics Catalog - General SuppliesOrtho OrganizersNo ratings yet
- 2019 EC 006 REORGANIZING BADAC Zone - 1Document5 pages2019 EC 006 REORGANIZING BADAC Zone - 1Barangay BotongonNo ratings yet
- TUM CoursesDocument3 pagesTUM CoursesJoao N Da SilvaNo ratings yet
- Theology of The BodyDocument2 pagesTheology of The BodyKim JuanNo ratings yet
- MMG 301 Study Guide For Exam 1Document14 pagesMMG 301 Study Guide For Exam 1Juyeon CheongNo ratings yet
- BCG - The Future of Jobs in The Era of AI - 2021 - NeiDocument40 pagesBCG - The Future of Jobs in The Era of AI - 2021 - NeiHevertom FischerNo ratings yet
- SRP Batch 1Document32 pagesSRP Batch 1eenahNo ratings yet
- Health and Wellness Programs For CVommercial Truck Drivers 144 PagesDocument91 pagesHealth and Wellness Programs For CVommercial Truck Drivers 144 PagesDenise Mathre100% (1)
- Threats On Child Health and SurvivalDocument14 pagesThreats On Child Health and SurvivalVikas SamvadNo ratings yet
- Non Hodgkin Lymphoma Complete PDFDocument104 pagesNon Hodgkin Lymphoma Complete PDFelika dwiNo ratings yet
- Special Consideration in Neonatal Resuscitation - 2022 - Seminars in PerinatologDocument8 pagesSpecial Consideration in Neonatal Resuscitation - 2022 - Seminars in PerinatologEduardo Rios DuboisNo ratings yet
- Psychoanalisis and PaediatricsDocument264 pagesPsychoanalisis and PaediatricsBlackKNo ratings yet
- Migrants' Election ManifestoDocument2 pagesMigrants' Election ManifestoMimi Panes - CorosNo ratings yet
- Dwnload Full Wardlaws Contemporary Nutrition A Functional Approach 5th Edition Wardlaw Test Bank PDFDocument36 pagesDwnload Full Wardlaws Contemporary Nutrition A Functional Approach 5th Edition Wardlaw Test Bank PDFamoeboid.amvis.uiem100% (9)
- Bayley Scales of Infant Development IIDocument2 pagesBayley Scales of Infant Development IIbutterflybaby04No ratings yet
- Fatimah Kti FixDocument71 pagesFatimah Kti FixOktaviani MuhaddistNo ratings yet
- Conflict or Consensus - An Investigation of Stakeholder Concerns DuringDocument10 pagesConflict or Consensus - An Investigation of Stakeholder Concerns DuringhohoexeNo ratings yet
- AP GeographyDocument95 pagesAP GeographyKhimavathBharathNaik88% (8)
- University of Cambridge International Examinations General Certificate of Education Ordinary LevelDocument8 pagesUniversity of Cambridge International Examinations General Certificate of Education Ordinary LevelKelvin SerimweNo ratings yet
- Jumpstart: Name: Angel E. PicazoDocument2 pagesJumpstart: Name: Angel E. PicazoAngel PicazoNo ratings yet
- Manual of Homeopathic Practice (1876)Document864 pagesManual of Homeopathic Practice (1876)Dr. JimNo ratings yet
- The Amazing DeclineDocument26 pagesThe Amazing DeclineSuzanne HumphriesNo ratings yet
- The Toxicology of Chlorine: School of Safety Science, University of New South Wales, Sydney NSW 2052, AustraliaDocument10 pagesThe Toxicology of Chlorine: School of Safety Science, University of New South Wales, Sydney NSW 2052, AustraliaAswar MakrufNo ratings yet
- Mia Deal or No Deal 2.3.7.A1Document2 pagesMia Deal or No Deal 2.3.7.A1bxnds. zay0% (1)
- Daftar PustakaDocument1 pageDaftar PustakaDaffa ArkanantaNo ratings yet
- Alwyn Naicker - Research Proposal Assignment 2 PDFDocument15 pagesAlwyn Naicker - Research Proposal Assignment 2 PDFAlwyn NaickerNo ratings yet
- Prevention of Foodborne Disease: The Five Keys To Safer FoodDocument2 pagesPrevention of Foodborne Disease: The Five Keys To Safer FoodThong Boon LeongNo ratings yet
- New Mcgraw Hill EducationDocument132 pagesNew Mcgraw Hill EducationAlexandru LeșanNo ratings yet
- Kit For Human Thyroid Stimulating Hormone (HTSH) : Irmak-9Document2 pagesKit For Human Thyroid Stimulating Hormone (HTSH) : Irmak-9micky mouseNo ratings yet