You might also like
- Canadian Pharmacy Review Ver1Document6 pagesCanadian Pharmacy Review Ver1Mon MonNo ratings yet
- Clinical Approach To Lymphadenopathy: Review ArticleDocument8 pagesClinical Approach To Lymphadenopathy: Review ArticleSigitNo ratings yet
- Nefro 341 REVIEWTreatmentoflupusnephritis OKDocument9 pagesNefro 341 REVIEWTreatmentoflupusnephritis OKSelena GajićNo ratings yet
- Lymph Node EnlargementDocument6 pagesLymph Node Enlargementlucas mansanoNo ratings yet
- Linfadenopatias BenignasDocument9 pagesLinfadenopatias Benignasangelo marinoNo ratings yet
- Abordaje Linfadenopatia PerifericaDocument13 pagesAbordaje Linfadenopatia PerifericaTony Gomez Luna LeyvaNo ratings yet
- Laryngeal Amyloidosis: ReviewDocument8 pagesLaryngeal Amyloidosis: ReviewLuis De jesus SolanoNo ratings yet
- Prevalence of Brain LymphomaDocument1 pagePrevalence of Brain LymphomaHengky KurniawanNo ratings yet
- Lymphadenopathy in ChildrenDocument5 pagesLymphadenopathy in ChildrenMaria PaulaNo ratings yet
- Utilidad Del Lavado Broncoalveolar en La Evaluación de La Enfermedad Pulmonar IntersticialDocument8 pagesUtilidad Del Lavado Broncoalveolar en La Evaluación de La Enfermedad Pulmonar IntersticialAlexis Guevara QuijadaNo ratings yet
- Efusi Pleura MaskellDocument10 pagesEfusi Pleura MaskellYessica Chrystie Dian SinurayaNo ratings yet
- Non-Hodgkin's LymphomasDocument23 pagesNon-Hodgkin's LymphomasshevmyrNo ratings yet
- Hannah JRDocument8 pagesHannah JRPatty GracinoNo ratings yet
- HHS Public Access: New Diagnostic Modalities in The Evaluation of LymphedemaDocument23 pagesHHS Public Access: New Diagnostic Modalities in The Evaluation of LymphedemataufikolingNo ratings yet
- Pennsylvania: L U P U S N E W SDocument21 pagesPennsylvania: L U P U S N E W SPison Hawila PardedeNo ratings yet
- AcuteLiverFailureUpdate201journalformat1 PDFDocument26 pagesAcuteLiverFailureUpdate201journalformat1 PDFDewanggaWahyuPrajaNo ratings yet
- Advances in Treatment of Progressive Multifocal LeukoencephalopathyDocument17 pagesAdvances in Treatment of Progressive Multifocal LeukoencephalopathyRandy UlloaNo ratings yet
- Lupus Nephritis... CureusDocument8 pagesLupus Nephritis... CureusAnab Rehan TaseerNo ratings yet
- AcuteLiverFailureUpdate201journalformat1 2 PDFDocument26 pagesAcuteLiverFailureUpdate201journalformat1 2 PDFHuy HuynhNo ratings yet
- Systemic Lupus ErythematosusDocument12 pagesSystemic Lupus ErythematosusEdwin WardhanaNo ratings yet
- Lupus Literature ReviewDocument6 pagesLupus Literature Reviewc5t9rejg100% (2)
- Lupus Nephritis: Disease of The MonthDocument12 pagesLupus Nephritis: Disease of The MonthHanik FiriaNo ratings yet
- Research Paper LupusDocument10 pagesResearch Paper Lupusfypikovekef2100% (1)
- Progressive myoclonus epilepsiesDocument11 pagesProgressive myoclonus epilepsiesbirriederesse42No ratings yet
- AASLD Position Paper The Management of Acute Liver FailureDocument19 pagesAASLD Position Paper The Management of Acute Liver FailurePhan Nguyễn Đại NghĩaNo ratings yet
- Dennis Wright, Bruce J Addis, Anthony S-Y Leong - Diagnostic Lymph Node Pathology, 2nd Edition (2011, CRC Press)Document185 pagesDennis Wright, Bruce J Addis, Anthony S-Y Leong - Diagnostic Lymph Node Pathology, 2nd Edition (2011, CRC Press)Daniel RojoNo ratings yet
- Art 3A10.1186 2F2049 6958 7 4Document6 pagesArt 3A10.1186 2F2049 6958 7 4Ivan RisnaNo ratings yet
- Is The Renal Biopsy Still Necessary in Lupus Nephropathy?Document4 pagesIs The Renal Biopsy Still Necessary in Lupus Nephropathy?Hosne araNo ratings yet
- European J of Haematology - 2022 - Paquin - The Diagnosis and Management of Suspected Lymphoma in General PracticeDocument11 pagesEuropean J of Haematology - 2022 - Paquin - The Diagnosis and Management of Suspected Lymphoma in General PracticeaminmofrehNo ratings yet
- OLPandupdate Carrozzo ThorpeDocument13 pagesOLPandupdate Carrozzo ThorpeAstrid Dwi SattiNo ratings yet
- Etiology and Pathogenesis of OLP - Kurago 2015 PDFDocument9 pagesEtiology and Pathogenesis of OLP - Kurago 2015 PDFintanNo ratings yet
- The Behaviour of Serum Survivin in Patients With Lupus NephritisDocument9 pagesThe Behaviour of Serum Survivin in Patients With Lupus Nephritismirandanasution1209No ratings yet
- Hypomyelinating Leukodystrophies Translational Research Progress and ProspectsDocument15 pagesHypomyelinating Leukodystrophies Translational Research Progress and ProspectsgomaNo ratings yet
- Thesis IntroductionDocument155 pagesThesis IntroductionSravani PeddagangannagariNo ratings yet
- EOSINOFILIADocument23 pagesEOSINOFILIAMarcoNo ratings yet
- Sdr. APHLDocument12 pagesSdr. APHLmarinaNo ratings yet
- Lupus Nephritis ThesisDocument6 pagesLupus Nephritis ThesisWriteMyPaperReviewsSouthBend100% (2)
- Linfoma Conjuntival 2023Document12 pagesLinfoma Conjuntival 2023Miguel HernandezNo ratings yet
- Identification and Management of Lupus Nephritis: An OverviewDocument6 pagesIdentification and Management of Lupus Nephritis: An OverviewEvaliaRahmatPuzianNo ratings yet
- Clinical Review: Systemic Lupus ErythematosusDocument5 pagesClinical Review: Systemic Lupus ErythematosusVijeyachandhar DorairajNo ratings yet
- LimfadenopatiDocument8 pagesLimfadenopatiZulkarnain PrakosoNo ratings yet
- NHL BaileyDocument26 pagesNHL BaileyFitria WaffiNo ratings yet
- Acute Lymphoblastic Leukaemia ArticleDocument10 pagesAcute Lymphoblastic Leukaemia ArticleDiego Fernando Ortiz TenorioNo ratings yet
- Primary Intraocular Lymphoma: SciencedirectDocument14 pagesPrimary Intraocular Lymphoma: Sciencedirectryan enotsNo ratings yet
- Management of Lupus Nephritis: Clinical MedicineDocument11 pagesManagement of Lupus Nephritis: Clinical MedicineLuna Ivanka Al FatihNo ratings yet
- Feline Alimentary Lymphoma2Document11 pagesFeline Alimentary Lymphoma2Mr. questionNo ratings yet
- Applied Therapeutic Koda Kimble 10e 2012 - 1Document6 pagesApplied Therapeutic Koda Kimble 10e 2012 - 1Tinsy ClaudiaNo ratings yet
- Myelodysplastic Syndromes SeminarDocument14 pagesMyelodysplastic Syndromes SeminarAdriian PortilloNo ratings yet
- Pediatrik LeukemiasDocument14 pagesPediatrik LeukemiasLefrina GusrianiiNo ratings yet
- Laboratory Diagnosis of Autoimmune DiseasesDocument6 pagesLaboratory Diagnosis of Autoimmune DiseasesYustina BubnovaNo ratings yet
- Lupus Research PaperDocument5 pagesLupus Research Paperttdqgsbnd100% (3)
- Hematological Abnormalities in SLE Patients at SMCH HospitalDocument1 pageHematological Abnormalities in SLE Patients at SMCH HospitalNATHANAEL SUNGTENo ratings yet
- Chronic Lymphocytic Leukemia Present StatusDocument18 pagesChronic Lymphocytic Leukemia Present StatusLhOi ParagasNo ratings yet
- Lupus Full PDFDocument12 pagesLupus Full PDFEzza noerNo ratings yet
- 4092 24437 1 PBDocument13 pages4092 24437 1 PBCloudcynaraaNo ratings yet
- Encefalitis autoinmune Clínica y Avances en BiologíaDocument14 pagesEncefalitis autoinmune Clínica y Avances en BiologíaalmarazneurologiaNo ratings yet
- DownloadDocument3 pagesDownloadbesttiktokfindsshopNo ratings yet
- Clinicopathologic Analysis of VerDocument27 pagesClinicopathologic Analysis of Versandip ghoseNo ratings yet
- CIDP Adn CaDocument9 pagesCIDP Adn CaabelNo ratings yet
- Lipedema - Is Not Lymphedema: A Review of Current LiteratureDocument9 pagesLipedema - Is Not Lymphedema: A Review of Current LiteraturePutra WaspadaNo ratings yet
- Chronic Lymphocytic LeukemiaFrom EverandChronic Lymphocytic LeukemiaMichael HallekNo ratings yet
- Lower Extremity AmputationsDocument9 pagesLower Extremity AmputationsAisyah DewiNo ratings yet
- Indonesia Improves MDR-TB Detection, Enrollment and TreatmentDocument35 pagesIndonesia Improves MDR-TB Detection, Enrollment and TreatmentAisyah DewiNo ratings yet
- Gallstonepancreatitis:: A ReviewDocument24 pagesGallstonepancreatitis:: A ReviewAisyah DewiNo ratings yet
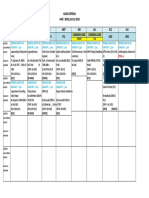
- RSUD Dr. Soetomo Surabaya operating scheduleDocument1 pageRSUD Dr. Soetomo Surabaya operating scheduleAisyah DewiNo ratings yet
- ICD9CMDocument470 pagesICD9CMBayyinah ArdianNo ratings yet
- 9Document1 page9Aisyah DewiNo ratings yet
- EspenDocument235 pagesEspenAisyah DewiNo ratings yet
- The correct answer is d) All of the aboveDocument63 pagesThe correct answer is d) All of the aboveAisyah DewiNo ratings yet
- Droste 2007Document4 pagesDroste 2007Aisyah DewiNo ratings yet
- Acute Limb IschemiaDocument11 pagesAcute Limb IschemiamarisahanaNo ratings yet
- Ossifying Fibroma: An Uncommon Differential Diagnosis For T2-Hypointense Sinonasal MassesDocument5 pagesOssifying Fibroma: An Uncommon Differential Diagnosis For T2-Hypointense Sinonasal MassesAisyah DewiNo ratings yet
- ICD10Volume2 en 2010Document201 pagesICD10Volume2 en 2010Ai NurfaiziyahNo ratings yet
- CeaDocument4 pagesCeaAisyah DewiNo ratings yet
- Acara Operasi Hari: Senin, 16 Juli 2018Document1 pageAcara Operasi Hari: Senin, 16 Juli 2018Aisyah DewiNo ratings yet
- Daftar Pustaka CatatanDocument3 pagesDaftar Pustaka CatatanAisyah DewiNo ratings yet
- Intra Abdominal DrainDocument5 pagesIntra Abdominal DrainAisyah DewiNo ratings yet
- Daftar Pustaka Tiroiditis RiedelDocument1 pageDaftar Pustaka Tiroiditis RiedelAisyah DewiNo ratings yet
- DocumentDocument13 pagesDocumentAisyah DewiNo ratings yet
- ICD-10 2010 Volume 1 & 3Document1,999 pagesICD-10 2010 Volume 1 & 3aprilNo ratings yet
- Pediatric Risk of Mortality III Score Dan Paediatric Index of Mortality 3Document3 pagesPediatric Risk of Mortality III Score Dan Paediatric Index of Mortality 3Aisyah DewiNo ratings yet
- DocumentDocument7 pagesDocumentAisyah DewiNo ratings yet
- Biosecurity Benefits Poultry FarmingDocument3 pagesBiosecurity Benefits Poultry FarmingsudheerpulaNo ratings yet
- Communicable and Non CommunicableDocument29 pagesCommunicable and Non CommunicableAkinpelu JoyNo ratings yet
- Risk Factors For Surgical Site InfectionDocument5 pagesRisk Factors For Surgical Site InfectionElizabeth Mautino CaceresNo ratings yet
- 1 en 148 Chapter OnlinePDFConceptsofHolisticHealthCare2016VebntegodtetalDocument8 pages1 en 148 Chapter OnlinePDFConceptsofHolisticHealthCare2016VebntegodtetalSheila ALNo ratings yet
- Haematological Diseases-1Document28 pagesHaematological Diseases-1Kunal DangatNo ratings yet
- Extra Questions 6th September 2020Document3 pagesExtra Questions 6th September 2020random personsaNo ratings yet
- Community Aquired Pneumonia (: Diagnosis CAP) and Current Management Yunita ArliniDocument12 pagesCommunity Aquired Pneumonia (: Diagnosis CAP) and Current Management Yunita ArliniSundas EjazNo ratings yet
- Francisco, Faye Andrea Go BSN 3-BDocument2 pagesFrancisco, Faye Andrea Go BSN 3-BFaye Andrea FranciscoNo ratings yet
- Pediatric Infectious Diseases. Vaccination ProgramsDocument44 pagesPediatric Infectious Diseases. Vaccination ProgramsShubhra PaulNo ratings yet
- The Marketing Experiment of Melody ToffeeDocument13 pagesThe Marketing Experiment of Melody ToffeeRishabh RajNo ratings yet
- First Aid, Emergency Care, and Disaster ManagementDocument7 pagesFirst Aid, Emergency Care, and Disaster Managementsabrina AliNo ratings yet
- Surgical Notes (Teddy)Document88 pagesSurgical Notes (Teddy)shichianNo ratings yet
- PPE Physical Examination Form RevDocument1 pagePPE Physical Examination Form RevCaitlyn KelleherNo ratings yet
- Erdheim-Chester Disease - UpToDateDocument40 pagesErdheim-Chester Disease - UpToDatePepe pepe pepeNo ratings yet
- Childhood Cancer Staging For Population RegistriesDocument64 pagesChildhood Cancer Staging For Population RegistriesMaria MihalachiNo ratings yet
- Flowchart For Assessing Illness in The Absence of The School NurseDocument1 pageFlowchart For Assessing Illness in The Absence of The School NurserahkelpNo ratings yet
- Trichuris Trichiura: Lecture By: Maha Gamal AldeinDocument20 pagesTrichuris Trichiura: Lecture By: Maha Gamal AldeinMohammad DweibNo ratings yet
- Dystonia Fact Sheet: Causes, Symptoms & TreatmentsDocument7 pagesDystonia Fact Sheet: Causes, Symptoms & Treatmentsepiipo91No ratings yet
- Nursing Health History /nursing Process/Physical AsessmentDocument2 pagesNursing Health History /nursing Process/Physical AsessmentKaye CorNo ratings yet
- SRP Practical Endocrinology HarrowerDocument700 pagesSRP Practical Endocrinology HarrowerGuillermo BelliNo ratings yet
- Chemical Pathology 2 - Plasma ProteinsDocument5 pagesChemical Pathology 2 - Plasma ProteinsaNo ratings yet
- Program at A Glance 30th Asmiha, Isci, Ina-Chd - 12oct2021Document13 pagesProgram at A Glance 30th Asmiha, Isci, Ina-Chd - 12oct2021Rizki Anindita MtdNo ratings yet
- Ibuprofen Drug StudyDocument3 pagesIbuprofen Drug StudySeann Loresco100% (2)
- TS Nicaragua Health System RPTDocument74 pagesTS Nicaragua Health System RPTAlcajNo ratings yet
- Use of Silver Nanoparticles in Hiv Treatment Protocols A Research Proposal 2157 7439.1000127Document5 pagesUse of Silver Nanoparticles in Hiv Treatment Protocols A Research Proposal 2157 7439.1000127Wellington TunhiraNo ratings yet
- Oropharyngeal Cancer: Current Understanding and ManagementDocument7 pagesOropharyngeal Cancer: Current Understanding and ManagementbgdNo ratings yet
- Assessment Mouth and Oropharynx LipsDocument8 pagesAssessment Mouth and Oropharynx LipsQuinmarc LimNo ratings yet
- Crohn's Disease Malabsorption: Causes, Symptoms and Nursing CareDocument31 pagesCrohn's Disease Malabsorption: Causes, Symptoms and Nursing Caretatenda chitindiNo ratings yet
- Nephrotic Syndrome in Children: Causes, Symptoms, and TreatmentDocument27 pagesNephrotic Syndrome in Children: Causes, Symptoms, and TreatmentAlokh Saha RajNo ratings yet