You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Módulo 22: Pasivos y Patrimonio: Fundación IFRS: Material de Formación Sobre LaDocument64 pagesMódulo 22: Pasivos y Patrimonio: Fundación IFRS: Material de Formación Sobre LaDAYANA ANDREA DAMS MOLINANo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
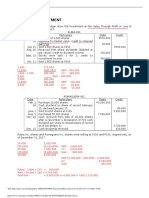
- Audit 2, AUDIT - OF - INVESTMENT - Problem - 2Document2 pagesAudit 2, AUDIT - OF - INVESTMENT - Problem - 2Shaz NagaNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- OpenMind 2 Unit 6 Wordlist SpanishDocument8 pagesOpenMind 2 Unit 6 Wordlist SpanishDaniel CarreónNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- International Vision Zero' Conference On Occupational Safety and HealthDocument9 pagesInternational Vision Zero' Conference On Occupational Safety and Healthjacobpm2010No ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Practice: 1. Suppose There Is A Perfectly Competitive Industry Where All The Firms AreDocument10 pagesPractice: 1. Suppose There Is A Perfectly Competitive Industry Where All The Firms Aremaddie isnt realNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Pros Sagssago Notes in Criminal Law 2017 EditionDocument316 pagesPros Sagssago Notes in Criminal Law 2017 EditionLEIGH100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Art Appreciation - UPDATEDDocument3 pagesArt Appreciation - UPDATEDJeffrey SiyNo ratings yet
- International Marketing ProjectDocument20 pagesInternational Marketing ProjectVikaNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Unit No: 09 Cable StructuresDocument34 pagesUnit No: 09 Cable StructuresRoman BaralNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Joe Lewis ATTU 2012-10 PDFDocument3 pagesJoe Lewis ATTU 2012-10 PDFBudo MediaNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Physioex Activity 1Document6 pagesPhysioex Activity 1Rara ArifahNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Downloaded From Manuals Search EngineDocument79 pagesDownloaded From Manuals Search EngineEmiliano Roberto Arocha CorsoNo ratings yet
- Infinity Astrological Magazine Inf10 2016 by Infinity Astrological MagazineDocument163 pagesInfinity Astrological Magazine Inf10 2016 by Infinity Astrological MagazineCern GabrielNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Psychology of Chess MistakesDocument5 pagesPsychology of Chess MistakesMunkhjargal MJ50% (2)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Estimation and ProblemsDocument18 pagesEstimation and ProblemsAyush SonthaliaNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Review of Camarines Norte FolkdancesDocument5 pagesReview of Camarines Norte FolkdancesMillenjoy MorenoNo ratings yet
- New and Used Toyota Tacoma Cars For Sale in CambodiaDocument1 pageNew and Used Toyota Tacoma Cars For Sale in CambodiaNhek VireakNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Lower Extremity Reconstruction Plastic SurgeryDocument65 pagesLower Extremity Reconstruction Plastic SurgeryJuan MoscaNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Urey James Alqueza Grade 12 STEM MarineDocument6 pagesUrey James Alqueza Grade 12 STEM MarineChristian BlantucasNo ratings yet
- Travel Standard 2019 SLB-SCS-S002Document17 pagesTravel Standard 2019 SLB-SCS-S002Reza BorahNo ratings yet
- Muhammad Hasnain: Al-Ghazi General Store Near Abdullah Hospital Skardu Cell Phone No: +92-3444584033Document3 pagesMuhammad Hasnain: Al-Ghazi General Store Near Abdullah Hospital Skardu Cell Phone No: +92-3444584033Muhammad HasnainNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Annex 4C Affidavit of UndertakingDocument2 pagesAnnex 4C Affidavit of UndertakingSometimes goodNo ratings yet
- 1 English1Document3 pages1 English1Andreea Lavinia BucataruNo ratings yet
- Logical Reasoning: Puzzle Test (Exercise: B)Document12 pagesLogical Reasoning: Puzzle Test (Exercise: B)satish kumarNo ratings yet
- 4-Delacon Connection 2019 - Protenga-V4Document34 pages4-Delacon Connection 2019 - Protenga-V4Derza MuljadiNo ratings yet
- Reza Shirmarz CV in EnglishDocument13 pagesReza Shirmarz CV in EnglishReza ShirmarzNo ratings yet
- Gazette No. 68, ChocolateDocument8 pagesGazette No. 68, ChocolateMihaela BarbulescuNo ratings yet
- Eerie Images - Decans in Horary - Nina GryphonDocument3 pagesEerie Images - Decans in Horary - Nina GryphonMarco SatoriNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Edgar Allan PoeDocument12 pagesEdgar Allan PoeFlorencia GarciaNo ratings yet
- Computer Architecture: Dr. M. Moustafa Hassan Elec. Power EngineeringDocument23 pagesComputer Architecture: Dr. M. Moustafa Hassan Elec. Power EngineeringjgjghNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)