You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- SYNERGY Fake Job Offer LetterDocument5 pagesSYNERGY Fake Job Offer LetterSyed's Way PoolNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- MDR - Conformity AssessmentDocument8 pagesMDR - Conformity AssessmentNathan LabordeNo ratings yet
- Contract Management ChecklistDocument15 pagesContract Management ChecklistCreanga Georgian100% (1)
- Chapter 9 - Firewalls and Intrusion Detection SystemDocument8 pagesChapter 9 - Firewalls and Intrusion Detection SystemJasminNo ratings yet
- Ruego Vs People - Physical InjuriesDocument10 pagesRuego Vs People - Physical Injuriesmldmolina75No ratings yet
- 4 Sem C.T Unit 3 Water Cement RatioDocument4 pages4 Sem C.T Unit 3 Water Cement RatioToufiq BhatiNo ratings yet
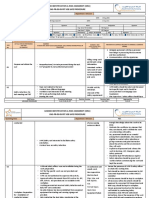
- OHS-PR-09-03-F07 JOB SAFE PROCEDURE (19) Installation of Conductor JumperDocument14 pagesOHS-PR-09-03-F07 JOB SAFE PROCEDURE (19) Installation of Conductor Jumpermohammed tofiqNo ratings yet
- Mycology 1 PrelimDocument4 pagesMycology 1 PrelimKaye Angel VillonNo ratings yet
- Short Tricks To Remember GK EasilyDocument3 pagesShort Tricks To Remember GK EasilyManoj KiningeNo ratings yet
- Lymph Node - Any of The Small, Oval or Round Bodies, Located Along The Lymphatic VesselsDocument2 pagesLymph Node - Any of The Small, Oval or Round Bodies, Located Along The Lymphatic VesselsKaren ParraNo ratings yet
- Tyler Resume Updated 3 23 17Document1 pageTyler Resume Updated 3 23 17api-285213449No ratings yet
- GSM Network SDCCH Congestion & Solutions-16Document15 pagesGSM Network SDCCH Congestion & Solutions-16abdullaaNo ratings yet
- Isagenix Isalean Shake Vs Visalus Shake 5 16 12Document8 pagesIsagenix Isalean Shake Vs Visalus Shake 5 16 12api-150110825No ratings yet
- Concise Encyclopedia of Temperate Tree Fruit Singha BasraDocument389 pagesConcise Encyclopedia of Temperate Tree Fruit Singha Basratibi_pl2005100% (6)
- Introduction To Chemical BondingDocument5 pagesIntroduction To Chemical BondingMini PGNo ratings yet
- 4099 0002Document4 pages4099 0002kikeecpNo ratings yet
- The Current Status of The "Food Security Doctrine" Implementation in The Russian Federation and Tasks For 2013-2020Document5 pagesThe Current Status of The "Food Security Doctrine" Implementation in The Russian Federation and Tasks For 2013-2020gautham28No ratings yet
- KFCDocument41 pagesKFCSumit Kumar100% (1)
- Nutrition Through-Out Lifespan (Infancy)Document37 pagesNutrition Through-Out Lifespan (Infancy)Vincent Maralit MaterialNo ratings yet
- Short EssayDocument2 pagesShort EssayMary Jane RiparipNo ratings yet
- Sulfato de Zinc MsdsDocument5 pagesSulfato de Zinc MsdsTomas Gaviria MartinezNo ratings yet
- Airo WaterDocument27 pagesAiro WaterAhana SahaNo ratings yet
- Death Claim Form Early - English - Hindi - 05112019Document9 pagesDeath Claim Form Early - English - Hindi - 05112019CHATTU HALDERNo ratings yet
- BancassuranceDocument53 pagesBancassuranceSonali Chaubey0% (1)
- ScoliosisDocument3 pagesScoliosisTracy100% (1)
- Types of CompressorsDocument44 pagesTypes of Compressorsjezreeleda.limNo ratings yet
- System 4 Med G 7831 - PG 85362Document76 pagesSystem 4 Med G 7831 - PG 85362jerimiah_manzonNo ratings yet
- Hosp DimDocument3 pagesHosp DimJoe ThesecondmonthNo ratings yet
- Deltaweld 453 MilDocument40 pagesDeltaweld 453 MilHugo RodriguezNo ratings yet
- 7 Advertising - AirDocument1 page7 Advertising - Airaletzring@innovectra.comNo ratings yet