You might also like
- How To Benefit From Everyday HerbsDocument167 pagesHow To Benefit From Everyday HerbsGarcia Abdullah100% (19)
- The HDL Handbook: Biological Functions and Clinical ImplicationsFrom EverandThe HDL Handbook: Biological Functions and Clinical ImplicationsNo ratings yet
- Antimicrobial Herb and Spice Compounds in FoodDocument20 pagesAntimicrobial Herb and Spice Compounds in FoodPrabowo SuryaningtyasNo ratings yet
- Lipitor WorksheetDocument2 pagesLipitor WorksheetMichael Kuzbyt100% (4)
- Complementary and Alternative Medical Lab Testing Part 8: UrologyFrom EverandComplementary and Alternative Medical Lab Testing Part 8: UrologyRating: 3 out of 5 stars3/5 (1)
- The Egyptian Heart Journal: Haitham Galal Mohammed, Adel Mohamed ShabanaDocument6 pagesThe Egyptian Heart Journal: Haitham Galal Mohammed, Adel Mohamed ShabanaDaniel Zagoto100% (1)
- BIOS LIFE - Cleveland Clinic Trial by Dr. Dennis SprecherDocument5 pagesBIOS LIFE - Cleveland Clinic Trial by Dr. Dennis SprecherHisWellnessNo ratings yet
- Medical Technology Board Exam Reviewer 1: CLINICAL CHEMISTRY ReviewDocument4 pagesMedical Technology Board Exam Reviewer 1: CLINICAL CHEMISTRY ReviewLyudmyla Gillego100% (1)
- Low-Dose Rosuvastatin Improves Lipids in Type 2 DiabetesDocument11 pagesLow-Dose Rosuvastatin Improves Lipids in Type 2 DiabetesZahid MahmoodNo ratings yet
- Omega 3Document8 pagesOmega 3Mireya AlejandraNo ratings yet
- Milaaaaaaa FDocument12 pagesMilaaaaaaa F200742 Elya AmaliaNo ratings yet
- Ezetimibe - A Novel Add On Treatment Strategy To Achieve Targeted LDL in Patients With Uncontrolled LDL Levels On High Dose Statin AloneDocument9 pagesEzetimibe - A Novel Add On Treatment Strategy To Achieve Targeted LDL in Patients With Uncontrolled LDL Levels On High Dose Statin AloneEditor ERWEJNo ratings yet
- j3 2010Document12 pagesj3 2010Taha FransNo ratings yet
- To Compare Rosuvastatin With Atorvastatin in Terms of Mean Change in LDL C in Patient With Diabetes PDFDocument7 pagesTo Compare Rosuvastatin With Atorvastatin in Terms of Mean Change in LDL C in Patient With Diabetes PDFJez RarangNo ratings yet
- DiabegardDocument6 pagesDiabegardmlteenNo ratings yet
- Kumarsingh 2017Document15 pagesKumarsingh 2017Quoc HuyNo ratings yet
- Lipid-Modifying Effects of NutraceuticalsDocument14 pagesLipid-Modifying Effects of NutraceuticalsBlanca MezaNo ratings yet
- Study of Plasma Level of Atorvastatin and Its Effect On Lipid ProfileDocument10 pagesStudy of Plasma Level of Atorvastatin and Its Effect On Lipid Profileheema valeraNo ratings yet
- Evaluate The Efficacy of Simvastatin and Fluvastatin in Patients With Hypercholesterolemia and Their Effect On Liver FunctionsDocument5 pagesEvaluate The Efficacy of Simvastatin and Fluvastatin in Patients With Hypercholesterolemia and Their Effect On Liver FunctionsfiqaalkasieNo ratings yet
- Effects of Poly-Herbal Tablet As Herbal Medicine On Lipid LevelDocument5 pagesEffects of Poly-Herbal Tablet As Herbal Medicine On Lipid LevelLiliNurmawatiNo ratings yet
- Nursing Research PresentaionDocument33 pagesNursing Research Presentaionapi-300699057No ratings yet
- Pharmaceutical SciencesDocument5 pagesPharmaceutical SciencesiajpsNo ratings yet
- Effect of Adherence To Lipid Profiles of Dyslipidemia Patients A Case Study at A Pharmacy Service in MedanDocument5 pagesEffect of Adherence To Lipid Profiles of Dyslipidemia Patients A Case Study at A Pharmacy Service in MedanInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- International Journal of Nursing and Health Services (IJNHS)Document11 pagesInternational Journal of Nursing and Health Services (IJNHS)Medianto C.PNo ratings yet
- Accepted For Publication October 14, 2017. 0149-2918/$ - See Front Matter & 2017 Elsevier HS Journals, Inc. All Rights ReservedDocument14 pagesAccepted For Publication October 14, 2017. 0149-2918/$ - See Front Matter & 2017 Elsevier HS Journals, Inc. All Rights ReservedDianne GalangNo ratings yet
- European Journal of Biomedical AND Pharmaceutical SciencesDocument11 pagesEuropean Journal of Biomedical AND Pharmaceutical Sciencesrafiqa banoNo ratings yet
- Yousef I 2020Document9 pagesYousef I 2020Gabriel GursenNo ratings yet
- Paper Title: (16 Bold)Document9 pagesPaper Title: (16 Bold)vegeto portmanNo ratings yet
- AnnotationsDocument3 pagesAnnotationsAegina FestinNo ratings yet
- MIRA KESUMA - Tugas Resume Jurnal - TEBDocument9 pagesMIRA KESUMA - Tugas Resume Jurnal - TEBksm vlogNo ratings yet
- The Effects of Long-Term Dietary Therapy On Patients With HypertriglyceridemiaDocument11 pagesThe Effects of Long-Term Dietary Therapy On Patients With Hypertriglyceridemiaraul zea calcinaNo ratings yet
- New England Journal Medicine: The ofDocument5 pagesNew England Journal Medicine: The ofAri Hidriansyah AtmajaNo ratings yet
- NursingresearchreportDocument12 pagesNursingresearchreportapi-300699057No ratings yet
- Clinical Trial 2016Document11 pagesClinical Trial 2016guugle gogleNo ratings yet
- Serum Ischemia Modified Albumin, Fibrinogen, HSCRP in DMT2 With and Without HypertensionDocument9 pagesSerum Ischemia Modified Albumin, Fibrinogen, HSCRP in DMT2 With and Without HypertensionMarcellia AngelinaNo ratings yet
- Dislipidemia en Pacientes TargaJIAS-17-19004Document5 pagesDislipidemia en Pacientes TargaJIAS-17-19004angelvpsNo ratings yet
- 2017 Article 551Document11 pages2017 Article 551Albert EdoNo ratings yet
- A Nutraceutical Combination Improves Insulin Sensitivity in Patients With Metabolic SyndromeDocument7 pagesA Nutraceutical Combination Improves Insulin Sensitivity in Patients With Metabolic SyndromegiannidietNo ratings yet
- Subclinical Hypothyroidism Linked to Lipid and Oxidative Stress IssuesDocument10 pagesSubclinical Hypothyroidism Linked to Lipid and Oxidative Stress IssuesJawaid AhmedNo ratings yet
- Stratified Treatment of HypertensionDocument7 pagesStratified Treatment of HypertensionMohamad MuntahaNo ratings yet
- Hari 2018Document11 pagesHari 2018rahmansetiawanajaNo ratings yet
- Anethum Graveolens and Hyperlipidemia: A Randomized Clinical TrialDocument4 pagesAnethum Graveolens and Hyperlipidemia: A Randomized Clinical TrialdhiyarahadianNo ratings yet
- Risk Factors For Coronary Heart Disease in Type Ii Diabetes MellitusDocument6 pagesRisk Factors For Coronary Heart Disease in Type Ii Diabetes MellitusmahalNo ratings yet
- Jurnal Herbal Ajikwa Ari WidiantoDocument6 pagesJurnal Herbal Ajikwa Ari WidiantoFarah AkhwanisNo ratings yet
- DioscinDocument15 pagesDioscinpaulo saNo ratings yet
- Dislipidemia Dan CardiovasculerDocument2 pagesDislipidemia Dan CardiovasculerWahyuningsih HamidNo ratings yet
- 2 DyslipidemiaDocument7 pages2 DyslipidemiaShengyou ZengNo ratings yet
- Paper TemplateDocument10 pagesPaper Templatenur hidayatNo ratings yet
- Effectiveness and Safety of Inclisiran In.42Document8 pagesEffectiveness and Safety of Inclisiran In.42Guillermo CenturionNo ratings yet
- Paper Title: (16 Bold Blue Color)Document9 pagesPaper Title: (16 Bold Blue Color)Fauzi RusdiantoNo ratings yet
- Pancreatic Fat Deposition Is Increased and Related To Beta Cell Function in Women With Familial Partial LipodystrophyDocument6 pagesPancreatic Fat Deposition Is Increased and Related To Beta Cell Function in Women With Familial Partial LipodystrophyThiago AlfradiqueNo ratings yet
- JCDR 11 FC01Document5 pagesJCDR 11 FC01Manmohan SinghNo ratings yet
- Researcharticle Open Access: Mahdieh Abbasalizad Farhangi, Parvin Dehghan, Siroos Tajmiri and Mehran Mesgari AbbasiDocument9 pagesResearcharticle Open Access: Mahdieh Abbasalizad Farhangi, Parvin Dehghan, Siroos Tajmiri and Mehran Mesgari AbbasilolaNo ratings yet
- Green Cardamom... Improves Serum Irisin, Glucose Indices, and Lipid Profiles In... Non-Alcoholic Fatty Liver Disease Patients ...Document11 pagesGreen Cardamom... Improves Serum Irisin, Glucose Indices, and Lipid Profiles In... Non-Alcoholic Fatty Liver Disease Patients ...Daniel GilbertoNo ratings yet
- Antihyperlipidemic Activity of Chloroxylon Swietenia in Triton WR1339 Induced HyperlipidemiaDocument7 pagesAntihyperlipidemic Activity of Chloroxylon Swietenia in Triton WR1339 Induced HyperlipidemiaDharmendra SawNo ratings yet
- A Systematic Review and Meta-Analysis of Ayurvedic Herbal Preparations For HypercholesterolemiaDocument24 pagesA Systematic Review and Meta-Analysis of Ayurvedic Herbal Preparations For HypercholesterolemiaSotiris AnagnostopoulosNo ratings yet
- 5 - Diabetes MellitusDocument9 pages5 - Diabetes MellitusNatnicha foongfaNo ratings yet
- Research Open Access: Ruscica Et Al. Nutrition Journal (2019) 18:13Document9 pagesResearch Open Access: Ruscica Et Al. Nutrition Journal (2019) 18:13Fatamorgana AbdullahNo ratings yet
- Roles of Plasma Leptin and Resistin in Novel Subgroup of T2DM - Cluster AnalysisDocument10 pagesRoles of Plasma Leptin and Resistin in Novel Subgroup of T2DM - Cluster AnalysisShayekh M ArifNo ratings yet
- Clinical ResearchDocument6 pagesClinical Researchnurul wahyuniNo ratings yet
- Original Article Evaluation of Dyslipidaemia in Type 2 Diabetes Mellitus PatientsDocument6 pagesOriginal Article Evaluation of Dyslipidaemia in Type 2 Diabetes Mellitus PatientsEnvhy AmaliaNo ratings yet
- L Carnosine in DiabetesDocument11 pagesL Carnosine in DiabetesVivekNo ratings yet
- Efficacy and Safety of High-Density Lipoprotein Cholesterol-Increasing CompoundsDocument13 pagesEfficacy and Safety of High-Density Lipoprotein Cholesterol-Increasing CompoundsAdityasekar WangiNo ratings yet
- Evaluation and Comparison of Hypolipidemic Effect of Curcuma Longa Linn. With Atorvastatin in Albino RatsDocument5 pagesEvaluation and Comparison of Hypolipidemic Effect of Curcuma Longa Linn. With Atorvastatin in Albino Ratsaghsal novanNo ratings yet
- Journal Appraisal 1Document7 pagesJournal Appraisal 1Norjetalexis Maningo CabreraNo ratings yet
- Medi 97 E0255Document8 pagesMedi 97 E0255Dhanang Prawira NugrahaNo ratings yet
- 3023 6565 2 PB PDFDocument5 pages3023 6565 2 PB PDFpopy AinunNo ratings yet
- At Some ConcentrationsDocument7 pagesAt Some ConcentrationsDewi nur thohidahNo ratings yet
- Comparative Study of Atorvastatin and RosuvastatinDocument8 pagesComparative Study of Atorvastatin and RosuvastatinDewi nur thohidahNo ratings yet
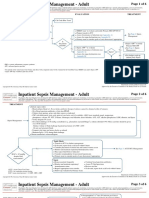
- Inpatient Sepsis Management - Adult: Page 1 of 6Document6 pagesInpatient Sepsis Management - Adult: Page 1 of 6Dewi nur thohidahNo ratings yet
- Advpub Ess14061Document10 pagesAdvpub Ess14061Dewi nur thohidahNo ratings yet
- Chronic Kidney Disease Stage V: (Laporan Kasus)Document5 pagesChronic Kidney Disease Stage V: (Laporan Kasus)Alif Fabri OktanoNo ratings yet
- Https FarterDocument1 pageHttps FarterDewi nur thohidahNo ratings yet
- Anti-Inflammatory Activity of Medicinal Plants A ReviewDocument10 pagesAnti-Inflammatory Activity of Medicinal Plants A ReviewDewi nur thohidahNo ratings yet
- Extraction and Evaluation of Piperine From Piper Nigrum Linn.Document6 pagesExtraction and Evaluation of Piperine From Piper Nigrum Linn.Dewi nur thohidahNo ratings yet
- Chronic Kidney Disease Stage V: (Laporan Kasus)Document5 pagesChronic Kidney Disease Stage V: (Laporan Kasus)Alif Fabri OktanoNo ratings yet
- Parametric Optimization of Microwave Reflux Extraction of Spice Oleoresin From White Pepper (Piper Nigrum)Document8 pagesParametric Optimization of Microwave Reflux Extraction of Spice Oleoresin From White Pepper (Piper Nigrum)Dewi nur thohidahNo ratings yet
- Recognize and Treatment of Digitalis Intoxication: Case ReportDocument6 pagesRecognize and Treatment of Digitalis Intoxication: Case ReportKilroy Vincent SterlingNo ratings yet
- Antimicrobial Activity of SpicesDocument55 pagesAntimicrobial Activity of SpicesDewi nur thohidahNo ratings yet
- INJEKSI LARUTAN SODIUM DIKLOFENAKDocument35 pagesINJEKSI LARUTAN SODIUM DIKLOFENAKDewi nur thohidahNo ratings yet
- 1 PBDocument11 pages1 PBDewi nur thohidahNo ratings yet
- Antimicrobial Activity of SpicesDocument55 pagesAntimicrobial Activity of SpicesDewi nur thohidahNo ratings yet
- Nutmeg's (Myristica Fragrans Houtt) Oleoresin Effect of Heating To Chemical Compositions and Antifungal PropertiesDocument11 pagesNutmeg's (Myristica Fragrans Houtt) Oleoresin Effect of Heating To Chemical Compositions and Antifungal PropertiesDewi nur thohidahNo ratings yet
- JurnalDocument9 pagesJurnalYanuar Ahsan OfficialNo ratings yet
- Peningkatan Kualitas Lada Putih Dengan Kombinasi LamaDocument9 pagesPeningkatan Kualitas Lada Putih Dengan Kombinasi LamaDewi nur thohidahNo ratings yet
- Antimicrobial Activity of SpicesDocument55 pagesAntimicrobial Activity of SpicesDewi nur thohidahNo ratings yet
- ParkinsonDocument9 pagesParkinsonDaniel OctavianusNo ratings yet
- Extraction and Evaluation of Piperine From Piper Nigrum Linn.Document6 pagesExtraction and Evaluation of Piperine From Piper Nigrum Linn.Dewi nur thohidahNo ratings yet
- Anti-Obesity Efficacy of Nanoemulsion OleoresinDocument10 pagesAnti-Obesity Efficacy of Nanoemulsion OleoresinDewi nur thohidahNo ratings yet
- A Review On Potential Families of Anti-Inflammatory ActivityDocument15 pagesA Review On Potential Families of Anti-Inflammatory ActivityDewi nur thohidahNo ratings yet
- HFHS CKD V6Document76 pagesHFHS CKD V6medicalNo ratings yet
- Parametric Optimization of Microwave Reflux Extraction of Spice Oleoresin From White Pepper (Piper Nigrum)Document8 pagesParametric Optimization of Microwave Reflux Extraction of Spice Oleoresin From White Pepper (Piper Nigrum)Dewi nur thohidahNo ratings yet
- Chronic Kidney Disease Stage V: (Laporan Kasus)Document5 pagesChronic Kidney Disease Stage V: (Laporan Kasus)Alif Fabri OktanoNo ratings yet
- Anti-Inflammatory Activity of Medicinal Plants A ReviewDocument10 pagesAnti-Inflammatory Activity of Medicinal Plants A ReviewDewi nur thohidahNo ratings yet
- Final ProjectDocument119 pagesFinal ProjectSaurabh KumarNo ratings yet
- Assignment 3.1 - LipidsDocument4 pagesAssignment 3.1 - LipidsJameseu KimNo ratings yet
- 7 - Clinical ChemistryDocument13 pages7 - Clinical ChemistryMary CabalceNo ratings yet
- Effect of Garlic Black Pepper and Hot ReDocument13 pagesEffect of Garlic Black Pepper and Hot ReŠhâh NawazNo ratings yet
- IM Group Case Report 2020Document183 pagesIM Group Case Report 2020Mary Ruth Aujero Sanchez-BenzonNo ratings yet
- Fenugreek As Dietary FibreDocument4 pagesFenugreek As Dietary FibrePriyadarshini Mh100% (2)
- Influence of Aerobic Exercise Training On Cardiovascular and Endocrine Inflammatory Biomarkers in Hypertensive Postmenopausal WomenDocument7 pagesInfluence of Aerobic Exercise Training On Cardiovascular and Endocrine Inflammatory Biomarkers in Hypertensive Postmenopausal WomenNemo SecretNo ratings yet
- ILIBDocument8 pagesILIBleonardocaldasvieiraNo ratings yet
- Pugud Samodro - Insulin Resistance and Metabolic SyndromeDocument32 pagesPugud Samodro - Insulin Resistance and Metabolic SyndromeReiza Primayana VigNo ratings yet
- The Impacts of Electrolyte Drink and TapDocument38 pagesThe Impacts of Electrolyte Drink and TapJoshua VidalNo ratings yet
- Atherosclerosis: Reporter: Collera, Charissa Constantino, Venice Clemena, Adnan Coronel, Romeo Cordova, KarlaDocument73 pagesAtherosclerosis: Reporter: Collera, Charissa Constantino, Venice Clemena, Adnan Coronel, Romeo Cordova, Karlaprecious_bustosNo ratings yet
- Department of Biochemistry: Test Name Value Unit Bio. Ref IntervalDocument18 pagesDepartment of Biochemistry: Test Name Value Unit Bio. Ref IntervalTabitha MartynNo ratings yet
- National Nutrition and Health Sur Vey (Nnhes) : Atherosclerosis - Related Diseases and Risk FactorsDocument11 pagesNational Nutrition and Health Sur Vey (Nnhes) : Atherosclerosis - Related Diseases and Risk FactorsGene Alfonso BanawaNo ratings yet
- Cardiac Function Tests GuideDocument35 pagesCardiac Function Tests GuideChandana Padma Priya JuturNo ratings yet
- Post Guidelines - June 16Document52 pagesPost Guidelines - June 16kevin clone1No ratings yet
- Week 6Document37 pagesWeek 6Wong ChocolateNo ratings yet
- Heart AttackDocument12 pagesHeart AttackPaul NeedhamNo ratings yet
- Garlic Benefits - Can Garlic Lower Your Cholesterol?Document4 pagesGarlic Benefits - Can Garlic Lower Your Cholesterol?Jipson VargheseNo ratings yet
- Effects of Juglans Nigra (Black Walnut) and Urtica Dioica (Nettle Leaf) On Lipid Profile of Thiamazole Induced Hypothyroidism in Obese Wistar Albino RatsDocument78 pagesEffects of Juglans Nigra (Black Walnut) and Urtica Dioica (Nettle Leaf) On Lipid Profile of Thiamazole Induced Hypothyroidism in Obese Wistar Albino RatsVictor SamuelNo ratings yet
- Pathology and Pathophysiology ALL+QUIZDocument235 pagesPathology and Pathophysiology ALL+QUIZomer.buzagloNo ratings yet
- Introduction to Clinical ChemistryDocument4 pagesIntroduction to Clinical ChemistryAllyah Ross DuqueNo ratings yet
- Sick and TiredDocument24 pagesSick and TiredVaradrajan MudliyarNo ratings yet
- Cesar - Cardio & HemaDocument77 pagesCesar - Cardio & HemakdfhjfhfNo ratings yet
- Therapeutic Potential of Murraya Koenigii in Dyslipidemia:A ReviewDocument5 pagesTherapeutic Potential of Murraya Koenigii in Dyslipidemia:A ReviewMamta ParnamiNo ratings yet
- Fernandes, 2023 PDFDocument5 pagesFernandes, 2023 PDFFani araujoNo ratings yet