You might also like
- Exam 2 Study Guide-2Document5 pagesExam 2 Study Guide-2Enoch SuhNo ratings yet
- Concepts of Infection ControlDocument53 pagesConcepts of Infection ControlPak Pandir0% (1)
- Chapter 12 Healthcare EpidemiologyDocument10 pagesChapter 12 Healthcare EpidemiologyRegiena Tamargo100% (1)
- H-Mole Chapter I-VDocument103 pagesH-Mole Chapter I-VJoevence Gazo CuaresmaNo ratings yet
- Dark Winter: Operation Dark Winter Was The Code Name For A Senior-Level Bio-Terrorist AttackDocument5 pagesDark Winter: Operation Dark Winter Was The Code Name For A Senior-Level Bio-Terrorist AttackJosephNo ratings yet
- Nicotine - It May Have A Good Side - Harvard HealthDocument3 pagesNicotine - It May Have A Good Side - Harvard HealthzimkoNo ratings yet
- Biostatistic and Epidemiology Lecture NoteDocument66 pagesBiostatistic and Epidemiology Lecture Notefff100% (3)
- Infection Control & Safety Standards in IcuDocument59 pagesInfection Control & Safety Standards in IcuHebsiba PonnayyanNo ratings yet
- NOTES CD Lecture Generic 2022Document182 pagesNOTES CD Lecture Generic 2022Meryville JacildoNo ratings yet
- Guide To Infection Control in The Hospital: Isolation of Communicable DiseasesDocument17 pagesGuide To Infection Control in The Hospital: Isolation of Communicable DiseasesColleen CalditoNo ratings yet
- EN20 BNC L1a 20200909Document95 pagesEN20 BNC L1a 20200909Carol LeeNo ratings yet
- Basic Microbiology For 2014 Ver1Document27 pagesBasic Microbiology For 2014 Ver1Dr. Mussa QamerNo ratings yet
- 29 Nursing Management of Communicable DiseaseDocument79 pages29 Nursing Management of Communicable DiseaseMonika SanaaNo ratings yet
- Guide To Infection Control in The Hospital: Isolation of Communicable DiseasesDocument17 pagesGuide To Infection Control in The Hospital: Isolation of Communicable DiseasesMatt ryioNo ratings yet
- Chapter 12Document35 pagesChapter 12BRENDHIL PACIFICO CRUZNo ratings yet
- Nosocomial InfectionDocument30 pagesNosocomial InfectionDivyeshkumar GanvitNo ratings yet
- Infeksi NosokomialDocument29 pagesInfeksi NosokomialAlunaficha Melody KiraniaNo ratings yet
- Hospital Acquired InfectionsDocument55 pagesHospital Acquired Infectionshaningtonjunior19No ratings yet
- Principle of Prevention To Infectious DiseaseDocument37 pagesPrinciple of Prevention To Infectious DiseaseSheryl ElitaNo ratings yet
- Isolation PrecautionsDocument58 pagesIsolation PrecautionsDrShereen Fawzy HafezNo ratings yet
- Nosocomial Infections: Dr. Nessren Farouk Lecturer of Public Health and Community MedicineDocument37 pagesNosocomial Infections: Dr. Nessren Farouk Lecturer of Public Health and Community MedicineAhmed MakledNo ratings yet
- 2022 Intensive Course. MM - Viral Hepatitis & HIV - AP Datin DR Noor ZettiDocument65 pages2022 Intensive Course. MM - Viral Hepatitis & HIV - AP Datin DR Noor ZettiRaja RuzannaNo ratings yet
- Infectious Disorders of Adults Transes Quiano Lp2 DiscussionDocument13 pagesInfectious Disorders of Adults Transes Quiano Lp2 DiscussionLorelyn FabrigarasNo ratings yet
- Infection Control: IntroductionDocument17 pagesInfection Control: Introductionsuman gupta100% (1)
- Funda Lab Mod 1-4Document23 pagesFunda Lab Mod 1-4Liane BartolomeNo ratings yet
- Rubella: Prepared and Presented by Ibrahim Ali Assiri 439106123Document21 pagesRubella: Prepared and Presented by Ibrahim Ali Assiri 439106123عادل حكميNo ratings yet
- Infection Control ModuleDocument12 pagesInfection Control ModuleFreida Michelle BonnitNo ratings yet
- Unknown 3Document14 pagesUnknown 3fares222.alohleNo ratings yet
- Preventing InfectionDocument56 pagesPreventing InfectionSol Angelika G. SuropiaNo ratings yet
- Communicable-D FINAL 2021-1-9Document16 pagesCommunicable-D FINAL 2021-1-9Shimaa KashefNo ratings yet
- Infection Control PracticesDocument5 pagesInfection Control PracticesMaryNo ratings yet
- Corynebacterium DiphtheriaeDocument27 pagesCorynebacterium DiphtheriaeBarkavi 9620No ratings yet
- Communicable Disease NursingDocument45 pagesCommunicable Disease NursingCahsrDlshsiNo ratings yet
- Communicable DisesaseDocument111 pagesCommunicable Disesasebrillaboy266No ratings yet
- Nosocomial InfectionsDocument26 pagesNosocomial InfectionsJuned SiddiqueNo ratings yet
- Seminar ON: Infection Prevention (Including Hiv) and Standard Safety Measures, Bio - Medical Waste ManagementDocument24 pagesSeminar ON: Infection Prevention (Including Hiv) and Standard Safety Measures, Bio - Medical Waste ManagementTHONDYNALUNo ratings yet
- CD Part 2 - Communicable Diseases With Pics (1) ConDocument239 pagesCD Part 2 - Communicable Diseases With Pics (1) ConMackoi SalamanesNo ratings yet
- Chapter 2 Infection Control LecDocument45 pagesChapter 2 Infection Control LecRhea CarinoNo ratings yet
- Nosocomial InfectionDocument30 pagesNosocomial InfectionZephas HillsNo ratings yet
- CDC Guidelines For Isolation Precautions in HospitalsDocument5 pagesCDC Guidelines For Isolation Precautions in Hospitalseng78ineNo ratings yet
- Communicable Disease: Mr. Pankaj Kusum Ramdas KhuspeDocument113 pagesCommunicable Disease: Mr. Pankaj Kusum Ramdas KhuspeManisa ParidaNo ratings yet
- Assign. Communicable DiseaseDocument25 pagesAssign. Communicable Diseasepooja banyalNo ratings yet
- Definition of InfectionDocument27 pagesDefinition of InfectionRenit AntoNo ratings yet
- 7epidemiology and Public HealthDocument47 pages7epidemiology and Public HealthJxce MLeKidNo ratings yet
- Is Monkeypox The Next Pandemic ?Document21 pagesIs Monkeypox The Next Pandemic ?Cyril LambayongNo ratings yet
- Chapter 14: Host Parasite RelationshipsDocument10 pagesChapter 14: Host Parasite RelationshipsNurul WidyawatiNo ratings yet
- Professor Panna Lal Saha BGC Trust Medical College ChittagongDocument39 pagesProfessor Panna Lal Saha BGC Trust Medical College ChittagongPanna SahaNo ratings yet
- Nosocomial Infections - Dr. LindaDocument30 pagesNosocomial Infections - Dr. LindaGeorge C. KasondaNo ratings yet
- Monkey PoxDocument29 pagesMonkey PoxMalavika A GNo ratings yet
- 1 Lect Surgery Infection Controle-Adobe PDFDocument56 pages1 Lect Surgery Infection Controle-Adobe PDFNadeem AlawashrehNo ratings yet
- Hospital Acquired Infections PDFDocument4 pagesHospital Acquired Infections PDFMuhammad Mohsin Ali DynamoNo ratings yet
- Prevention and Control of InfectionDocument138 pagesPrevention and Control of InfectionJeon CookyNo ratings yet
- Mechanism of Infection and Transmission of Disease: PresentationDocument29 pagesMechanism of Infection and Transmission of Disease: PresentationSuryakant SonwaniNo ratings yet
- Output 1 InfectionDocument13 pagesOutput 1 InfectionallanrnmanalotoNo ratings yet
- Airborne Transmission: Nurul Aqmar Mohd Nor Hazalin Phc454 - Pharmaceutical MicrobiologyDocument27 pagesAirborne Transmission: Nurul Aqmar Mohd Nor Hazalin Phc454 - Pharmaceutical MicrobiologySuhaila Abdul RahimNo ratings yet
- Module 11Document35 pagesModule 11camille nina jane navarroNo ratings yet
- Six Elements of InfectionDocument18 pagesSix Elements of InfectionAlhadzra AlihNo ratings yet
- Week 4. Infection Control Fall 22-23Document40 pagesWeek 4. Infection Control Fall 22-23aisha.hadid31No ratings yet
- 5.infection Control & Standard PrecautionsDocument33 pages5.infection Control & Standard PrecautionsGilbert JohnNo ratings yet
- Infection Precaution, HTMDocument32 pagesInfection Precaution, HTMAuzaniAkraminAhmadNo ratings yet
- Microbial Associations/Interactio NS: Nanette Ramilo-Cruz, MD, DPAFPDocument50 pagesMicrobial Associations/Interactio NS: Nanette Ramilo-Cruz, MD, DPAFPKhatrinaNo ratings yet
- MicroorganismsDocument14 pagesMicroorganismsDima MasadehNo ratings yet
- Communicable DiseasesDocument43 pagesCommunicable Diseasesipshitadas.21No ratings yet
- Contagious Diseases: The Science, History, and Future of Epidemics. From Ancient Plagues to Modern Pandemics, How to Stay Ahead of a Global Health CrisisFrom EverandContagious Diseases: The Science, History, and Future of Epidemics. From Ancient Plagues to Modern Pandemics, How to Stay Ahead of a Global Health CrisisNo ratings yet
- Drug Study: Lidocaine Hydrochloride XylocaineDocument2 pagesDrug Study: Lidocaine Hydrochloride XylocaineJoevence Gazo CuaresmaNo ratings yet
- Drug Study: 10cc/1vialDocument2 pagesDrug Study: 10cc/1vialJoevence Gazo CuaresmaNo ratings yet
- H-Mole NCPsDocument7 pagesH-Mole NCPsJoevence Gazo CuaresmaNo ratings yet
- Activity Intolerance Related To Generalized Weakness As EvidencedDocument2 pagesActivity Intolerance Related To Generalized Weakness As EvidencedJoevence Gazo CuaresmaNo ratings yet
- College of Arts and Sciences Nursing Department: InstructionDocument3 pagesCollege of Arts and Sciences Nursing Department: InstructionJoevence Gazo CuaresmaNo ratings yet
- JMJ Marist Brothers Notre Dame of Marbel University College of Arts and Sciences - Nursing Department Alunan Avenue, Koronadal City, South CotabatoDocument1 pageJMJ Marist Brothers Notre Dame of Marbel University College of Arts and Sciences - Nursing Department Alunan Avenue, Koronadal City, South CotabatoJoevence Gazo CuaresmaNo ratings yet
- DIPHENHYDRAMINEDocument4 pagesDIPHENHYDRAMINEJoevence Gazo CuaresmaNo ratings yet
- Drug-Study - ParacetamolDocument1 pageDrug-Study - ParacetamolJoevence Gazo CuaresmaNo ratings yet
- Drug-Study - DiphenhydramineDocument2 pagesDrug-Study - DiphenhydramineJoevence Gazo CuaresmaNo ratings yet
- DRUG+STUDY NaprexDocument2 pagesDRUG+STUDY NaprexJoevence Gazo CuaresmaNo ratings yet
- DRUG+STUDY PropofolDocument2 pagesDRUG+STUDY PropofolJoevence Gazo Cuaresma100% (2)
- Physiology, Body Fluids - StatPearls - NCBI BookshelfDocument5 pagesPhysiology, Body Fluids - StatPearls - NCBI Bookshelfpilar gabriela hernandez fernandezNo ratings yet
- Vitiligo - Pathogenesis, Clinical Features, and Diagnosis - UpToDateDocument38 pagesVitiligo - Pathogenesis, Clinical Features, and Diagnosis - UpToDateInna MeratiNo ratings yet
- Case Study Renal DiseaseDocument33 pagesCase Study Renal DiseaseJewel BrondaNo ratings yet
- Vitamin D: Gandham. RajeevDocument66 pagesVitamin D: Gandham. Rajeevguna sundariNo ratings yet
- Wifi Study April PDFDocument153 pagesWifi Study April PDFসূর্যোদয় এক নতুন প্রচেষ্টাNo ratings yet
- Studies in Diabetes by Irina Obrosova, Martin J. Stevens, Mark A. Yorek (Eds.)Document277 pagesStudies in Diabetes by Irina Obrosova, Martin J. Stevens, Mark A. Yorek (Eds.)tasnimkheir1No ratings yet
- MSC Yoga - Semester 2 Hatha Yoga Pradipika - Answers To 10 Marks QuestionsDocument32 pagesMSC Yoga - Semester 2 Hatha Yoga Pradipika - Answers To 10 Marks QuestionsHenrickNo ratings yet
- Approach To The Patient With Postmenopausal Uterine Bleeding - UpToDateDocument18 pagesApproach To The Patient With Postmenopausal Uterine Bleeding - UpToDateCHINDY REPA REPANo ratings yet
- TB 200430183237Document68 pagesTB 200430183237Rahmadika NofriNo ratings yet
- Clinical Practice GuidelinesDocument99 pagesClinical Practice GuidelinesKersti Marzo100% (1)
- Previous BON Files (Medical-Surgical Nursing)Document14 pagesPrevious BON Files (Medical-Surgical Nursing)Tom CuencaNo ratings yet
- Warm Water Compress As An Alternative For Decreasing The Degree of Superficial Phlebitis in Children During HospitalizationDocument8 pagesWarm Water Compress As An Alternative For Decreasing The Degree of Superficial Phlebitis in Children During HospitalizationYogi SastrawanNo ratings yet
- Role of 50 Millesimal Potencies in Primary Dysmenorrhoea Updated PDFDocument106 pagesRole of 50 Millesimal Potencies in Primary Dysmenorrhoea Updated PDFKamal Patidar50% (2)
- Euthanasia Reading Comprehension2Document2 pagesEuthanasia Reading Comprehension2Angel O Cordoba RromNo ratings yet
- Automation of Ventilator Control For Hyperbaric Oxygen TherapyDocument2 pagesAutomation of Ventilator Control For Hyperbaric Oxygen Therapyra5tr@No ratings yet
- Chen, S., Et - Al. (2020) - (01-11)Document11 pagesChen, S., Et - Al. (2020) - (01-11)Vielia IrmayantiNo ratings yet
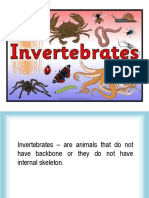
- InvertebratesDocument46 pagesInvertebratesIvy Mae ArnaizNo ratings yet
- 4.6.3.cavitary Syndrome (19525)Document3 pages4.6.3.cavitary Syndrome (19525)Ioana DucaNo ratings yet
- Dr. Teguh - Peran TCM Dalam DX TB Dan TBRO - TB Day 2019Document23 pagesDr. Teguh - Peran TCM Dalam DX TB Dan TBRO - TB Day 2019Meillyssa ChandraNo ratings yet
- SP234 Bird GuanoDocument3 pagesSP234 Bird GuanoJohn GeddesNo ratings yet
- WES WGS Brochure Pages V2.1eng Web 20201019Document16 pagesWES WGS Brochure Pages V2.1eng Web 20201019drumerNo ratings yet
- Mount Sinai ICUDocument642 pagesMount Sinai ICUMahmoud FathyNo ratings yet
- Steps in Viral Pathogenesis-Lecture ThreeDocument3 pagesSteps in Viral Pathogenesis-Lecture ThreeIM CTNo ratings yet
- Birth TraumaDocument57 pagesBirth TraumaAbu HajerahNo ratings yet
- 5 - Ruth (17 Aug 2020) Hawazen - CheckedDocument2 pages5 - Ruth (17 Aug 2020) Hawazen - CheckedDr. Emad Elbadawy د عماد البدويNo ratings yet
- FibrobookletDocument24 pagesFibrobookletNeptune ShellNo ratings yet
- Evaluation of The Child With Global Developmental DelayDocument14 pagesEvaluation of The Child With Global Developmental DelaylauramwoodyardNo ratings yet