You might also like
- Clinical Cases For OSCE's (Pharmacy)Document13 pagesClinical Cases For OSCE's (Pharmacy)Anam MirNo ratings yet
- Expanded Maternity Leave Checklist For Full PayDocument2 pagesExpanded Maternity Leave Checklist For Full PayEmil CastilloNo ratings yet
- Infant Care and Feeding Notes 1Document46 pagesInfant Care and Feeding Notes 1Art John CalambaNo ratings yet
- Newborn CareDocument120 pagesNewborn Carejuly3ciaNo ratings yet
- Oxygen AdministrationDocument4 pagesOxygen Administrationss100% (1)
- High - Risk PregnancyDocument110 pagesHigh - Risk PregnancyAndre DityaNo ratings yet
- Handouts Developmental MilestoneDocument8 pagesHandouts Developmental MilestoneJonas Marvin AnaqueNo ratings yet
- Pediatric Checklist EditedDocument72 pagesPediatric Checklist EditedJun Man100% (2)
- BGH ChartingDocument3 pagesBGH ChartingDjan Kurvie ValencerinaNo ratings yet
- Essential Intrapartum and Newborn CareDocument37 pagesEssential Intrapartum and Newborn CareVenice s SantosNo ratings yet
- Unang YakapDocument57 pagesUnang YakapHelen Grace Avila100% (3)
- Unang YakapDocument27 pagesUnang YakapMary Faith Kiat-ongNo ratings yet
- Einc Eval ExamDocument8 pagesEinc Eval ExamMaxeneDhaleNo ratings yet
- Essential Intrapartum Newborn CareDocument36 pagesEssential Intrapartum Newborn Carefatima chrystelle nuñal100% (1)
- BSN Level III Clinical InstructorDocument33 pagesBSN Level III Clinical InstructorChristine Bell JapitanaNo ratings yet
- Breastfeeding PDFDocument11 pagesBreastfeeding PDFSatya Prakash TiwariNo ratings yet
- Essential Intrapartum Newborn Care 181120082158 PDFDocument19 pagesEssential Intrapartum Newborn Care 181120082158 PDFDorinna Rizada BagaNo ratings yet
- Calamba Doctors' Colleges: Performance Evaluation ChecklistDocument2 pagesCalamba Doctors' Colleges: Performance Evaluation ChecklistJapsay Francisco GranadaNo ratings yet
- University of Saint Louis Tuguegarao City, Philippines: Maternal and Child Health NursingDocument70 pagesUniversity of Saint Louis Tuguegarao City, Philippines: Maternal and Child Health NursingSam PothNo ratings yet
- EP7 - ET Suctioning SlideshowDocument19 pagesEP7 - ET Suctioning SlideshowYashodhara Ghosh SenNo ratings yet
- EINC Essential Intrapartim NC ChecklistDocument7 pagesEINC Essential Intrapartim NC Checklisthey aadarshaNo ratings yet
- Essential Intrapartum and Newborn Care Practice Session ChecklistDocument28 pagesEssential Intrapartum and Newborn Care Practice Session ChecklistMonica Melchor DoriaNo ratings yet
- CounsellingDocument2 pagesCounsellingMarlie Villanueva100% (1)
- NCM 107 (Unang Yakap)Document28 pagesNCM 107 (Unang Yakap)Danna MendozaNo ratings yet
- Essential Intrapartum and Newborn CareDocument27 pagesEssential Intrapartum and Newborn Careteabagman100% (2)
- New Born Care: Slide 0: Learning ObjectivesDocument10 pagesNew Born Care: Slide 0: Learning ObjectivesAmelia ChristmasNo ratings yet
- Breastfeeding 120912050521 Phpapp01Document57 pagesBreastfeeding 120912050521 Phpapp01varshasharma05No ratings yet
- 3 - Intrapartum CareDocument97 pages3 - Intrapartum CareRem AlfelorNo ratings yet
- Perineal Care ChecklistDocument4 pagesPerineal Care Checklistgalaxy113100% (3)
- Essential Intrapartum and Newborn CareDocument23 pagesEssential Intrapartum and Newborn CareEarl ReyesNo ratings yet
- Pointers To Review NMC CBTDocument2 pagesPointers To Review NMC CBTLouie Rudolf Kim67% (9)
- Essential Intrapartum and Newborn CareDocument27 pagesEssential Intrapartum and Newborn CareKaren Mae AlcantaraNo ratings yet
- Brighten, Jolene - Healing Your Body Naturally After Childbirth - The New Mom's Guide To Navigating The Fourth Trimester (2015, Brighten Wellness)Document186 pagesBrighten, Jolene - Healing Your Body Naturally After Childbirth - The New Mom's Guide To Navigating The Fourth Trimester (2015, Brighten Wellness)Ivana100% (1)
- Imci ChartDocument26 pagesImci ChartDenise Espinosa100% (1)
- AO - MBFHI. 2pptDocument44 pagesAO - MBFHI. 2pptcorzpun168678100% (3)
- Ncm-120-Week-14-Topic 8 (F-P) - Nov 8 To 13, 2021Document45 pagesNcm-120-Week-14-Topic 8 (F-P) - Nov 8 To 13, 2021Shaf Abubakar100% (1)
- EENC (Early Essential Newborn Care)Document74 pagesEENC (Early Essential Newborn Care)Jennifer AlamonNo ratings yet
- FHSISDocument31 pagesFHSISNezer SorianoNo ratings yet
- EINCDocument2 pagesEINCmayeNo ratings yet
- Procedure Checklist For Einc (NCM 07-SL) DoneDocument3 pagesProcedure Checklist For Einc (NCM 07-SL) DoneKath AngelesNo ratings yet
- Einc ReviewerDocument4 pagesEinc ReviewerEricson Candelaria0% (1)
- Bag TechniqueDocument30 pagesBag Techniquecoosa liquors100% (1)
- RD ManualDocument6 pagesRD Manualapple m.No ratings yet
- Essential Newborn CareDocument20 pagesEssential Newborn Carejanjan_cepilloNo ratings yet
- Essential Newborn Care ProtocolDocument23 pagesEssential Newborn Care ProtocolKaren Viviene CincoNo ratings yet
- Essential Intrapartum Newborn Care 1 AutosavedDocument30 pagesEssential Intrapartum Newborn Care 1 AutosavedJamie HaravataNo ratings yet
- Steps in Essential Newborn CareDocument12 pagesSteps in Essential Newborn CareCedy L. CieloNo ratings yet
- PP Bag TechniqueDocument74 pagesPP Bag TechniqueAngelika BacoNo ratings yet
- Breast Care and Assisting in BreastfeedingDocument7 pagesBreast Care and Assisting in BreastfeedingBJ FernandezNo ratings yet
- Quiz 2Document15 pagesQuiz 2Francis Rafael PadillaNo ratings yet
- Grace NBCareDocument47 pagesGrace NBCareGrace Ordinario Sabordo100% (1)
- (R1) National Health Situation On MCNDocument4 pages(R1) National Health Situation On MCNNicole HonradoNo ratings yet
- A. KMC Introduction, Components & BenefitsDocument25 pagesA. KMC Introduction, Components & BenefitssantojuliansyahNo ratings yet
- Home Visit Steps: Perform The Bag TechniqueDocument4 pagesHome Visit Steps: Perform The Bag TechniqueRasec Nayr CoseNo ratings yet
- Unit VIII PRESUMPTIVE SIGNS AND SYMPTOMS OF PREGNANCYDocument5 pagesUnit VIII PRESUMPTIVE SIGNS AND SYMPTOMS OF PREGNANCYNancy100% (1)
- Non Time-Bound Procedures: ProcedureDocument5 pagesNon Time-Bound Procedures: ProcedureArlyn MarcelinoNo ratings yet
- Done LEOPOLDS MANEUVER MONICITDocument2 pagesDone LEOPOLDS MANEUVER MONICITMoiraMaeBeridoBaliteNo ratings yet
- Bag Technique Lecture NotesDocument4 pagesBag Technique Lecture NotesSarahLabadanNo ratings yet
- Technique For Bag TechniqueDocument2 pagesTechnique For Bag TechniqueVince Leonida100% (1)
- Catheterization: NCM 107 LabDocument4 pagesCatheterization: NCM 107 LabCatherine PradoNo ratings yet
- High Risk NewbornDocument4 pagesHigh Risk NewbornHanna AligatoNo ratings yet
- v3.PhilHealth Presentation For DepEd PRO III - 072619Document127 pagesv3.PhilHealth Presentation For DepEd PRO III - 072619Hazelle BondocNo ratings yet
- 4 Core Steps of EincDocument52 pages4 Core Steps of Eincjamaica cabriga100% (1)
- Essential Intrapartal and Newborn CareDocument4 pagesEssential Intrapartal and Newborn CareJoycee BoNo ratings yet
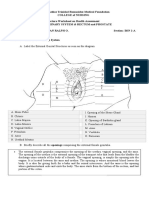
- Genitourinary Lecture BorromeoDocument8 pagesGenitourinary Lecture BorromeoKriztian BorromeoNo ratings yet
- Neurologic Lecture BorromeoDocument6 pagesNeurologic Lecture BorromeoKriztian BorromeoNo ratings yet
- Teaching Strategies Worksheet: Cognitive Learning Theories: The FollowingDocument7 pagesTeaching Strategies Worksheet: Cognitive Learning Theories: The FollowingKriztian BorromeoNo ratings yet
- Name: Kriztian Ralph O. Borromeo Year Level: BSN 2-A Nutri Group: CDocument8 pagesName: Kriztian Ralph O. Borromeo Year Level: BSN 2-A Nutri Group: CKriztian BorromeoNo ratings yet
- BORROMEO, K - Week13ReflectionJournal104Document1 pageBORROMEO, K - Week13ReflectionJournal104Kriztian BorromeoNo ratings yet
- Teaching Strategies TOPIC: Understanding Motivation and Behavior ChangeDocument3 pagesTeaching Strategies TOPIC: Understanding Motivation and Behavior ChangeKriztian BorromeoNo ratings yet
- Fundamentals of Nursing Worksheet in Nutrition and EliminationDocument3 pagesFundamentals of Nursing Worksheet in Nutrition and EliminationKriztian BorromeoNo ratings yet
- Chapter Two 2.0 Literature ReviewDocument2 pagesChapter Two 2.0 Literature Reviewjohn mwangiNo ratings yet
- K - (0gq I5) U U!$g.qDocument64 pagesK - (0gq I5) U U!$g.qKristel AnneNo ratings yet
- Discuss The Principles and Complications of The Various Sling Surgeries For Nulliparous Prolapse?Document14 pagesDiscuss The Principles and Complications of The Various Sling Surgeries For Nulliparous Prolapse?ashwiniNo ratings yet
- Vaginal InfectionDocument14 pagesVaginal InfectionmariaNo ratings yet
- Ansci ReviewerDocument5 pagesAnsci ReviewerMyles QuinteroNo ratings yet
- Anemia in Pregnancy: Maternal and Child Health NursingDocument20 pagesAnemia in Pregnancy: Maternal and Child Health NursingSunny Mae Tura PuigNo ratings yet
- Bellini 2015Document7 pagesBellini 2015Tifanny TantosoNo ratings yet
- IYCF - Infant and Young Child Feeding National Counselling Cards For Community Workers UgandaDocument27 pagesIYCF - Infant and Young Child Feeding National Counselling Cards For Community Workers UgandaJewelle Anne Estanilla LimenNo ratings yet
- Immediate Newborn Care: Care of The Newborn at The Time of BirthDocument42 pagesImmediate Newborn Care: Care of The Newborn at The Time of BirthDara Gi's FashionHausNo ratings yet
- (A) Multiple Choice Questions, Answers and Explanation 1Document3 pages(A) Multiple Choice Questions, Answers and Explanation 1Angela MariaNo ratings yet
- The Determinance of Induced Abortion Among Undergraduate StudentsDocument87 pagesThe Determinance of Induced Abortion Among Undergraduate StudentsUtibe Tibz IkpembeNo ratings yet
- Toxicologist Warns Against Covid Jabs PDFDocument14 pagesToxicologist Warns Against Covid Jabs PDFty techNo ratings yet
- Benign Pelvic and Perineal Masses - Prof HashimDocument32 pagesBenign Pelvic and Perineal Masses - Prof HashimVinesh SharmaNo ratings yet
- Mithun Rashi Baby Boy Names With MeaningsDocument7 pagesMithun Rashi Baby Boy Names With Meaningspoojamistry_123No ratings yet
- Welcome To The Morning SessionDocument23 pagesWelcome To The Morning SessionGENERAL sharpNo ratings yet
- Prenatal Development of The Eye and Its AdnexaDocument71 pagesPrenatal Development of The Eye and Its AdnexamumunooNo ratings yet
- Unit Three Nutritional RequirementDocument45 pagesUnit Three Nutritional RequirementHSC UNITEDNo ratings yet
- A Descriptive Study Was Undertaken To Gain Insight Into The Knowledge Base of Expectant Mother's Attending Antenatal OPD at A Selected Hospital in The State of Uttar PradeshDocument5 pagesA Descriptive Study Was Undertaken To Gain Insight Into The Knowledge Base of Expectant Mother's Attending Antenatal OPD at A Selected Hospital in The State of Uttar PradeshInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Endometrial BiopsyDocument13 pagesEndometrial BiopsyChanta MaharjanNo ratings yet
- Pratisandhi Report Bridging GapsDocument34 pagesPratisandhi Report Bridging GapsRadomir18No ratings yet
- ECO211 Powerpoint 10Document5 pagesECO211 Powerpoint 10Mostafa MahmoudNo ratings yet
- Musculoskeletal DevelopmentDocument40 pagesMusculoskeletal DevelopmentMajd HusseinNo ratings yet
- 3 PRIORITY NURSING CARE PLANS (Intrapartum and Postpartum Periods)Document11 pages3 PRIORITY NURSING CARE PLANS (Intrapartum and Postpartum Periods)Ryan Robert V. VentoleroNo ratings yet
- Nursing Care Plan 3 Risk For Altered ParentingDocument7 pagesNursing Care Plan 3 Risk For Altered Parentingdbryant010178% (9)
- The Effect of Endorphine Massage Againt Decrease in Pregnant Womens Back Pain in Varastri Salon Day Spa Sleman YogyakartaDocument3 pagesThe Effect of Endorphine Massage Againt Decrease in Pregnant Womens Back Pain in Varastri Salon Day Spa Sleman YogyakartaDerison MarsinovaNo ratings yet
- Deepika Final Report AnalysisDocument16 pagesDeepika Final Report AnalysisDeepika BhattaraiNo ratings yet