You might also like
- NHS UK Sub-Acromial DecompressionDocument3 pagesNHS UK Sub-Acromial DecompressionmertNo ratings yet
- Rotator Cuff RepairDocument5 pagesRotator Cuff RepairAdhitya TaslimNo ratings yet
- NHS UK Rotator Cuff RepairDocument5 pagesNHS UK Rotator Cuff RepairmertNo ratings yet
- NHS UK Total Shoulder Replacement, Hemiarthroplasty and Cap ReplacementDocument4 pagesNHS UK Total Shoulder Replacement, Hemiarthroplasty and Cap ReplacementmertNo ratings yet
- Flyer Ankle Sprain Rehabilitation PT GuidelineDocument3 pagesFlyer Ankle Sprain Rehabilitation PT GuidelineEka Wahyu HerdiyantiNo ratings yet
- NHS UK ACJ Reconstruction For InstabilityDocument4 pagesNHS UK ACJ Reconstruction For InstabilitymertNo ratings yet
- Sport Injury Rehablitation JPMRDocument22 pagesSport Injury Rehablitation JPMRlilis pratiwiNo ratings yet
- Achilles Mid Substance Speedbridge Rehab Guidelines CompressedDocument11 pagesAchilles Mid Substance Speedbridge Rehab Guidelines CompressedRAUL8609No ratings yet
- Rehabilitation Protocol of ACL ReconstructionDocument2 pagesRehabilitation Protocol of ACL ReconstructionkapsicumadNo ratings yet
- Rehab-Plans-and-Exercises Hip-Arthroscopy Protocol-For-Physiotherapy-Following-SurgeryDocument2 pagesRehab-Plans-and-Exercises Hip-Arthroscopy Protocol-For-Physiotherapy-Following-SurgeryMellow Moon RecordsNo ratings yet
- Non Operative Achilles Rupture GuidelinesDocument4 pagesNon Operative Achilles Rupture GuidelinesYosip Becerra MondragonNo ratings yet
- Post Op Cervical Fusion PDFDocument3 pagesPost Op Cervical Fusion PDFNICOLÁS ANDRÉS AYELEF PARRAGUEZNo ratings yet
- PT Guidelines Ankle Fracture With ORIF FinalDocument3 pagesPT Guidelines Ankle Fracture With ORIF FinalShinta ParamithaNo ratings yet
- Dr. Harold Shock III, MD Shoulder Stabilization: Goals For Phase 1 Range of MotionDocument4 pagesDr. Harold Shock III, MD Shoulder Stabilization: Goals For Phase 1 Range of MotionAbdul Wahid ShaikhNo ratings yet
- 4 Brunnstrom ApproachDocument18 pages4 Brunnstrom ApproachHabibieNaufal ChannelNo ratings yet
- Total Shoulder Arthroplasty Tsa 2Document15 pagesTotal Shoulder Arthroplasty Tsa 2api-550365743No ratings yet
- PT Nonop LCL PLCDocument4 pagesPT Nonop LCL PLCJo CacerNo ratings yet
- Physiotherapy Advice Post Gynae SurgeryDocument4 pagesPhysiotherapy Advice Post Gynae SurgerySamruddhi WadekarNo ratings yet
- Spondylolysis Non Operative Rehabilitation GuidelineDocument5 pagesSpondylolysis Non Operative Rehabilitation GuidelineAndroid HomeNo ratings yet
- Rehabilitation Guidelines For Post Operative Shoulder Instability Repair Updated20june08 - 0Document11 pagesRehabilitation Guidelines For Post Operative Shoulder Instability Repair Updated20june08 - 0Florin Vasile BosiNo ratings yet
- Case SummaryDocument4 pagesCase Summaryapi-479717740No ratings yet
- Spondylolysis Non Operative Rehabilitation GuidelineDocument5 pagesSpondylolysis Non Operative Rehabilitation GuidelineParnitha RajNo ratings yet
- RehabilitaciónpostCx Inestabilidad de HombroDocument13 pagesRehabilitaciónpostCx Inestabilidad de Hombromarcelogascon.oNo ratings yet
- Post Natal Exercise: King Edward Memorial HospitalDocument13 pagesPost Natal Exercise: King Edward Memorial HospitalElifah Rahmadhani100% (1)
- Rehabilitation Guidelines For Patients Undergoing Surgery For Lateral Ligament Reconstruction of The AnkleDocument10 pagesRehabilitation Guidelines For Patients Undergoing Surgery For Lateral Ligament Reconstruction of The AnkleVladGrosuNo ratings yet
- BalanceDocument31 pagesBalancebpt2No ratings yet
- Scapular-Stabilization Exercises - Early-Intervention PrescriptionDocument6 pagesScapular-Stabilization Exercises - Early-Intervention PrescriptionJohnnySnow100% (1)
- Post Op Lumbar FusionDocument3 pagesPost Op Lumbar FusionBaiq LenyNo ratings yet
- PT Guidelines For Ankle SprainDocument5 pagesPT Guidelines For Ankle SprainKirti GunjikarNo ratings yet
- NHS UK Distension, Manipulation Under Anaesthetic and Arthroscopic Capsular ReleaseDocument3 pagesNHS UK Distension, Manipulation Under Anaesthetic and Arthroscopic Capsular ReleasemertNo ratings yet
- Meniscal Repair GuidelineDocument2 pagesMeniscal Repair GuidelineTan Zhen XinNo ratings yet
- Flyer Sosm Knee Osteoarthritis Rehabilitation Guideline 11x8 - 5Document5 pagesFlyer Sosm Knee Osteoarthritis Rehabilitation Guideline 11x8 - 5Pedro GouveiaNo ratings yet
- Rotator Cuff Impingement PDFDocument8 pagesRotator Cuff Impingement PDFmadaleenNo ratings yet
- Lec9 Basic Concepts of Spinal Management With ExerciseDocument21 pagesLec9 Basic Concepts of Spinal Management With Exercisesana mumtazNo ratings yet
- (Guideline Post Operative Achilles Tendon Repair) PDFDocument3 pages(Guideline Post Operative Achilles Tendon Repair) PDFOkky SaidNo ratings yet
- ACL Rehabilitation ProgressionDocument8 pagesACL Rehabilitation ProgressionTomaž Radko Erjavec ŠnebergerNo ratings yet
- Lumbar Microdiscectomy Postoperative Physiotherapy and RehabilitationDocument4 pagesLumbar Microdiscectomy Postoperative Physiotherapy and RehabilitationfunkyhonkyNo ratings yet
- Post-Operative Physiotherapy Guidelines: Elbow ReplacementDocument1 pagePost-Operative Physiotherapy Guidelines: Elbow ReplacementBlake BoggenpoelNo ratings yet
- Rehabilitation Protocol After Anterior Cruciate Ligament ReconstructionDocument3 pagesRehabilitation Protocol After Anterior Cruciate Ligament ReconstructionTirumala RaoNo ratings yet
- PNF InserviceDocument25 pagesPNF Inserviceapi-518034073No ratings yet
- A Guide To Training With Knee Pain For Personal Trainers & Strength CoachesDocument1 pageA Guide To Training With Knee Pain For Personal Trainers & Strength CoachesMargarida MachadoNo ratings yet
- PT Acl Meniscus 2Document7 pagesPT Acl Meniscus 2sumitra87dasNo ratings yet
- Burn ManagementDocument15 pagesBurn ManagementPraneetha NouduriNo ratings yet
- Shoulder Post-Operative Rehabilitation ProtocolsDocument6 pagesShoulder Post-Operative Rehabilitation ProtocolsShrutiNo ratings yet
- Nursing Care Plan (NCP) : Date and Time Nursing Diagnosis Short - Term and Long - Term OutcomesDocument2 pagesNursing Care Plan (NCP) : Date and Time Nursing Diagnosis Short - Term and Long - Term OutcomesDeanne Carla DalilisNo ratings yet
- Ant Shoulder DislocationDocument3 pagesAnt Shoulder DislocationÉva KappéterNo ratings yet
- Rotator-Cuff-Repair Eggert 1015Document3 pagesRotator-Cuff-Repair Eggert 1015Sorin IordacheNo ratings yet
- General Guidelines /precautions:: Non-Operative Labral/FAI Hip Rehabilitation GuidelineDocument4 pagesGeneral Guidelines /precautions:: Non-Operative Labral/FAI Hip Rehabilitation GuidelineBurr NerrNo ratings yet
- Journals Ijatt 11 5 Article-P15-PreviewDocument2 pagesJournals Ijatt 11 5 Article-P15-Previewashlyn granthamNo ratings yet
- AerobicsDocument3 pagesAerobicsjohn kevin pascuaNo ratings yet
- Olympic Weightlifting Prep ProgramDocument124 pagesOlympic Weightlifting Prep ProgramSamehAlyNo ratings yet
- Acl Reconstruction ProtocolDocument8 pagesAcl Reconstruction ProtocolMestereaga AlinNo ratings yet
- Hip Labrum and Fai Non Operative Rehabilitation GuidelineDocument4 pagesHip Labrum and Fai Non Operative Rehabilitation GuidelineDevi MigiekaNo ratings yet
- Acl Reconstruction ProtocolDocument8 pagesAcl Reconstruction ProtocolFahd AbdelazimNo ratings yet
- Physical Therapy Prescription For Spasticity in Multiple SclerosisDocument4 pagesPhysical Therapy Prescription For Spasticity in Multiple SclerosisRiaz KhanNo ratings yet
- Complains of Sharp Pain Through Particular Ranges, Then The Therapist Needs To Modify The Exercises To Avoid A Painful ArcDocument6 pagesComplains of Sharp Pain Through Particular Ranges, Then The Therapist Needs To Modify The Exercises To Avoid A Painful Arcsimonpintaric3No ratings yet
- NCP For MGDocument2 pagesNCP For MGsalome carpioNo ratings yet
- Neurorestorasi Untuk Pasien Stroke Fase Post Akut (Pendekatan Konsep PNF)Document43 pagesNeurorestorasi Untuk Pasien Stroke Fase Post Akut (Pendekatan Konsep PNF)lizadwijanuaryanaNo ratings yet
- Balance and Fall Prevention: By, Sankari Nedunsaliyan Physiotherapist Dip in PT (MAL), BSC Hons Applied Rehab (UK)Document63 pagesBalance and Fall Prevention: By, Sankari Nedunsaliyan Physiotherapist Dip in PT (MAL), BSC Hons Applied Rehab (UK)Ali ImranNo ratings yet
- NHS UK ACJ Reconstruction For InstabilityDocument4 pagesNHS UK ACJ Reconstruction For InstabilitymertNo ratings yet
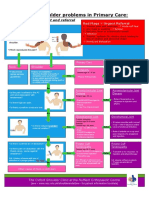
- NHS UK Diagnosis of Shoulder ProblemsDocument1 pageNHS UK Diagnosis of Shoulder ProblemsmertNo ratings yet
- Frozen Shoulder: Information For YouDocument8 pagesFrozen Shoulder: Information For YouCentaur Archer100% (1)
- NHS UK Posterior Stabilisation of The ShoulderDocument1 pageNHS UK Posterior Stabilisation of The ShouldermertNo ratings yet
- Oxford Elbow Score (OES) : English Version For The United KingdomDocument3 pagesOxford Elbow Score (OES) : English Version For The United KingdommertNo ratings yet
- Oxford Elbow Score (OES) : English Version For The United KingdomDocument3 pagesOxford Elbow Score (OES) : English Version For The United KingdommertNo ratings yet
- NHS UK Distension, Manipulation Under Anaesthetic and Arthroscopic Capsular ReleaseDocument3 pagesNHS UK Distension, Manipulation Under Anaesthetic and Arthroscopic Capsular ReleasemertNo ratings yet
- NHS UK Distension, Manipulation Under Anaesthetic and Arthroscopic Capsular ReleaseDocument3 pagesNHS UK Distension, Manipulation Under Anaesthetic and Arthroscopic Capsular ReleasemertNo ratings yet
- Journal Club PDADocument30 pagesJournal Club PDASnehal PatilNo ratings yet
- Your Guide To Post Surgery Care - Major - CleanDocument28 pagesYour Guide To Post Surgery Care - Major - CleanZar Chi LinNo ratings yet
- Ed Model of Care 2012Document68 pagesEd Model of Care 2012Hans GrobakNo ratings yet
- Ican BrochureDocument16 pagesIcan BrochureAbhishek ShatagopachariNo ratings yet
- HEALTH Career PlanDocument31 pagesHEALTH Career PlanHarlene Dela Cruz Ozar100% (2)
- Group 4 Case Presentation DiarrheaDocument46 pagesGroup 4 Case Presentation DiarrheaEphraim John QuichoNo ratings yet
- Newcastle Disease The Vaccines & Vaccination: by Haas Md. Yatim D.V.M (UPM)Document36 pagesNewcastle Disease The Vaccines & Vaccination: by Haas Md. Yatim D.V.M (UPM)zainodin adhomNo ratings yet
- Furuncles and Carbuncles: Bacterial Skin InfectionsDocument19 pagesFuruncles and Carbuncles: Bacterial Skin InfectionsKylie GolindangNo ratings yet
- Flunarizine Versus Betahistine in Vertigo: A Systematic ReviewDocument11 pagesFlunarizine Versus Betahistine in Vertigo: A Systematic ReviewevanoNo ratings yet
- TESTDocument22 pagesTESTjuniati samparaNo ratings yet
- Predicting Covid-19 Using External Symptoms With Fuzzy Logic.Document23 pagesPredicting Covid-19 Using External Symptoms With Fuzzy Logic.Samiksha BankarNo ratings yet
- Read The Passage and Answer The Questions: by An Old Age"Document1 pageRead The Passage and Answer The Questions: by An Old Age"Hesen Gozelov100% (1)
- Nat MurDocument19 pagesNat MurSun BNo ratings yet
- Tingkat Kepatuhan Antihipertensi Dan Pengontrolan Tekanan Darah Pasien Rawat Jalan Rs Pku Muhammadiyah BantulDocument6 pagesTingkat Kepatuhan Antihipertensi Dan Pengontrolan Tekanan Darah Pasien Rawat Jalan Rs Pku Muhammadiyah BantulRusnaneeNo ratings yet
- Digestion: The Good, The Bad, and The DirtyDocument43 pagesDigestion: The Good, The Bad, and The DirtyPatrícia Vieira100% (2)
- An Opd Based Prospective Exploratory Study of DermDocument4 pagesAn Opd Based Prospective Exploratory Study of DermSankita SandalNo ratings yet
- Prevention of Surgical Site Infections: Pola Brenner, Patricio NercellesDocument10 pagesPrevention of Surgical Site Infections: Pola Brenner, Patricio NercellesAmeng GosimNo ratings yet
- A Three-Dimensional Method of Visualizing The Temporomandibular Joint Based On Magnetic Resonance Imaging in A Case of Juvenile Chronic ArthritisDocument7 pagesA Three-Dimensional Method of Visualizing The Temporomandibular Joint Based On Magnetic Resonance Imaging in A Case of Juvenile Chronic ArthritisNAGARAJNo ratings yet
- REFLEXOLOGY PresentationDocument15 pagesREFLEXOLOGY Presentationdanielle palm100% (4)
- Assessment Tool For Level 1 Hospital Annex K1 PDFDocument47 pagesAssessment Tool For Level 1 Hospital Annex K1 PDFMadelyn LamanilaoNo ratings yet
- The Relevance of Attachment Theory For PDocument52 pagesThe Relevance of Attachment Theory For PVeera Balaji KumarNo ratings yet
- Pancoast TumorDocument26 pagesPancoast TumorDhanis HastinNo ratings yet
- NCP CalculiDocument8 pagesNCP CalculihailleyannNo ratings yet
- Loresca - Ratio Mtle - HistopathDocument10 pagesLoresca - Ratio Mtle - HistopathKaycee Gretz LorescaNo ratings yet
- ABC of Intensive CareDocument49 pagesABC of Intensive CareCurro MirallesNo ratings yet
- Drug StudyDocument3 pagesDrug StudyJohn AlcantaraNo ratings yet
- Inside The Human BodyDocument1 pageInside The Human BodyKaravanNo ratings yet
- Management of Client With Integumentary DisordersDocument97 pagesManagement of Client With Integumentary Disordersduday76100% (1)
- Case Study 1Document4 pagesCase Study 1api-271668042No ratings yet
- The Kaohsiung J of Med Scie - 2013 - Tsai - Pyoderma Gangrenosum Intractable Leg Ulcers in Sjogren S SyndromeDocument2 pagesThe Kaohsiung J of Med Scie - 2013 - Tsai - Pyoderma Gangrenosum Intractable Leg Ulcers in Sjogren S SyndromeAsad KakarNo ratings yet