You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- CV Abdelgadir Ahmed Eltayeb.Document7 pagesCV Abdelgadir Ahmed Eltayeb.AbdelgadirEltayebNo ratings yet
- Endoscopic Sinus SurgeryDocument91 pagesEndoscopic Sinus SurgeryGiovanni HenryNo ratings yet
- Renewed CGHS UpdatesDocument60 pagesRenewed CGHS UpdatesJanipalli HarishNo ratings yet
- Brosur FESSDocument9 pagesBrosur FESSsoeyahyaNo ratings yet
- 07 RJR 08 Particularities of Anesthesia in ENT Endoscopic SurgeryDocument8 pages07 RJR 08 Particularities of Anesthesia in ENT Endoscopic SurgeryAyuAnatrieraNo ratings yet
- Stortz Endoscopic Sinus SurgeyDocument75 pagesStortz Endoscopic Sinus SurgeyAndreea Neacsu100% (1)
- University of Utah Health Nasal Polyps Content cv1 051820 MGDocument5 pagesUniversity of Utah Health Nasal Polyps Content cv1 051820 MGapi-297617076No ratings yet
- Endoscopic Sinus Surgery 1Document3 pagesEndoscopic Sinus Surgery 1Lamy houlou GeorgesNo ratings yet
- Diagnosis Dan Tatalaksana Rinosinusitis Maksilaris Odontogenik Yang Meluas Sampai Etmoid Dan Frontal: Laporan KasusDocument5 pagesDiagnosis Dan Tatalaksana Rinosinusitis Maksilaris Odontogenik Yang Meluas Sampai Etmoid Dan Frontal: Laporan Kasussupiana sastraNo ratings yet
- Changes in Mucociliary Clearance and Olfaction Following Endoscopic Sinus SurgeryDocument20 pagesChanges in Mucociliary Clearance and Olfaction Following Endoscopic Sinus SurgerygoolnuulNo ratings yet
- Endoscopic Sinus SurgeryDocument8 pagesEndoscopic Sinus SurgeryAdrIs Bravo MonteroNo ratings yet
- FessDocument3 pagesFessMadMariNo ratings yet
- Neck Pain Chronic Sinusitis and Eustachian Tube Dysfunction - Caring Medical FloridaDocument2 pagesNeck Pain Chronic Sinusitis and Eustachian Tube Dysfunction - Caring Medical FloridaTulisanNo ratings yet
- Are Errors in Otorhinolaryngology Always A Sign of Medical MalpracticeDocument7 pagesAre Errors in Otorhinolaryngology Always A Sign of Medical MalpracticeMyrellaAlexandraNo ratings yet
- CGHS Rates 2014 - Ahmedabad1Document51 pagesCGHS Rates 2014 - Ahmedabad1Chirag KoradiaNo ratings yet
- The Colleges of Medicine of South AfricaDocument7 pagesThe Colleges of Medicine of South AfricaJustine NyangaresiNo ratings yet
- 1 - Krespi - In-Office Laser Septal Spur RemovalDocument1 page1 - Krespi - In-Office Laser Septal Spur Removalmohamed radwanNo ratings yet
- CGHS Rates 2014 ChandigarhDocument45 pagesCGHS Rates 2014 Chandigarhsanjeeta.chauhan22No ratings yet
- CGHS Rates 2014 - HyderabadDocument60 pagesCGHS Rates 2014 - HyderabadPradeep PaswanNo ratings yet
- Thesis On Functional Endoscopic Sinus SurgeryDocument5 pagesThesis On Functional Endoscopic Sinus SurgeryBuyAPaperTulsa100% (2)
- Quality of Life After Functional Endoscopic Sinus Surgery in Patients With Chronic RhinosinusitisDocument15 pagesQuality of Life After Functional Endoscopic Sinus Surgery in Patients With Chronic RhinosinusitisNarendraNo ratings yet
- CGHS Rates - TrivandrumDocument79 pagesCGHS Rates - Trivandrumimran kureshiNo ratings yet
- 1 s2.0 S1879729618300073 MainDocument5 pages1 s2.0 S1879729618300073 MainAditiya RonaldiNo ratings yet
- International Journal of Surgery Case ReportsDocument5 pagesInternational Journal of Surgery Case ReportsLee제노No ratings yet
- NonCytotoxic Dibenzyl and Also Difluoroborate Capmatinibxlsxoid Fluorophores Permit Visual Image Involving Nucleus or Even Cytoplasm Inside Bioimagingixvwj PDFDocument1 pageNonCytotoxic Dibenzyl and Also Difluoroborate Capmatinibxlsxoid Fluorophores Permit Visual Image Involving Nucleus or Even Cytoplasm Inside Bioimagingixvwj PDFtubweed4No ratings yet
- CGHS Rates 2014 - BhopalDocument40 pagesCGHS Rates 2014 - BhopalUpendra SahuNo ratings yet
- Disorders of The Nose and Paranasal SinusesDocument50 pagesDisorders of The Nose and Paranasal Sinusesphew1234567890No ratings yet
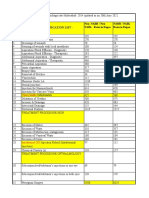
- CGHS Mumbai 2010 Rate List Updated On 29th June 2021Document45 pagesCGHS Mumbai 2010 Rate List Updated On 29th June 2021nishu solankiNo ratings yet
- Advice Following Nasal Surgery Fes Sep20Document8 pagesAdvice Following Nasal Surgery Fes Sep20Adela MarcovNo ratings yet
- CGHS RateListDocument45 pagesCGHS RateListSandip SharmaNo ratings yet