You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Monte Vista Journal Public Service EntryDocument25 pagesMonte Vista Journal Public Service EntryJennifer AlonzoNo ratings yet
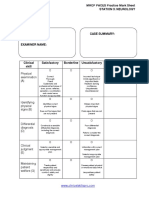
- Station 3 Neurology MRCP PACES Mark SheetDocument1 pageStation 3 Neurology MRCP PACES Mark SheetdoctorebrahimNo ratings yet
- Station 2 History MRCP PACES Practice Mark SheetDocument1 pageStation 2 History MRCP PACES Practice Mark SheetdoctorebrahimNo ratings yet
- Station 3 Cardiovascular MRCP PACES Practice Mark SheetDocument1 pageStation 3 Cardiovascular MRCP PACES Practice Mark SheetdoctorebrahimNo ratings yet
- Station 1 Abdominal MRCP PACES Practice Mark SheetDocument1 pageStation 1 Abdominal MRCP PACES Practice Mark SheetdoctorebrahimNo ratings yet
- Adam Vogel - Challenges and Possibilities of Automated Speech Monitoring in AtaxiaDocument15 pagesAdam Vogel - Challenges and Possibilities of Automated Speech Monitoring in AtaxiadoctorebrahimNo ratings yet
- In DiabetesDocument1 pageIn DiabetesdoctorebrahimNo ratings yet
- Carlo Wilke - NFL in SCA1 and MSA CDocument12 pagesCarlo Wilke - NFL in SCA1 and MSA CdoctorebrahimNo ratings yet
- Skin Involvement in Atypical Hemolytic Uremic SyndromeDocument4 pagesSkin Involvement in Atypical Hemolytic Uremic SyndromedoctorebrahimNo ratings yet
- CANOMODDocument9 pagesCANOMODdoctorebrahimNo ratings yet
- Impact of DM On MIDocument13 pagesImpact of DM On MIdoctorebrahimNo ratings yet
- CANOMAD Responding To Weekly IV ImmunoglobulinDocument4 pagesCANOMAD Responding To Weekly IV ImmunoglobulindoctorebrahimNo ratings yet
- Variants of Guillainbarre Syndrome Miller Fisher Syndrome Facial Diplegia and Multiple Cranial Nerve PalsiesDocument6 pagesVariants of Guillainbarre Syndrome Miller Fisher Syndrome Facial Diplegia and Multiple Cranial Nerve PalsiesdoctorebrahimNo ratings yet
- Stroke and Transient Ischaemic Attack in Over 16s Diagnosis and Initial Management PDF 66141665603269Document48 pagesStroke and Transient Ischaemic Attack in Over 16s Diagnosis and Initial Management PDF 66141665603269doctorebrahimNo ratings yet
- The Rare and The Unexpected Miller Fisher SyndromeDocument4 pagesThe Rare and The Unexpected Miller Fisher SyndromedoctorebrahimNo ratings yet
- Cadasil 072007Document39 pagesCadasil 072007doctorebrahimNo ratings yet
- Skin Care: Kind and Conscious Treatment For Your SkinDocument9 pagesSkin Care: Kind and Conscious Treatment For Your SkinCielo Amor RabangNo ratings yet
- Bahasa Inggris SPMB 2002 Regional IIIDocument3 pagesBahasa Inggris SPMB 2002 Regional IIIatikah_s0% (1)
- Admit Card RofDocument4 pagesAdmit Card RofSankit SasmalNo ratings yet
- Black Death ReportDocument2 pagesBlack Death ReportArthur YanNo ratings yet
- PollutionDocument13 pagesPollutionRahul VatsNo ratings yet
- Basic First Aid Training1Document30 pagesBasic First Aid Training1Richard LindsayNo ratings yet
- Appropriate AssessmentDocument35 pagesAppropriate AssessmentPeter EgbodorNo ratings yet
- Sally Magnusson - WHERE MEMORIES GO - 1st Chapter PDFDocument15 pagesSally Magnusson - WHERE MEMORIES GO - 1st Chapter PDFThe Sunday TimesNo ratings yet
- IRS 3500a Form For California Tax-ExemptionDocument1 pageIRS 3500a Form For California Tax-ExemptionjhbjhbkjhNo ratings yet
- Transference Focused PsychotherapyDocument22 pagesTransference Focused PsychotherapybobifilNo ratings yet
- Assesment Trauma PatientDocument10 pagesAssesment Trauma PatientCahyani KurniaNo ratings yet
- Lab Safety EssayDocument3 pagesLab Safety Essayapi-491255213No ratings yet
- Microbiology TestingDocument15 pagesMicrobiology TestingUmesh ChikhlikarNo ratings yet
- Requirements For Residential Concrete Construction and CommentaryDocument26 pagesRequirements For Residential Concrete Construction and CommentaryINARQ1979No ratings yet
- Case Studies For Dysfunctional FamilyDocument1 pageCase Studies For Dysfunctional FamilyTricia Hyazinth MendozaNo ratings yet
- MODULE 7 Labor Standards (ACD) Pacturan, CJADocument3 pagesMODULE 7 Labor Standards (ACD) Pacturan, CJACzarina JaneNo ratings yet
- Permit To Work Format - Ramzan Sugar Mills Limited (RSML)Document2 pagesPermit To Work Format - Ramzan Sugar Mills Limited (RSML)cuteboom1122No ratings yet
- Protogyl PDFDocument5 pagesProtogyl PDFpushkar078No ratings yet
- Creekside Naturals Children's Sleep AidDocument1 pageCreekside Naturals Children's Sleep Aidmirza abdullahNo ratings yet
- Lecture-Npos in The PhilippinesDocument14 pagesLecture-Npos in The PhilippinesAngela PaduaNo ratings yet
- Thesis TopicDocument10 pagesThesis TopicPrachi AgarwalNo ratings yet
- Dental Treatment of Medical Compromised PatientsDocument50 pagesDental Treatment of Medical Compromised PatientssrinivasNo ratings yet
- Avaaram PooDocument3 pagesAvaaram PooThirtha KumarNo ratings yet
- BrainwashedDocument2 pagesBrainwashedapi-304543250No ratings yet
- Identifying Information: Office of Medical Student AffairsDocument8 pagesIdentifying Information: Office of Medical Student AffairsAdnan Al JafaryNo ratings yet
- HopelessnessDocument20 pagesHopelessnessSyed BuRhan Ud-DinNo ratings yet
- NICE ProceedingsDocument63 pagesNICE Proceedingssn_b5No ratings yet
- Arellano University: Neatness: 2 Completeness: 3 Creativity: 2 Output: 8 Total: 15Document3 pagesArellano University: Neatness: 2 Completeness: 3 Creativity: 2 Output: 8 Total: 15Ashley Jade Hanna FloresNo ratings yet