You might also like
- Radiotherapy of Liver CancerFrom EverandRadiotherapy of Liver CancerJinsil SeongNo ratings yet
- Ahmed 2011Document10 pagesAhmed 2011skribekbenjaminNo ratings yet
- First-Line Crizotinib Versus Chemotherapy in ALK-Positive Lung CancerDocument11 pagesFirst-Line Crizotinib Versus Chemotherapy in ALK-Positive Lung CancerRitam JoarderNo ratings yet
- Mottet2016 PDFDocument12 pagesMottet2016 PDFdipawelloiNo ratings yet
- EJGO2022054 Cervical CaDocument8 pagesEJGO2022054 Cervical CaRahmayantiYuliaNo ratings yet
- 2019 Article 6402Document8 pages2019 Article 6402shahrasyiddNo ratings yet
- Ou 2016Document8 pagesOu 2016tami widiatul azahraNo ratings yet
- REQUITE A Prospective Multicentre Cohort Study ofDocument9 pagesREQUITE A Prospective Multicentre Cohort Study ofAhmad ShamyNo ratings yet
- Biomarkers For The Diagnosis of Cholangiocarcinoma A Systematic Review 2018Document10 pagesBiomarkers For The Diagnosis of Cholangiocarcinoma A Systematic Review 2018Anna MariaNo ratings yet
- J Juro 2018 07 040Document7 pagesJ Juro 2018 07 040wanggaNo ratings yet
- Consensus Recommendations For Radiation Therapy Contouring and Treatment of Vulvar Carcinoma Gaffney 2016Document17 pagesConsensus Recommendations For Radiation Therapy Contouring and Treatment of Vulvar Carcinoma Gaffney 2016zanNo ratings yet
- Male Breast Cancer: An Institutional ExperienceDocument5 pagesMale Breast Cancer: An Institutional ExperienceIJAR JOURNALNo ratings yet
- Factors Affecting The Approaches and Complications of Surgery inDocument8 pagesFactors Affecting The Approaches and Complications of Surgery inAlin VázquezNo ratings yet
- Baumann 2016 IJROBP Development Validation of Bladder Contouring AtlasDocument9 pagesBaumann 2016 IJROBP Development Validation of Bladder Contouring AtlaszanNo ratings yet
- Cancer de PancreasDocument12 pagesCancer de PancreasRuben RoaNo ratings yet
- Fonc 13 1162683Document2 pagesFonc 13 1162683vinadata01No ratings yet
- Tugas Ibu RetinoblastomaDocument7 pagesTugas Ibu RetinoblastomamalaNo ratings yet
- Expert Consensus Contouring Guidelines For Intensity Modulated Radiation Therapy in Esophageal and Gastroesophageal Junction CancerDocument10 pagesExpert Consensus Contouring Guidelines For Intensity Modulated Radiation Therapy in Esophageal and Gastroesophageal Junction CancermarrajoanaNo ratings yet
- The Addition of Pelvic Lymph Node Treatment To Pro - 9Document2 pagesThe Addition of Pelvic Lymph Node Treatment To Pro - 9gascarteziniNo ratings yet
- PublicacionDocument5 pagesPublicacionNoelia Peirats AymerichNo ratings yet
- SouthAsianJCancer6115-2517942 065939Document5 pagesSouthAsianJCancer6115-2517942 065939Gibi SupitNo ratings yet
- Prognostic Model For Survival of Local Recurrent Nasopharyngeal Carcinoma With Intensity-Modulated RadiotherapyDocument7 pagesPrognostic Model For Survival of Local Recurrent Nasopharyngeal Carcinoma With Intensity-Modulated Radiotherapypp kabsemarangNo ratings yet
- Paper 2Document13 pagesPaper 2บอส เลิศเกียรติรัชตะNo ratings yet
- 10 1016@j Jfma 2018 01 015Document10 pages10 1016@j Jfma 2018 01 015darpa22No ratings yet
- Fonc 07 00177Document13 pagesFonc 07 00177Ihenanacho HappinessNo ratings yet
- Concurrent Cisplatin, Etoposide, and Chest Radiotherapy in Pathologic Stage IIIB Non-Small-Cell Lung CancerDocument7 pagesConcurrent Cisplatin, Etoposide, and Chest Radiotherapy in Pathologic Stage IIIB Non-Small-Cell Lung Cancerdurgesh kumarNo ratings yet
- Radioterapia en CacUDocument6 pagesRadioterapia en CacUVicente RamosNo ratings yet
- Efficacy of Intensity-Modulated Radiotherapy With Concurrent Carboplatin in Nasopharyngeal CarcinomaDocument8 pagesEfficacy of Intensity-Modulated Radiotherapy With Concurrent Carboplatin in Nasopharyngeal CarcinomadenanurbaniazharNo ratings yet
- 2019 Article 5894 PDFDocument8 pages2019 Article 5894 PDFGalgalo GarbichaNo ratings yet
- Apalutamide For Metastatic, Castration-Sensitive Prostate Cancer TITANDocument12 pagesApalutamide For Metastatic, Castration-Sensitive Prostate Cancer TITANOrlando SotoNo ratings yet
- P1 Functional Outcomes and Health-Related QualityDocument11 pagesP1 Functional Outcomes and Health-Related Qualityernitaranterupang79No ratings yet
- Prophylactic Irradiation To The Contralateral BreaDocument6 pagesProphylactic Irradiation To The Contralateral Breaashnamuni07No ratings yet
- Xu 2021Document9 pagesXu 2021Drsaumyta MishraNo ratings yet
- Clinical StudyDocument7 pagesClinical StudyTit fuckerNo ratings yet
- Uganda - CervixDocument9 pagesUganda - CervixDaniel PalmeraNo ratings yet
- P. Wang Et Al.2019Document6 pagesP. Wang Et Al.2019Mai M. AlshalNo ratings yet
- Efficacy and Safety of Endoscopic Nasopharyngectomy Combined With Low-Dose Radiotherapy For Primary T1-2 Nasopharyngeal CarcinomaDocument7 pagesEfficacy and Safety of Endoscopic Nasopharyngectomy Combined With Low-Dose Radiotherapy For Primary T1-2 Nasopharyngeal CarcinomaRoger J MorenoNo ratings yet
- Me Hanna 2016Document11 pagesMe Hanna 2016eswarNo ratings yet
- Escamoso de Esofago Cervical Metaanalisis, Guler 2022Document2 pagesEscamoso de Esofago Cervical Metaanalisis, Guler 2022Carlos N. Rojas PuyolNo ratings yet
- Gynecologic Oncology Reports: Olpin J., Chuang L., Berek J., Ga Ffney D. TDocument7 pagesGynecologic Oncology Reports: Olpin J., Chuang L., Berek J., Ga Ffney D. TJheyson Javier Barrios PereiraNo ratings yet
- MainDocument7 pagesMainHanaNo ratings yet
- International Seminars in Surgical OncologyDocument8 pagesInternational Seminars in Surgical OncologyAhmad ShafiqNo ratings yet
- ACPGBI CRC Part 1Document3 pagesACPGBI CRC Part 1NevilleNo ratings yet
- ESMO Guideline 2019 - Early Breast Cancer TreatmentDocument27 pagesESMO Guideline 2019 - Early Breast Cancer Treatmentrahma watiNo ratings yet
- 10.1016@S1470 20451930318 3Document10 pages10.1016@S1470 20451930318 3FistiNo ratings yet
- Surgical Treatment of Trichilemmal CarcinomaDocument4 pagesSurgical Treatment of Trichilemmal CarcinomaNESRINE MARZAKNo ratings yet
- Neadyuvancia Cancer de Pene 1Document5 pagesNeadyuvancia Cancer de Pene 1Ivan Perez NestaresNo ratings yet
- MainDocument8 pagesMainIoana CucuNo ratings yet
- J Eururo 2020 09 046Document20 pagesJ Eururo 2020 09 046Ivor Wiguna Hartanto WilopoNo ratings yet
- TIRADS2017Document9 pagesTIRADS2017Eliana RuizNo ratings yet
- Propensity Scorimg AnalysisDocument8 pagesPropensity Scorimg AnalysisDrsaumyta MishraNo ratings yet
- First-Line Treatment of Metastatic Renal Cell Carcinoma: A Systematic Review and Network Meta-AnalysisDocument8 pagesFirst-Line Treatment of Metastatic Renal Cell Carcinoma: A Systematic Review and Network Meta-AnalysisDr. Alexandre SatoNo ratings yet
- Systemic Therapy in The Curative Treatment of Head and Neck Squamous Cell Cancer: A Systematic ReviewDocument11 pagesSystemic Therapy in The Curative Treatment of Head and Neck Squamous Cell Cancer: A Systematic ReviewLorena Sánchez PérezNo ratings yet
- Seminar: Fred R Hirsch, Giorgio V Scagliotti, James L Mulshine, Regina Kwon, Walter J Curran, Yi-Long Wu, Luis Paz-AresDocument13 pagesSeminar: Fred R Hirsch, Giorgio V Scagliotti, James L Mulshine, Regina Kwon, Walter J Curran, Yi-Long Wu, Luis Paz-AresseruniallisaaslimNo ratings yet
- Q 3 WedefDocument6 pagesQ 3 Wedefsupaidi97No ratings yet
- Theraphy RadDocument4 pagesTheraphy RadMega PuspitaNo ratings yet
- Vaginal Dose Is Associated With Toxicity in Image Guided Tandem Ring or Ovoid-Based BrachytherapyDocument7 pagesVaginal Dose Is Associated With Toxicity in Image Guided Tandem Ring or Ovoid-Based BrachytherapyFlor ZalazarNo ratings yet
- Update On Radiotherapy in Gynaecological Malignancies: ReviewDocument8 pagesUpdate On Radiotherapy in Gynaecological Malignancies: ReviewDesrha TangdiseruNo ratings yet
- Jamaoncology Miao 2022 Oi 220055 1670534730.29028Document10 pagesJamaoncology Miao 2022 Oi 220055 1670534730.29028Raul Matute MartinNo ratings yet
- Tca 12 2161Document9 pagesTca 12 2161hafidisara05No ratings yet
- Normal Newborn CareDocument49 pagesNormal Newborn CareIrfan MohammadNo ratings yet
- Daftar SingkatanDocument3 pagesDaftar SingkatanYohanes AdhityaNo ratings yet
- Xiaoli HuDocument12 pagesXiaoli HuYohanes AdhityaNo ratings yet
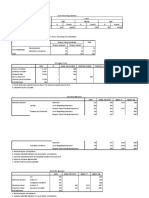
- Case Processing SummaryDocument2 pagesCase Processing SummaryYohanes AdhityaNo ratings yet
- MabuchiDocument13 pagesMabuchiYohanes AdhityaNo ratings yet
- TitiloyeDocument5 pagesTitiloyeYohanes AdhityaNo ratings yet
- CouvreurDocument10 pagesCouvreurYohanes AdhityaNo ratings yet
- TekalegnDocument14 pagesTekalegnYohanes AdhityaNo ratings yet
- MirzaDocument7 pagesMirzaYohanes AdhityaNo ratings yet
- SummaryDocument2 pagesSummaryYohanes AdhityaNo ratings yet
- Daftar Pustaka - EditDocument5 pagesDaftar Pustaka - EditYohanes AdhityaNo ratings yet
- Head Nursing Evaluation ToolDocument2 pagesHead Nursing Evaluation ToolDharline Abbygale Garvida Agullana100% (5)
- 7.2 PlasmapheresisDocument13 pages7.2 PlasmapheresisBALAJI100% (1)
- Hnca Physician Network Participation Request Form PDFDocument1 pageHnca Physician Network Participation Request Form PDFMalsom SingsonNo ratings yet
- A Standardized Endodontic Technique Utilizing Newly Designed Instruments and Filling Materials PDFDocument9 pagesA Standardized Endodontic Technique Utilizing Newly Designed Instruments and Filling Materials PDFCristian FernandoNo ratings yet
- Animals: Clinical Practice Guidelines: An Opinion of The Legal Implication To Veterinary MedicineDocument13 pagesAnimals: Clinical Practice Guidelines: An Opinion of The Legal Implication To Veterinary MedicinesamiNo ratings yet
- OsteomyelitisDocument18 pagesOsteomyelitisRizka Permana PutriNo ratings yet
- Black DeathDocument10 pagesBlack DeathKrisi KehayovaNo ratings yet
- 2016 Revised Standards For Clinical Dental Hygiene PracticeDocument16 pages2016 Revised Standards For Clinical Dental Hygiene PracticeElvira PurnamasariNo ratings yet
- CCC No: Ministry of Health Effective 01 October 2016 Viral Load Requisition FormDocument1 pageCCC No: Ministry of Health Effective 01 October 2016 Viral Load Requisition FormMigori ArtNo ratings yet
- 4.10.17final Clinical Trials Talk.4.10.2017 - 300526 - 284 - 30426 - v1Document67 pages4.10.17final Clinical Trials Talk.4.10.2017 - 300526 - 284 - 30426 - v1Mohammed HammedNo ratings yet
- BLUE-Protocol and FALLS-Protocol: Two Applications of Lung Ultrasound in The Critically IllDocument12 pagesBLUE-Protocol and FALLS-Protocol: Two Applications of Lung Ultrasound in The Critically IllChristiaan CordovaNo ratings yet
- Applied Kinesiology Essentials DR S Cuthbert Townsend Letter Jan.2016 PDFDocument5 pagesApplied Kinesiology Essentials DR S Cuthbert Townsend Letter Jan.2016 PDFdocerick87No ratings yet
- English For Nursing 2: Vocational English Teacher's BookDocument15 pagesEnglish For Nursing 2: Vocational English Teacher's BookSelina Nguyễn VuNo ratings yet
- Administering A Subcutaneous InjectionDocument2 pagesAdministering A Subcutaneous InjectionLiana Koh VillanuevaNo ratings yet
- Activity Design Mrsia 2018 Final BudgetDocument3 pagesActivity Design Mrsia 2018 Final BudgetRJay Mon MarcosNo ratings yet
- A Step by Step Guide To Mastering The OSCEsDocument20 pagesA Step by Step Guide To Mastering The OSCEsAl Imari60% (10)
- Clinical Management VHF Pocket BookDocument113 pagesClinical Management VHF Pocket BookZeljnaznanjaNo ratings yet
- A Clinicians Pearls Myths in Rheumatology 2Nd Edition John H Stone Full ChapterDocument67 pagesA Clinicians Pearls Myths in Rheumatology 2Nd Edition John H Stone Full Chapterclarence.terry830100% (6)
- Pathogenesis TBDocument39 pagesPathogenesis TBGede Eka Putra NugrahaNo ratings yet
- Ikam Bau TahiDocument17 pagesIkam Bau TahiAndre PrasetyooNo ratings yet
- CricothyroidotomyDocument38 pagesCricothyroidotomyAlsalman AnamNo ratings yet
- Project On Gaming EffectDocument19 pagesProject On Gaming EffectAnjali 9eNo ratings yet
- Chapter - 1: 1 - P A G e Measuring Patient Satisfaction Service of JRRMCHDocument39 pagesChapter - 1: 1 - P A G e Measuring Patient Satisfaction Service of JRRMCHMd Khaled NoorNo ratings yet
- ISHRS 20th Abstract Book 2012 Bahamas FinalDocument418 pagesISHRS 20th Abstract Book 2012 Bahamas FinalAlan J Bauman MDNo ratings yet
- Certificate of EligibilityDocument6 pagesCertificate of EligibilitySweet SimyunnNo ratings yet
- Overview of Nursing TheoriesDocument60 pagesOverview of Nursing TheoriestokzzNo ratings yet
- Endobronchial Tuberculosis An OverviewDocument5 pagesEndobronchial Tuberculosis An OverviewPramesti Fitria KNo ratings yet
- Guía de Diabetes y PsicosisDocument5 pagesGuía de Diabetes y PsicosiskarlunchoNo ratings yet
- HealOzone Brochure 01 PDFDocument5 pagesHealOzone Brochure 01 PDFAGNo ratings yet
- Final English 211c Part ADocument4 pagesFinal English 211c Part Aapi-341958041No ratings yet