You might also like
- SMJ October 2018 Mazzeo 113-118Document7 pagesSMJ October 2018 Mazzeo 113-118HantiukNo ratings yet
- Selenium Supplementation For Hashimoto SDocument73 pagesSelenium Supplementation For Hashimoto SHantiukNo ratings yet
- Mechanisms in Endocrinology Thyroid andDocument13 pagesMechanisms in Endocrinology Thyroid andHantiukNo ratings yet
- Primary Empty Sella Syndrome and The Prevalence of Hormonal DysregulationDocument9 pagesPrimary Empty Sella Syndrome and The Prevalence of Hormonal DysregulationHantiukNo ratings yet
- Frequency of Celiac Disease in PatientsDocument6 pagesFrequency of Celiac Disease in PatientsHantiukNo ratings yet
- Exaggerated Thelarche An Uncommon PresenDocument48 pagesExaggerated Thelarche An Uncommon PresenHantiukNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- SVTDocument31 pagesSVTAkbar IskandarNo ratings yet
- Allergic Contact DermatitisDocument12 pagesAllergic Contact DermatitisAzis BoenjaminNo ratings yet
- Comparative Efficacy and Acceptability META-ANALYSIS 2015Document11 pagesComparative Efficacy and Acceptability META-ANALYSIS 2015Alexandra CastellanosNo ratings yet
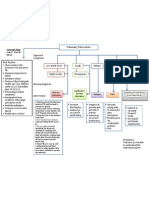
- Concept Map PTBDocument1 pageConcept Map PTBJoan Abardo100% (2)
- Parameters of The Model: Name Live Alpha Beta DescriptionDocument5 pagesParameters of The Model: Name Live Alpha Beta DescriptionAngga Prawira KautsarNo ratings yet
- Immnunology Notebook Chapter One: Innate ImmunityDocument45 pagesImmnunology Notebook Chapter One: Innate ImmunityJavier Alejandro Daza GalvánNo ratings yet
- Non-Cardiac Chest PainDocument5 pagesNon-Cardiac Chest PainRNo ratings yet
- Ncbi List of Books and Dental ArticlesDocument6 pagesNcbi List of Books and Dental ArticlesIulia Isacov0% (1)
- Bacteria Found in UrineDocument7 pagesBacteria Found in UrineAria DomingoNo ratings yet
- Laparoscopic Course: General Principles of Laparoscopy: Specific Aspects of Transperitoneal Access (R.Bollens)Document4 pagesLaparoscopic Course: General Principles of Laparoscopy: Specific Aspects of Transperitoneal Access (R.Bollens)Anuj MisraNo ratings yet
- Full Download Winninghams Critical Thinking Cases in Nursing 5th Edition Harding Solutions ManualDocument28 pagesFull Download Winninghams Critical Thinking Cases in Nursing 5th Edition Harding Solutions Manualnoahmya6100% (25)
- Disorders of Immunity Hypersensitivity Reactions: Dr. Mehzabin AhmedDocument25 pagesDisorders of Immunity Hypersensitivity Reactions: Dr. Mehzabin AhmedFrances FranciscoNo ratings yet
- Counseling TechniquesDocument60 pagesCounseling Techniquesdinalen0% (1)
- Textbook of Gynaecological OncologyDocument58 pagesTextbook of Gynaecological OncologyMarco Vinicio Benavides Osorto100% (2)
- Medical Biotechnology Multiple Choice Question (GuruKpo)Document13 pagesMedical Biotechnology Multiple Choice Question (GuruKpo)GuruKPO91% (11)
- 2020 Anaphylaxis JACI 2020Document42 pages2020 Anaphylaxis JACI 2020Peter Albeiro Falla CortesNo ratings yet
- D An Introduction: Physical Medicine and RehabilitationDocument33 pagesD An Introduction: Physical Medicine and RehabilitationChadNo ratings yet
- Festival Dance Lesson - Module 2 - P.E. 3rd Quarter PPT 2 of 2Document29 pagesFestival Dance Lesson - Module 2 - P.E. 3rd Quarter PPT 2 of 2Maria Fe VibarNo ratings yet
- Mandibulasr Truma ManagementDocument18 pagesMandibulasr Truma Managementjoal510No ratings yet
- HSBDocument4 pagesHSBCarlos WebsterNo ratings yet
- AQ4PDocument3 pagesAQ4PAhmed GaberNo ratings yet
- Behavioral Health Care Plan: Assessment DataDocument9 pagesBehavioral Health Care Plan: Assessment Dataapi-521018364No ratings yet
- Patient Wellbeing Assessment and Recovery Plan - Children and AdolescentsDocument12 pagesPatient Wellbeing Assessment and Recovery Plan - Children and AdolescentsSyedaNo ratings yet
- TM Joint PDFDocument16 pagesTM Joint PDFdhruvNo ratings yet
- Pukpuklo A Wealth in The SeaDocument2 pagesPukpuklo A Wealth in The SeaKrizha Angela NicolasNo ratings yet
- Wards and Departments in The Hospital NamingDocument4 pagesWards and Departments in The Hospital NamingSlebeww PetewNo ratings yet
- Acid Fast StainDocument3 pagesAcid Fast StainMartina MicicNo ratings yet
- IDP 11.13.19 11.14.19 Metal Implants White Paper - 0 PDFDocument152 pagesIDP 11.13.19 11.14.19 Metal Implants White Paper - 0 PDFVivek KhakharNo ratings yet
- Infusion PumpDocument14 pagesInfusion PumpSREEDEVI T SURESHNo ratings yet
- Acute Parenchymal Liver DiseaseDocument29 pagesAcute Parenchymal Liver Diseasejeevan ghimireNo ratings yet