You might also like
- AutoantibodiesDocument235 pagesAutoantibodiesMihai M100% (2)
- Surviving Cancer, COVID-19, and Disease: The Repurposed Drug RevolutionFrom EverandSurviving Cancer, COVID-19, and Disease: The Repurposed Drug RevolutionNo ratings yet
- EBMDocument636 pagesEBMDaniel SalaNo ratings yet
- ZZ ZZZZZZZZ ZZZZZZZZDocument2 pagesZZ ZZZZZZZZ ZZZZZZZZJanderick S EsguerraNo ratings yet
- On The Life of Asclepiades of BithyniaDocument20 pagesOn The Life of Asclepiades of BithyniaIsabel PlataNo ratings yet
- An Update On Menopause ManagementDocument10 pagesAn Update On Menopause ManagementJuan FranciscoNo ratings yet
- PE and HX Taking HandoutDocument11 pagesPE and HX Taking HandoutJoshua RivasNo ratings yet
- Evidence-Based Medicine: What It Can and Cannot Do: Goffredo Freddi and José Luis Romàn-PumarDocument4 pagesEvidence-Based Medicine: What It Can and Cannot Do: Goffredo Freddi and José Luis Romàn-PumarIan SeptiyanNo ratings yet
- Jop 18 1 Forssell 1Document24 pagesJop 18 1 Forssell 1Alejandra LorancaNo ratings yet
- Evidence BaseDocument10 pagesEvidence BaseblatchujosephNo ratings yet
- Evidence Based Medicine New ApprDocument15 pagesEvidence Based Medicine New ApprHalim SyahrilNo ratings yet
- Deloitte Personalised Medicine Analysis-PGx-ROIDocument32 pagesDeloitte Personalised Medicine Analysis-PGx-ROISimranjit SinghNo ratings yet
- Key Words: Evidence Based Medicine, Health, Patients, Decision MakingDocument11 pagesKey Words: Evidence Based Medicine, Health, Patients, Decision MakingSandiNo ratings yet
- Introduction To E B MDocument10 pagesIntroduction To E B Mدكتور محمودNo ratings yet
- Michael T. Greenwood - Acupuncture and Evidence-Based Medicine: A Philosophical CritiqueDocument12 pagesMichael T. Greenwood - Acupuncture and Evidence-Based Medicine: A Philosophical CritiqueSonyRed100% (1)
- What It Is and What It Is NotDocument4 pagesWhat It Is and What It Is NotshrikantNo ratings yet
- How Physicians Manage Medical Uncertainty: A Qualitative Study and Conceptual TaxonomyDocument17 pagesHow Physicians Manage Medical Uncertainty: A Qualitative Study and Conceptual TaxonomyAlexNo ratings yet
- PMC The Personalized Medicine Report Opportunity Challenges and The FutureDocument72 pagesPMC The Personalized Medicine Report Opportunity Challenges and The Futuretanveer kaurNo ratings yet
- Evidence-Based Public Health, Community Medicine, Preventive CareDocument8 pagesEvidence-Based Public Health, Community Medicine, Preventive Carehydra89No ratings yet
- Evidence-Based Medicine: An Obstetrician and Gynaecologist's PerspectiveDocument8 pagesEvidence-Based Medicine: An Obstetrician and Gynaecologist's PerspectiveRené RodriguezNo ratings yet
- Evidence Based Medicine: What It Is and What It Isn'tDocument3 pagesEvidence Based Medicine: What It Is and What It Isn'tCristian EstradaNo ratings yet
- Alternative and Orthodox Medicine and The " " Principle: Letter To The EditorDocument2 pagesAlternative and Orthodox Medicine and The " " Principle: Letter To The EditorBiol. Miguel Angel Gutiérrez DomínguezNo ratings yet
- 6.1 Evidence Based Medicine (EBM) Is The Conscientious, Explicit, Judicious and ReasonableDocument5 pages6.1 Evidence Based Medicine (EBM) Is The Conscientious, Explicit, Judicious and Reasonablefraol alemuNo ratings yet
- Emergency Department Management of Cellulitis and Other Skin andDocument24 pagesEmergency Department Management of Cellulitis and Other Skin andJesus CedeñoNo ratings yet
- Bensing 00 Bridgingthegap PDFDocument10 pagesBensing 00 Bridgingthegap PDFJuan Carlos JaramilloNo ratings yet
- Person Med EMBO RepDocument4 pagesPerson Med EMBO Reptomtom1010No ratings yet
- MBE Controversias PDFDocument9 pagesMBE Controversias PDFAdriana M Rueda CastellanosNo ratings yet
- Editorials: Evidence Based Medicine: What It Is and What It Isn'tDocument4 pagesEditorials: Evidence Based Medicine: What It Is and What It Isn'tDanymilosOroNo ratings yet
- Pediatric and Neonatal Individualized Medicine: Care and Cure For Each and EveryoneDocument4 pagesPediatric and Neonatal Individualized Medicine: Care and Cure For Each and EveryoneMugo SaktiNo ratings yet
- What Is The Value of Oncology Medicines?: CommentaryDocument4 pagesWhat Is The Value of Oncology Medicines?: CommentaryIván RodríguezNo ratings yet
- EBM and MeShDocument2 pagesEBM and MeShRobert ImgratNo ratings yet
- Evidence Based Medicine in Neurosurgery PDFDocument5 pagesEvidence Based Medicine in Neurosurgery PDFsalikaabrarNo ratings yet
- BR 7 1 3 PDFDocument3 pagesBR 7 1 3 PDFalejandro.rivera2570No ratings yet
- Integrating CAM Practices Into The Conventional Health Systems (Integrative Medicine)Document12 pagesIntegrating CAM Practices Into The Conventional Health Systems (Integrative Medicine)Joud D.No ratings yet
- Private and Public Area in BiomedicalDocument2 pagesPrivate and Public Area in BiomedicalHas SimNo ratings yet
- 31200753: Sepsis Personalization V ProtocolizationDocument6 pages31200753: Sepsis Personalization V ProtocolizationLuis Enrique Caceres AlavrezNo ratings yet
- Precision MedicineDocument23 pagesPrecision Medicinecelecosib100% (1)
- A New Vision of Definition, Commentary, and Understanding in Clinical and Translational MedicineDocument3 pagesA New Vision of Definition, Commentary, and Understanding in Clinical and Translational MedicineMahmoud HakimNo ratings yet
- Evidence Based Medicine Practice With Their Evolution and Application in Current Health SectorDocument5 pagesEvidence Based Medicine Practice With Their Evolution and Application in Current Health SectorInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 2017 Embracing Uncertainty To Advance Diagnosis inDocument2 pages2017 Embracing Uncertainty To Advance Diagnosis inpainfree888No ratings yet
- Ethical Dilemmas in Communicating Bad NewsDocument5 pagesEthical Dilemmas in Communicating Bad NewsLiliana RogozeaNo ratings yet
- REFLECTIONDocument1 pageREFLECTIONMiks SahurdaNo ratings yet
- Evidence-Based Medicine: David L. SackettDocument3 pagesEvidence-Based Medicine: David L. SackettNicolas MarinNo ratings yet
- A Narrative Review of Defensive Medical Practice in PsychiatryDocument1 pageA Narrative Review of Defensive Medical Practice in PsychiatryyehfanweiNo ratings yet
- Doctors in Society: Medical Professionalism in A Changing WorldDocument6 pagesDoctors in Society: Medical Professionalism in A Changing Worldishu sNo ratings yet
- The Human Element vs. The Standardization of Medical Care - Books & IdeasDocument11 pagesThe Human Element vs. The Standardization of Medical Care - Books & IdeasAna Belen Tapia GómezNo ratings yet
- Problems in The Evidence'' of Evidence-Based Medicine'': Special ArticleDocument7 pagesProblems in The Evidence'' of Evidence-Based Medicine'': Special ArticleninhodesoyaNo ratings yet
- Changing Our Diagnostic Paradigm Part II Movement System Diagnostic ClassificationDocument11 pagesChanging Our Diagnostic Paradigm Part II Movement System Diagnostic ClassificationSandro PerilloNo ratings yet
- Commentary: Improving The Medical Decision-Making Process by John E. WennbergDocument8 pagesCommentary: Improving The Medical Decision-Making Process by John E. WennbergGee ThaNo ratings yet
- Complementary Therapies in Palliative Cancer Care: Edzard ErnstDocument5 pagesComplementary Therapies in Palliative Cancer Care: Edzard ErnstDwi CahyoNo ratings yet
- MM20802-EPID IN CLINICAL PRACTICE Y2.v2Document18 pagesMM20802-EPID IN CLINICAL PRACTICE Y2.v2danishNo ratings yet
- Rational Decision Making in MedicineDocument11 pagesRational Decision Making in MedicineSanti AraratNo ratings yet
- Patient Safety USMLEDocument18 pagesPatient Safety USMLEsdroyafmc100% (2)
- EBM Has Not Only Called Out The Problems But Offered SolutionsDocument3 pagesEBM Has Not Only Called Out The Problems But Offered SolutionsYael NepoNo ratings yet
- Primary Health Care and Family MedicineDocument5 pagesPrimary Health Care and Family MedicineCATHERINE HAYNESNo ratings yet
- Nejm CER Consent KassDocument3 pagesNejm CER Consent KassSasha Hidayat FullNo ratings yet
- Why Do Ineffective Treatments Seem HelpfullDocument7 pagesWhy Do Ineffective Treatments Seem HelpfullRazvan UngureanuNo ratings yet
- 1 - Outcomes ResearchDocument12 pages1 - Outcomes ResearchMauricio Ruiz MoralesNo ratings yet
- Artifcial Intelligence and Machine Learning in Precision and GenomicDocument18 pagesArtifcial Intelligence and Machine Learning in Precision and GenomicAditya DebnathNo ratings yet
- Ten Common Questions (And Their Answers) On Medical FutilityDocument17 pagesTen Common Questions (And Their Answers) On Medical FutilitycindyNo ratings yet
- Clinical and Translational Science From Bench Bedside To Global VillageDocument4 pagesClinical and Translational Science From Bench Bedside To Global VillageSamNo ratings yet
- CHAPTER 7 - Value of Medical Lab Science PersonnelDocument8 pagesCHAPTER 7 - Value of Medical Lab Science PersonnelHannahjoy anainNo ratings yet
- Rational fluid and volume therapy in anaesthesia and intensive care medicineFrom EverandRational fluid and volume therapy in anaesthesia and intensive care medicineNo ratings yet
- Effectiveness of Manual Therapies: The UK Evidence ReportDocument40 pagesEffectiveness of Manual Therapies: The UK Evidence Reportapi-286958060No ratings yet
- Test For Eng 13 Reading and Writing (ANSWERS)Document3 pagesTest For Eng 13 Reading and Writing (ANSWERS)Joseph Santos San JuanNo ratings yet
- Difference Between Industrial Wastewater and Municipal WastewaterDocument11 pagesDifference Between Industrial Wastewater and Municipal Wastewatertawsifamin19896% (25)
- BrackDocument4 pagesBrackkoebra211No ratings yet
- JRCRS ARTICLE Comparison of SWDDocument10 pagesJRCRS ARTICLE Comparison of SWDdr musafirNo ratings yet
- HPLC Methods For Folic AcidDocument21 pagesHPLC Methods For Folic AcidSowmya SagarNo ratings yet
- Lydia Eloise HallDocument9 pagesLydia Eloise HallNikki Rivera100% (1)
- Hypotonic and Hypertonic Contractions and Precipitate LabourDocument3 pagesHypotonic and Hypertonic Contractions and Precipitate LabourRebecca ApeladoNo ratings yet
- Ramsay Hunt SyndromeDocument5 pagesRamsay Hunt SyndromeriyanNo ratings yet
- Official Control of Food Safety in Lithuania: Import and ExportDocument33 pagesOfficial Control of Food Safety in Lithuania: Import and ExportAbdi HajiNo ratings yet
- ThumbDriver Clinican Fitting InstructionsDocument4 pagesThumbDriver Clinican Fitting InstructionsGómez Torres Javier JesúsNo ratings yet
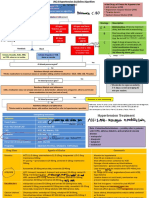
- Obesity Treatment, Beyond The Guidelines Practical Suggestions For Clinical PracticeDocument2 pagesObesity Treatment, Beyond The Guidelines Practical Suggestions For Clinical PracticeKharen VerjelNo ratings yet
- 44-261 Ammonium ChlorideDocument31 pages44-261 Ammonium Chloridedaniel abiaNo ratings yet
- Mock Test For Physical Education XII For Examination 2023 - Day 2 - LowDocument18 pagesMock Test For Physical Education XII For Examination 2023 - Day 2 - LowLakshmikanta BanerjeeNo ratings yet
- GSK Report 2008 FullDocument212 pagesGSK Report 2008 FullSerhat ERTANNo ratings yet
- Depression in Filipino YouthDocument8 pagesDepression in Filipino Youthjohn patrick acebuche100% (2)
- Diagnostic Test: Control No. Location ConditionDocument15 pagesDiagnostic Test: Control No. Location ConditiondwellerNo ratings yet
- Standardized Color-Coding Solution Labeling in The Operating RoomDocument3 pagesStandardized Color-Coding Solution Labeling in The Operating Roomcumar cabdicazizNo ratings yet
- MAPC 2nd Year Assignments 2019-20Document13 pagesMAPC 2nd Year Assignments 2019-20Jayee's GalleryNo ratings yet
- Manual: Department of DefenseDocument63 pagesManual: Department of DefenseAnonymous fmC3PqkNo ratings yet
- Method Statement For Cement Wall Plastering-1Document8 pagesMethod Statement For Cement Wall Plastering-1md_rehan_2No ratings yet
- ATLAS HSE Management System DescriptionDocument10 pagesATLAS HSE Management System DescriptionGary DrimieNo ratings yet
- 2014 JNC 8 Hypertension - 221105 - 134757Document3 pages2014 JNC 8 Hypertension - 221105 - 134757Ei lessonNo ratings yet
- Stress Echo Quick ManualDocument3 pagesStress Echo Quick ManualMayrina NDNo ratings yet
- ZOP - Newsletter - January 2011Document7 pagesZOP - Newsletter - January 2011MZALENDO.NETNo ratings yet
- Encyclopedia of Entomology 2nd EditionDocument2 pagesEncyclopedia of Entomology 2nd EditionexjupiterNo ratings yet