You might also like
- Treatment Planning Single Maxillary Anterior Implants for DentistsFrom EverandTreatment Planning Single Maxillary Anterior Implants for DentistsNo ratings yet
- Multidisciplinary Treatment of A Subgingivally Fractured Tooth With Indirect Restoration A Case ReportDocument5 pagesMultidisciplinary Treatment of A Subgingivally Fractured Tooth With Indirect Restoration A Case ReportEriana 梁虹绢 SutonoNo ratings yet
- Jurnal GicDocument6 pagesJurnal GicHusnul KhatimahNo ratings yet
- Ijda July-Sep 2015Document5 pagesIjda July-Sep 2015bhaskaracharya dontabhaktuniNo ratings yet
- 724 2683 4 PB PDFDocument2 pages724 2683 4 PB PDFCristi GaidurNo ratings yet
- MOLARDocument8 pagesMOLARJuan Carlos MeloNo ratings yet
- 6.clinical Case ReportMultidisciplinary Approach For Rehabilitation of Debilitated Anterior ToothDocument6 pages6.clinical Case ReportMultidisciplinary Approach For Rehabilitation of Debilitated Anterior ToothSahana RangarajanNo ratings yet
- Restoration of Esthetics And.... POST COREDocument6 pagesRestoration of Esthetics And.... POST COREnadeemNo ratings yet
- Hemisection A Treatment Option For An Endodontically Treated Molar With Vertical Root FractureDocument3 pagesHemisection A Treatment Option For An Endodontically Treated Molar With Vertical Root FracturePaulo CastroNo ratings yet
- Multidisciplinary Approach For The Treatment of Horizontal Root-Fractured Maxillary Anterior TeethDocument11 pagesMultidisciplinary Approach For The Treatment of Horizontal Root-Fractured Maxillary Anterior TeethGülbike DemirelNo ratings yet
- Oz 2006Document5 pagesOz 2006ayoubNo ratings yet
- BELOBROV I 2008 Conservative Treatment of A Cervical Horizontal Root Fracture and A Complicated Crown Fracture A Case ReportDocument5 pagesBELOBROV I 2008 Conservative Treatment of A Cervical Horizontal Root Fracture and A Complicated Crown Fracture A Case ReportaactinoNo ratings yet
- Case ReportDocument8 pagesCase ReportKeyla Paola De La Hoz FonsecaNo ratings yet
- 2007 - Intrusion of Overerupted Molars byDocument7 pages2007 - Intrusion of Overerupted Molars byTien Li AnNo ratings yet
- Miyahira2008 - Miniplates As Skeletal Anchorage For Treating Mandibular Second Molar ImpactionsDocument4 pagesMiyahira2008 - Miniplates As Skeletal Anchorage For Treating Mandibular Second Molar ImpactionsNathália LopesNo ratings yet
- Management of Transverse Root Fracture by Dowel - Inlay: A Case ReportDocument9 pagesManagement of Transverse Root Fracture by Dowel - Inlay: A Case ReportAdzhani SabilaNo ratings yet
- Case ReportDocument5 pagesCase ReportWainaianaNo ratings yet
- Maturogenesis of A Complicated Crown Fracture: A Case Report With 8 Years Follow-UpDocument4 pagesMaturogenesis of A Complicated Crown Fracture: A Case Report With 8 Years Follow-UpKIH 20162017No ratings yet
- Implicaciones Periodontales Del Tratamiento Quirúrgico-OrtodónticoDocument9 pagesImplicaciones Periodontales Del Tratamiento Quirúrgico-OrtodónticoAlfredo NovoaNo ratings yet
- AAE Newsletter Covers Endodontic TreatmentDocument6 pagesAAE Newsletter Covers Endodontic TreatmentMehwish MunawarNo ratings yet
- Decoronation of An Ankylosed Permanent Incisor: Alveolar Ridge Preservation and Rehabilitation by An Implant Supported Porcelain CrownDocument4 pagesDecoronation of An Ankylosed Permanent Incisor: Alveolar Ridge Preservation and Rehabilitation by An Implant Supported Porcelain CrownJuan Carlos MeloNo ratings yet
- Ejpd 2017 1 5Document5 pagesEjpd 2017 1 5Mariatun Zahro NasutionNo ratings yet
- Orthodontic Treatment in A Periodontal Patient With Pathologic Migration of Anterior TeethDocument9 pagesOrthodontic Treatment in A Periodontal Patient With Pathologic Migration of Anterior TeethMárcio LMSNo ratings yet
- TMP 371 BDocument4 pagesTMP 371 BFrontiersNo ratings yet
- 16 Box Loop and 3 Impacted TeethDocument12 pages16 Box Loop and 3 Impacted TeethtomografiaquinNo ratings yet
- The Treatment Strategy of An Oblique Complicated Crownroot Fracturecase Report PDC 1000110Document4 pagesThe Treatment Strategy of An Oblique Complicated Crownroot Fracturecase Report PDC 1000110Isabel Escobar MinotasNo ratings yet
- Factors Determining Correction of Malpositioned Teeth Using Cast Post Core RestorationsDocument3 pagesFactors Determining Correction of Malpositioned Teeth Using Cast Post Core RestorationsM Ghazy FajruyumaNo ratings yet
- A Biological Approach To Crown Fracture Fracture RDocument5 pagesA Biological Approach To Crown Fracture Fracture Rhendra cahyaditaNo ratings yet
- Biological approach for management of anterior tooth trauma: Triple case reportDocument7 pagesBiological approach for management of anterior tooth trauma: Triple case reportZarah Hannah Leah DalmacioNo ratings yet
- Jurnal Kasus Tambahan 3 - Khairin Yonni (12730)Document6 pagesJurnal Kasus Tambahan 3 - Khairin Yonni (12730)Khairin YonniNo ratings yet
- 2016 Salvation of Severely Fractured Anterior Tooth An Orthodontic ApproachDocument4 pages2016 Salvation of Severely Fractured Anterior Tooth An Orthodontic ApproachRajesh GyawaliNo ratings yet
- Management of Fracture Tooth Fragment Reattachment: Case ReportDocument7 pagesManagement of Fracture Tooth Fragment Reattachment: Case Reportwaleed MagidNo ratings yet
- Intentional Re-Plantation of A Vertically Fractured Tooth Repaired With An Adhesive ResinDocument10 pagesIntentional Re-Plantation of A Vertically Fractured Tooth Repaired With An Adhesive Resinveena rNo ratings yet
- Cdej 4 49Document4 pagesCdej 4 49TridddNo ratings yet
- 10 1111@jerd 12466Document4 pages10 1111@jerd 12466NémethBálintNo ratings yet
- Sept2020 ToothDocument3 pagesSept2020 ToothTrina ViskhawatNo ratings yet
- IntJOralHealthDent 7-2-146 150Document5 pagesIntJOralHealthDent 7-2-146 150Neha MehtaNo ratings yet
- Decoronation For The Management of An Ankylosed Young Permanent ToothDocument5 pagesDecoronation For The Management of An Ankylosed Young Permanent ToothCesar Augusto Rojas MachucaNo ratings yet
- Oh 2010Document5 pagesOh 2010gbaez.88No ratings yet
- Asds 02 0215Document3 pagesAsds 02 02156mf9jf6h99No ratings yet
- Esthetic and Endodontic Management of A Deep Crown-Root Fracture of A Maxillary Central IncisorDocument4 pagesEsthetic and Endodontic Management of A Deep Crown-Root Fracture of A Maxillary Central IncisordrgozanNo ratings yet
- Management of Ectopically Erupting MaxillaryDocument7 pagesManagement of Ectopically Erupting MaxillaryLiliana Aguilar VillarrealNo ratings yet
- Management of Severe Dento-Alveolar Traumatic Injuries in A 9-YeaDocument7 pagesManagement of Severe Dento-Alveolar Traumatic Injuries in A 9-YeasintaznNo ratings yet
- Articulo AlexDocument2 pagesArticulo AlexGustavo Gonzales ChavezNo ratings yet
- Immediate Dentoalveolar RestorationDocument8 pagesImmediate Dentoalveolar RestorationДмитрий ЦененкоNo ratings yet
- Marsupialização Tracionamento CistodentigeroDocument10 pagesMarsupialização Tracionamento CistodentigeroLucas SantiagoNo ratings yet
- Zachrisson2004 Management of Missing Maxillary Anterior Teeth With Emphasis On AutotransplantationDocument5 pagesZachrisson2004 Management of Missing Maxillary Anterior Teeth With Emphasis On AutotransplantationplsssssNo ratings yet
- Reimplantation of Avulsed Teeth After Dry Storage For One WeekDocument5 pagesReimplantation of Avulsed Teeth After Dry Storage For One WeekHesti RahayuNo ratings yet
- Pedo JurnalDocument5 pagesPedo JurnalAngelinaNo ratings yet
- Controlled Tooth Movement To Correct An Iatrogenic Problem: Case ReportDocument8 pagesControlled Tooth Movement To Correct An Iatrogenic Problem: Case ReportElla GolikNo ratings yet
- Impaksi GigiDocument3 pagesImpaksi GigiKarma YogaNo ratings yet
- Extrusion Splint Technique in Management of Dental Trauma: A Case ReportDocument5 pagesExtrusion Splint Technique in Management of Dental Trauma: A Case ReportdrvarunmalhotraNo ratings yet
- Forced Eruption of Adjoining Maxillary Premolars Using A Removable Orthodontic Appliance: A Case ReportDocument4 pagesForced Eruption of Adjoining Maxillary Premolars Using A Removable Orthodontic Appliance: A Case Reportikeuchi_ogawaNo ratings yet
- Chiu 2015 BimaxillaryDocument36 pagesChiu 2015 BimaxillaryMax FerNo ratings yet
- Tooth TtriyionDocument5 pagesTooth TtriyionDhanasriNo ratings yet
- Severe Crowding and A Dilacerated Maxillary Central Incisor in An AdolescentDocument9 pagesSevere Crowding and A Dilacerated Maxillary Central Incisor in An AdolescentDaneyi Giraldo LoaizaNo ratings yet
- 2 PDFDocument4 pages2 PDFPutri AmaliaNo ratings yet
- ArtigoDocument5 pagesArtigoCarolina DezanNo ratings yet
- Complete Dentures Opposing Natural TeethDocument8 pagesComplete Dentures Opposing Natural TeethMaqbul AlamNo ratings yet
- Immediate Natural Tooth Pontic - A Case ReportDocument3 pagesImmediate Natural Tooth Pontic - A Case ReportInternational Organization of Scientific Research (IOSR)No ratings yet
- Factory made uPVC windows installationDocument2 pagesFactory made uPVC windows installationAmit Singh100% (2)
- Course Progression Map For 2021 Commencing Students: E3001 Bachelor of Engineering (Honours) Common First YearDocument21 pagesCourse Progression Map For 2021 Commencing Students: E3001 Bachelor of Engineering (Honours) Common First YearNguyễn An KhoaNo ratings yet
- MD R2 Nastran Release GuideDocument276 pagesMD R2 Nastran Release GuideMSC Nastran BeginnerNo ratings yet
- Bio-Sil ULTRA 1050: Medically Pure Platinum-Cured Silicone Tubing With An Ultra-Smooth Inner SurfaceDocument2 pagesBio-Sil ULTRA 1050: Medically Pure Platinum-Cured Silicone Tubing With An Ultra-Smooth Inner SurfaceLari GrossiNo ratings yet
- Guide to Quality Control Arrangements on SeedsDocument15 pagesGuide to Quality Control Arrangements on SeedsArun Kumar100% (1)
- Stereochemistry MSCDocument29 pagesStereochemistry MSCBapu Thorat50% (2)
- Petford & Atherton., 1996Document31 pagesPetford & Atherton., 1996Ivan Hagler Becerra VasquezNo ratings yet
- Week 7: Nurses Role in Disaster: Home Mitigation and PreparednessDocument10 pagesWeek 7: Nurses Role in Disaster: Home Mitigation and PreparednessRose Ann LacuarinNo ratings yet
- Practice Quiz M1 (Ungraded) - MergedDocument22 pagesPractice Quiz M1 (Ungraded) - MergedAbdullah Abdullah100% (1)
- Construction Site PremisesDocument78 pagesConstruction Site PremisesDrew B Mrtnz67% (6)
- Adding True Bypass To A Vintage Big MuffDocument8 pagesAdding True Bypass To A Vintage Big MuffOliver SuttonNo ratings yet
- Foreign Body Airway ObstructionDocument6 pagesForeign Body Airway ObstructionReeja RajeshNo ratings yet
- FIKE RD Combo With Relief ValvesDocument11 pagesFIKE RD Combo With Relief ValvesAnkit GandhiNo ratings yet
- General Description: Effective Distance Depends On Antenna, Tag and EnvironmentDocument2 pagesGeneral Description: Effective Distance Depends On Antenna, Tag and EnvironmentSHASHANK BHUSHANNo ratings yet
- Columbus Files Motion To Dismiss Bankruptcy Claim by Latitude Five25 OwnersDocument38 pagesColumbus Files Motion To Dismiss Bankruptcy Claim by Latitude Five25 OwnersWSYX/WTTENo ratings yet
- Flacs CFD ManualDocument658 pagesFlacs CFD ManualCyanNo ratings yet
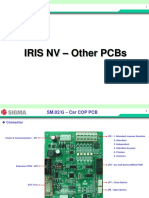
- 07 IRIS NV PCB OtherDocument15 pages07 IRIS NV PCB OtherArnaldo cordovaNo ratings yet
- Ras Abu Aboud Stadium Daily Report 040 (20190613)Document4 pagesRas Abu Aboud Stadium Daily Report 040 (20190613)tuan50% (2)
- SR. NO. Capacity/Descirption of Machine Client: A.C. Generator StatorsDocument5 pagesSR. NO. Capacity/Descirption of Machine Client: A.C. Generator Statorsmtj4uNo ratings yet
- Hero LetterDocument3 pagesHero LetterArunachalam Muthiah0% (1)
- Zenopus ClassicDocument32 pagesZenopus Classicserenity42No ratings yet
- Well Rounded.: 360 CassetteDocument12 pagesWell Rounded.: 360 CassetteMonty Va Al MarNo ratings yet
- RCS England Trainees Guide To A Quality Improvement Project 2021Document17 pagesRCS England Trainees Guide To A Quality Improvement Project 2021Wee K WeiNo ratings yet
- Liebert AC4 Controller ManualDocument88 pagesLiebert AC4 Controller ManualGreg WilliamsNo ratings yet
- Rules For The CertificationDocument84 pagesRules For The CertificationhdelriovNo ratings yet
- Seminar Application of Nitrous Oxide in AutomobilesDocument20 pagesSeminar Application of Nitrous Oxide in AutomobilesSaikat BadyakarNo ratings yet
- S2 Papers FinalizedDocument149 pagesS2 Papers FinalizedRaffles HolmesNo ratings yet
- Erotic MassageDocument113 pagesErotic MassageMahmoud El Mohamdy75% (4)
- Reverse Phrase Action Camera LightsDocument40 pagesReverse Phrase Action Camera LightsDINDO AzucenaNo ratings yet
- The Picture of Dorian GrayDocument137 pagesThe Picture of Dorian GrayАнгелаС.No ratings yet