You might also like
- An Analysis of Impact of Antenatl Care in Reducing Maternal Mortality RateDocument46 pagesAn Analysis of Impact of Antenatl Care in Reducing Maternal Mortality RateUsman Ahmad TijjaniNo ratings yet
- Ed Post Lab Heat of Formation of NaClDocument4 pagesEd Post Lab Heat of Formation of NaClEdimar ManlangitNo ratings yet
- Building A Pentesting Lab For Wireless Networks - Sample ChapterDocument29 pagesBuilding A Pentesting Lab For Wireless Networks - Sample ChapterPackt PublishingNo ratings yet
- Medical Tourism in IndiaDocument39 pagesMedical Tourism in IndiaAkhil Choudhary0% (1)
- Zygosaccharomyces James2011Document11 pagesZygosaccharomyces James2011edson escamillaNo ratings yet
- N2 V Operare ManualDocument370 pagesN2 V Operare Manualramiro0001No ratings yet
- Community Health NursingDocument23 pagesCommunity Health Nursingcoy008No ratings yet
- Pedoman Internal Program KRRDocument19 pagesPedoman Internal Program KRRemy nurhayatiNo ratings yet
- Thesis 1asddddddddddddddddddddddddddddddDocument81 pagesThesis 1asddddddddddddddddddddddddddddddKR Alegre100% (3)
- Chapter One Background of The StudyDocument43 pagesChapter One Background of The StudyUsman Ahmad Tijjani100% (1)
- Research Proposal Social Health and Development: Population-Based Managed Care (PBMC) Is A Management Technique DesignedDocument10 pagesResearch Proposal Social Health and Development: Population-Based Managed Care (PBMC) Is A Management Technique DesignedJaved HassanNo ratings yet
- Ranking of Sustainable Medical Tourism Destinations in Iran: An Integrated Approach Using Fuzzy SWARA-PROMETHEEDocument32 pagesRanking of Sustainable Medical Tourism Destinations in Iran: An Integrated Approach Using Fuzzy SWARA-PROMETHEEBolaji OdegbesanNo ratings yet
- Human Resources For HealthDocument7 pagesHuman Resources For HealthclaramaharaniNo ratings yet
- Finalized HSR Group Assignment GMPH Students SDocument21 pagesFinalized HSR Group Assignment GMPH Students Shabtamu birhanuNo ratings yet
- Integrating Oral Health Care Into Primary Health Care SystemDocument8 pagesIntegrating Oral Health Care Into Primary Health Care SystemDiana AyuNo ratings yet
- IJTMGH Volume 5 Issue 3 Pages 77-83Document7 pagesIJTMGH Volume 5 Issue 3 Pages 77-83Iman AzrbjNo ratings yet
- KDC Report 1juneDocument19 pagesKDC Report 1juneHarshada BhaleraoNo ratings yet
- The Knowledge, Ability, and Skills of Primary Health Care Providers in SEANERN Countries: A Multi-National Cross-Sectional StudyDocument8 pagesThe Knowledge, Ability, and Skills of Primary Health Care Providers in SEANERN Countries: A Multi-National Cross-Sectional StudyAzubeda SaidiNo ratings yet
- Transport and Communication Systems in Health Services: Tropical Doctor August 1977Document5 pagesTransport and Communication Systems in Health Services: Tropical Doctor August 1977mohit7898No ratings yet
- Oti2024 9982661Document9 pagesOti2024 9982661NataliaNo ratings yet
- LJM 5 4873Document8 pagesLJM 5 4873Ashu TyagiNo ratings yet
- Health Care Services in Saudi Arabia: Past, Present and FutureDocument6 pagesHealth Care Services in Saudi Arabia: Past, Present and FutureNisrin SaudNo ratings yet
- Manila DeclarationDocument6 pagesManila DeclarationJorge TignoNo ratings yet
- Factors Influencing Health Service Utilization in Ishaka Division, Bushenyi-Ishaka Municipality Insights and ImplicationsDocument11 pagesFactors Influencing Health Service Utilization in Ishaka Division, Bushenyi-Ishaka Municipality Insights and ImplicationsKIU PUBLICATION AND EXTENSIONNo ratings yet
- Project Proposal (IFMSA APRM 2012 Bangladesh)Document15 pagesProject Proposal (IFMSA APRM 2012 Bangladesh)Renzo R. GuintoNo ratings yet
- 6546 27022 1 PBDocument22 pages6546 27022 1 PBascarolineeNo ratings yet
- Assessment of Interventions To Attract and Retain Health Workers in Rural Zambia - A Discrete Choice ExperimentDocument12 pagesAssessment of Interventions To Attract and Retain Health Workers in Rural Zambia - A Discrete Choice ExperimentJace AlacapaNo ratings yet
- Komunitas IngDocument6 pagesKomunitas IngIngca ClaudiaNo ratings yet
- Emrpub 2012 en 1362 PDFDocument82 pagesEmrpub 2012 en 1362 PDFachysfNo ratings yet
- Evaluating Medical Tourism WhitepaperDocument8 pagesEvaluating Medical Tourism WhitepaperAssia MDellaNo ratings yet
- 1 s2.0 S187603411200175X Main PDFDocument6 pages1 s2.0 S187603411200175X Main PDFRiza Ikhsan MuliaNo ratings yet
- B.Sc. Handbook 2018-21Document59 pagesB.Sc. Handbook 2018-21Manisha NishaNo ratings yet
- Health Equity and Migrants in The Greater Mekong SubregionDocument11 pagesHealth Equity and Migrants in The Greater Mekong SubregionRafif DaffaNo ratings yet
- Global Standards For Health Promoting Schools Who UnescoDocument12 pagesGlobal Standards For Health Promoting Schools Who UnescoDavidNo ratings yet
- Barriers To Nurse - Patient Communication in Saudi Arabia: An Integrative ReviewDocument10 pagesBarriers To Nurse - Patient Communication in Saudi Arabia: An Integrative Reviewmark3dasaNo ratings yet
- Psikologi Faal Pertemuan 11Document3 pagesPsikologi Faal Pertemuan 11Shenina KnightleyNo ratings yet
- Primary Health Care in Jamkhed, IndiaDocument5 pagesPrimary Health Care in Jamkhed, IndiaJay WalleNo ratings yet
- Assessment of Knowledge Among ASHAs in The DeliverDocument7 pagesAssessment of Knowledge Among ASHAs in The DeliverShilpu RtwNo ratings yet
- Training Needs Assessment For Nurses in Sennar State, Sudan: Cross Sectional StudyDocument12 pagesTraining Needs Assessment For Nurses in Sennar State, Sudan: Cross Sectional Studyhikmat pramajatiNo ratings yet
- Icehsr, 2022Document128 pagesIcehsr, 2022Aliza KhanNo ratings yet
- PacistanDocument7 pagesPacistanKonstantinos KokorasNo ratings yet
- Determinants of Fitness Level Influencing The Morbidity Rate of Palembang's Hajj PilgrimsDocument12 pagesDeterminants of Fitness Level Influencing The Morbidity Rate of Palembang's Hajj PilgrimsSessa MagabeNo ratings yet
- Role of International Agancies in Public HealthDocument39 pagesRole of International Agancies in Public Healthmariagulalai2No ratings yet
- TASK 9 Kajang Local PlanDocument30 pagesTASK 9 Kajang Local PlanKhairussaadah MisnanNo ratings yet
- 4 Jurnal Alotaibi 2019Document16 pages4 Jurnal Alotaibi 2019Charis MurwadiNo ratings yet
- Covid-19 Online Cross-Training ProgramDocument13 pagesCovid-19 Online Cross-Training ProgramIJAR JOURNALNo ratings yet
- The Health Workforce Crisis in Bangladesh: Shortage, Inappropriate Skill-Mix and Inequitable DistributionDocument8 pagesThe Health Workforce Crisis in Bangladesh: Shortage, Inappropriate Skill-Mix and Inequitable DistributionMohammad Mizanur RahmanNo ratings yet
- Evaluating Food Safety Knowledge and Practices Among Foodservice Staff in Al Madinah Hospitals, Saudi ArabiaDocument19 pagesEvaluating Food Safety Knowledge and Practices Among Foodservice Staff in Al Madinah Hospitals, Saudi ArabiaAiza ConchadaNo ratings yet
- Jurnal PDFDocument6 pagesJurnal PDFepe iniNo ratings yet
- PDF-006506 Travel HealthDocument6 pagesPDF-006506 Travel Healthjean rumveyeNo ratings yet
- One Health Principles and ConceptsDocument116 pagesOne Health Principles and ConceptsRapchel EstrellaNo ratings yet
- RCSI Bahrain ConnectED Newsletter Winter 2022-23Document32 pagesRCSI Bahrain ConnectED Newsletter Winter 2022-23Yousif YousifNo ratings yet
- Egypt: Health Sector ReformDocument16 pagesEgypt: Health Sector Reformdevon2610No ratings yet
- Validity and Reliability of Turkish Version of Hospital Survey On Patient Safety Culture and Perception of Patient Safety in Public Hospitals in TurkeyDocument9 pagesValidity and Reliability of Turkish Version of Hospital Survey On Patient Safety Culture and Perception of Patient Safety in Public Hospitals in TurkeyReski Wahyuningsih NurNo ratings yet
- The Effect of Patient Safety Education On Undergraduate Nursing Students Patient Safety CompetenciesDocument6 pagesThe Effect of Patient Safety Education On Undergraduate Nursing Students Patient Safety CompetenciesRandom HNo ratings yet
- Summary - Regional Action Plan For Refugee and Migrant Health 2023 2030enDocument2 pagesSummary - Regional Action Plan For Refugee and Migrant Health 2023 2030enepure.mirunaNo ratings yet
- Primary Health Care Workers ManualDocument11 pagesPrimary Health Care Workers ManualVanitha duraiNo ratings yet
- Abstract 59Document3 pagesAbstract 59Jarvis WheelerNo ratings yet
- Draft Ast 3Document21 pagesDraft Ast 3Nathan ChanhangaNo ratings yet
- Influences Impacting The Acceptance of Voluntary Medical Male Circumcision Among Medical Students Pursuing Bachelor's Degrees at Kampala International University Teaching HospitalDocument10 pagesInfluences Impacting The Acceptance of Voluntary Medical Male Circumcision Among Medical Students Pursuing Bachelor's Degrees at Kampala International University Teaching HospitalKIU PUBLICATION AND EXTENSIONNo ratings yet
- Global Output of Research On The Health of International Migrant Workers From 2000 To 2017Document12 pagesGlobal Output of Research On The Health of International Migrant Workers From 2000 To 2017Meghraj ChinchoreNo ratings yet
- Travel Health Nursing: Scope and Standards of Practice, 1st EditionFrom EverandTravel Health Nursing: Scope and Standards of Practice, 1st EditionNo ratings yet
- Clinical Protection Handbook: for Healthcare Workers against COVID-19From EverandClinical Protection Handbook: for Healthcare Workers against COVID-19No ratings yet
- Community Mobilization As An Essential ToolDocument67 pagesCommunity Mobilization As An Essential ToolUsman Ahmad TijjaniNo ratings yet
- Attitude 0F Nursing Mothers Towards Exclusive Breast Feeding Among Maried Women Aged 18-45 YearsDocument47 pagesAttitude 0F Nursing Mothers Towards Exclusive Breast Feeding Among Maried Women Aged 18-45 YearsUsman Ahmad TijjaniNo ratings yet
- Effects of Vitamin A Deficiency in Primary School PupilsDocument55 pagesEffects of Vitamin A Deficiency in Primary School PupilsUsman Ahmad TijjaniNo ratings yet
- Appraising The Attitude of People Towards The Use of Family Planning ServicesDocument59 pagesAppraising The Attitude of People Towards The Use of Family Planning ServicesUsman Ahmad TijjaniNo ratings yet
- Assesment of Remediation Toward The Eredication of Lead PoisonDocument51 pagesAssesment of Remediation Toward The Eredication of Lead PoisonUsman Ahmad TijjaniNo ratings yet
- Assessment of Nutritional Status of Pregnant Women AttendingDocument60 pagesAssessment of Nutritional Status of Pregnant Women AttendingUsman Ahmad Tijjani100% (1)
- Assessment of The Factors Affecting The Nutritional Status of Pregnant Women AttendingDocument73 pagesAssessment of The Factors Affecting The Nutritional Status of Pregnant Women AttendingUsman Ahmad TijjaniNo ratings yet
- Eng MetodbokenDocument130 pagesEng MetodbokenUsman Ahmad TijjaniNo ratings yet
- Analysis of The Factors Responsible For Water Pollution inDocument57 pagesAnalysis of The Factors Responsible For Water Pollution inUsman Ahmad TijjaniNo ratings yet
- Senate of The Federal Republic of Nigeria Order Paper: Tuesday, 9 February, 2021Document6 pagesSenate of The Federal Republic of Nigeria Order Paper: Tuesday, 9 February, 2021Usman Ahmad TijjaniNo ratings yet
- An Assessment of The Effects of Female Genital Mutilation AmongDocument57 pagesAn Assessment of The Effects of Female Genital Mutilation AmongUsman Ahmad TijjaniNo ratings yet
- Analysis of The Factors Responsible For Water Pollution in Rural CommunitiesDocument57 pagesAnalysis of The Factors Responsible For Water Pollution in Rural CommunitiesUsman Ahmad TijjaniNo ratings yet
- Knowledge, Attitude and Practice of Pilgrims Regarding Heat-Related Illnesses During The 2017 Hajj Mass GatheringDocument13 pagesKnowledge, Attitude and Practice of Pilgrims Regarding Heat-Related Illnesses During The 2017 Hajj Mass GatheringUsman Ahmad TijjaniNo ratings yet
- Utilization of Family Planning ProjectDocument49 pagesUtilization of Family Planning ProjectUsman Ahmad TijjaniNo ratings yet
- Investigating The Prevalence of Faeco - Oral Nematodes Infections Among ChildrenDocument59 pagesInvestigating The Prevalence of Faeco - Oral Nematodes Infections Among ChildrenUsman Ahmad TijjaniNo ratings yet
- The Significance of Immunization in The Prevention of Childhood Killer DiseasesDocument69 pagesThe Significance of Immunization in The Prevention of Childhood Killer DiseasesUsman Ahmad Tijjani100% (1)
- Evaluation of A Questionnaire To Assess Nutritional Knowledge, Attitudes and Practices in A Thai PopulationDocument10 pagesEvaluation of A Questionnaire To Assess Nutritional Knowledge, Attitudes and Practices in A Thai PopulationUsman Ahmad TijjaniNo ratings yet
- The Prevalence of Diabetes Mellitus Among Fifty Years and AboveDocument58 pagesThe Prevalence of Diabetes Mellitus Among Fifty Years and AboveUsman Ahmad TijjaniNo ratings yet
- Sexuality and Contractive Use Among AdolescentsDocument35 pagesSexuality and Contractive Use Among AdolescentsUsman Ahmad TijjaniNo ratings yet
- 3rd Page 5Document1 page3rd Page 5api-282737728No ratings yet
- Contoh Assignment PDFDocument18 pagesContoh Assignment PDFSiti Fatimah A Salam67% (3)
- TMPRO CASABE 1318 Ecopetrol Full ReportDocument55 pagesTMPRO CASABE 1318 Ecopetrol Full ReportDiego CastilloNo ratings yet
- Business CombinationsDocument18 pagesBusiness Combinationszubair afzalNo ratings yet
- Karthik ResumeDocument2 pagesKarthik ResumeArun Raj ANo ratings yet
- LS01 ServiceDocument53 pagesLS01 ServicehutandreiNo ratings yet
- Bachelors - Harvest Moon Animal ParadeDocument12 pagesBachelors - Harvest Moon Animal ParaderikaNo ratings yet
- Teks Drama Malin KundangDocument8 pagesTeks Drama Malin KundangUhuy ManiaNo ratings yet
- PreviewpdfDocument83 pagesPreviewpdfJohana GavilanesNo ratings yet
- Object-Oriented Design Patterns in The Kernel, Part 2 (LWN - Net)Document15 pagesObject-Oriented Design Patterns in The Kernel, Part 2 (LWN - Net)Rishabh MalikNo ratings yet
- Rubric For Aet570 BenchmarkDocument4 pagesRubric For Aet570 Benchmarkapi-255765082No ratings yet
- Buildingawinningsalesforce WP DdiDocument14 pagesBuildingawinningsalesforce WP DdiMawaheb ContractingNo ratings yet
- Lec. 2Document22 pagesLec. 2محمدNo ratings yet
- Journal of Atmospheric Science Research - Vol.5, Iss.4 October 2022Document54 pagesJournal of Atmospheric Science Research - Vol.5, Iss.4 October 2022Bilingual PublishingNo ratings yet
- Jurnal Ekologi TerestrialDocument6 pagesJurnal Ekologi TerestrialFARIS VERLIANSYAHNo ratings yet
- Manual Ares-G2 2Document78 pagesManual Ares-G2 2CarolDiasNo ratings yet
- Will Smith BiographyDocument11 pagesWill Smith Biographyjhonatan100% (1)
- Distribution BoardDocument7 pagesDistribution BoardmuralichandrasekarNo ratings yet
- AFAR - 07 - New Version No AnswerDocument7 pagesAFAR - 07 - New Version No AnswerjonasNo ratings yet
- Asuhan Keperawatan Pada Klien Dengan Proses Penyembuhan Luka. Pengkajian Diagnosa Perencanaan Implementasi EvaluasiDocument43 pagesAsuhan Keperawatan Pada Klien Dengan Proses Penyembuhan Luka. Pengkajian Diagnosa Perencanaan Implementasi EvaluasiCak FirmanNo ratings yet
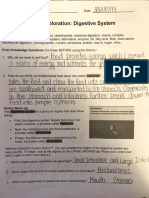
- Student Exploration: Digestive System: Food Inio Simple Nutrien/oDocument9 pagesStudent Exploration: Digestive System: Food Inio Simple Nutrien/oAshantiNo ratings yet
- Engine Controls (Powertrain Management) - ALLDATA RepairDocument3 pagesEngine Controls (Powertrain Management) - ALLDATA RepairRonald FerminNo ratings yet
- Britannia Volume 12 Issue 1981 (Doi 10.2307/526240) Michael P. Speidel - Princeps As A Title For 'Ad Hoc' CommandersDocument8 pagesBritannia Volume 12 Issue 1981 (Doi 10.2307/526240) Michael P. Speidel - Princeps As A Title For 'Ad Hoc' CommandersSteftyraNo ratings yet
- 1"a Study On Employee Retention in Amara Raja Power Systems LTDDocument81 pages1"a Study On Employee Retention in Amara Raja Power Systems LTDJerome Samuel100% (1)
- Clash of Clans Hack Activation CodeDocument2 pagesClash of Clans Hack Activation Codegrumpysadness7626No ratings yet
- NHM Thane Recruitment 2022 For 280 PostsDocument9 pagesNHM Thane Recruitment 2022 For 280 PostsDr.kailas Gaikwad , MO UPHC Turbhe NMMCNo ratings yet