You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Metabical Case Study SolutionDocument4 pagesMetabical Case Study Solutionparoengineer100% (7)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 023-SOP For Conducting Hold Time StudyDocument3 pages023-SOP For Conducting Hold Time StudyAshok Lenka100% (2)
- Drugs Acting On GitDocument119 pagesDrugs Acting On GitNathaniel Mbiu Tim100% (1)
- 2017-06 NewsletterDocument5 pages2017-06 Newsletterapi-235801784No ratings yet
- Anti Scabies DrugsDocument4 pagesAnti Scabies DrugsNavjot Brar100% (2)
- NCP PneumoniaDocument47 pagesNCP Pneumoniabhevpat251100% (1)
- Nama Antibiotik Regimen Dosis Dosis Per-Hari Rute No Kode PasienDocument10 pagesNama Antibiotik Regimen Dosis Dosis Per-Hari Rute No Kode PasienAri AnggaraNo ratings yet
- Clinical PharmacyDocument38 pagesClinical PharmacyJurusan Farmasi Poltekkes MedanNo ratings yet
- At Home Steroid Testing GuideDocument11 pagesAt Home Steroid Testing GuideMyHomeTestingNo ratings yet
- USFDA Guidelines For PharmaceuticalsDocument5 pagesUSFDA Guidelines For PharmaceuticalsemranNo ratings yet
- Xenobiotic Metabolism PDFDocument50 pagesXenobiotic Metabolism PDFroxy8marie8chanNo ratings yet
- B Pharm 8 Sem Pharmalite - inDocument30 pagesB Pharm 8 Sem Pharmalite - inAnurag PatelNo ratings yet
- General PHARMAKOLOGY - Загальна фармакологія - Курс лекцій - изд.2005-215 сDocument219 pagesGeneral PHARMAKOLOGY - Загальна фармакологія - Курс лекцій - изд.2005-215 сSahil Saini100% (4)
- Olive Oil PEG-7 EstersDocument29 pagesOlive Oil PEG-7 EstersNurulNo ratings yet
- Syn 3 - Roche and Tamiflu-SG3Document29 pagesSyn 3 - Roche and Tamiflu-SG3Yani RahmaNo ratings yet
- Aripiprazole Lai Prescribing GuidelinesDocument8 pagesAripiprazole Lai Prescribing Guidelinestabic68932No ratings yet
- Common Drugs and Their Antidotes - PDF Version 1Document4 pagesCommon Drugs and Their Antidotes - PDF Version 1Maryam Khushbakhat50% (2)
- ChemDocument13 pagesChemKrislyn Joy FloresNo ratings yet
- 2 PirrolidonaDocument4 pages2 PirrolidonaAstrid Carolina Gutierrez ShimabukuroNo ratings yet
- Morocco Pharmaceuticals ReportDocument45 pagesMorocco Pharmaceuticals ReportGone Fishin100% (2)
- Drug and Alcohol Policy CAN enDocument43 pagesDrug and Alcohol Policy CAN enrv0014No ratings yet
- 1.2 Drug Devt and ProcessDocument14 pages1.2 Drug Devt and ProcessJohn King AmuraoNo ratings yet
- Research Paper About Herbal PlantsDocument8 pagesResearch Paper About Herbal Plantssvfziasif100% (1)
- Drug StudyDocument14 pagesDrug StudyNikki RodrigoNo ratings yet
- Stock Obat BPJS Desember 2017Document16 pagesStock Obat BPJS Desember 2017Vika FujiNo ratings yet
- Potassium Chloride - Uses, Dosage & Side EffectsDocument4 pagesPotassium Chloride - Uses, Dosage & Side EffectsKenneth Mark B. TevesNo ratings yet
- Chapter 11 Multiple Dosage RegimenDocument35 pagesChapter 11 Multiple Dosage RegimenYuli Irvaransiah DIatun NIkmah100% (2)
- Auto ClaveDocument4 pagesAuto ClaveSarah Swasti PNo ratings yet
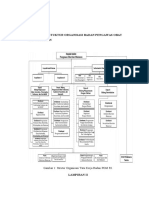
- Lampiran 1: Stuktur Organisasi Badan Pengawas Obat Dan MakananDocument13 pagesLampiran 1: Stuktur Organisasi Badan Pengawas Obat Dan MakananmeilaNo ratings yet
- Ketoconazole Cream Clinical ParticularsDocument2 pagesKetoconazole Cream Clinical ParticularsJai MurugeshNo ratings yet