You might also like
- Diabetes and ExerciseDocument5 pagesDiabetes and ExerciseRoslitha HaryaniNo ratings yet
- Diabetes Up Date 2009Document115 pagesDiabetes Up Date 2009Stefani NoviliaNo ratings yet
- Type 2 Diabetes MellitusDocument24 pagesType 2 Diabetes Mellitusdr. M.F. Romdhoni100% (1)
- Pharmacotherapeutics PDFDocument30 pagesPharmacotherapeutics PDFprazol shresthaNo ratings yet
- 34 - Polyneuropathy Classification by NCS and EMGDocument16 pages34 - Polyneuropathy Classification by NCS and EMGMutiara Kristiani PutriNo ratings yet
- Curs Diabet 1-3Document202 pagesCurs Diabet 1-3serj_inaNo ratings yet
- Risk For Unstable Blood Glucose (DM)Document4 pagesRisk For Unstable Blood Glucose (DM)Ace Khiel Peralta50% (2)
- Medsurg 1Document59 pagesMedsurg 1Angel YN Patricio FlorentinoNo ratings yet
- Insulin Dr. BowoDocument39 pagesInsulin Dr. BowoAri AsriniNo ratings yet
- DM Tipe 1 Neuropati DiabetikDocument15 pagesDM Tipe 1 Neuropati DiabetikMutiara Kristiani PutriNo ratings yet
- Edr 05 155Document8 pagesEdr 05 155Noor NoorNo ratings yet
- Diabeticneuropathypart1: Overview and Symmetric PhenotypesDocument21 pagesDiabeticneuropathypart1: Overview and Symmetric PhenotypesPrima Heptayana NainggolanNo ratings yet
- Kaur, Diabetic Autonomic Neuropathy Pathogenesis and Treatment, 2014Document8 pagesKaur, Diabetic Autonomic Neuropathy Pathogenesis and Treatment, 2014elbueno21No ratings yet
- 2023 Pharmacogenomics Diabetes FAA - 240118 - 071252Document24 pages2023 Pharmacogenomics Diabetes FAA - 240118 - 071252Maryam HaniniNo ratings yet
- Guidelines Neuropaty DMDocument8 pagesGuidelines Neuropaty DMPinto D. R PiliangNo ratings yet
- Redox-Potential and Immune-Endothelial Axis States of Pancreases in Type 2 Diabetes Mellitus in ExperimentsDocument6 pagesRedox-Potential and Immune-Endothelial Axis States of Pancreases in Type 2 Diabetes Mellitus in ExperimentsEdisher TsivtsivadzeNo ratings yet
- Journal ReadingDocument7 pagesJournal Readingdr AnnisaNo ratings yet
- Experimental Biology and MedicineDocument11 pagesExperimental Biology and MedicineYunitasya GuspiraNo ratings yet
- Accepted Manuscript: Diabetes & Metabolic Syndrome: Clinical Research & ReviewsDocument14 pagesAccepted Manuscript: Diabetes & Metabolic Syndrome: Clinical Research & ReviewsRafaelPetitNo ratings yet
- Diabetes - Lecture: Prof. Dr. Doina CatrinoiuDocument131 pagesDiabetes - Lecture: Prof. Dr. Doina CatrinoiuPantea Constantin AlinNo ratings yet
- Resveratrol NeuropathyDocument13 pagesResveratrol NeuropathyΔημητρης ΦιλιογλουNo ratings yet
- 4984 23623 1 PB PDFDocument14 pages4984 23623 1 PB PDFMayra Elizabeth RodriguezNo ratings yet
- Patofisiologi Diabetic NefropathyDocument5 pagesPatofisiologi Diabetic NefropathyFakhri AminNo ratings yet
- Ep171984 CRDocument3 pagesEp171984 CRAssifa RidzkiNo ratings yet
- Pharmacological Management of Type 2 Diabetes Mellitus: Rationale For Rational Use of InsulinDocument9 pagesPharmacological Management of Type 2 Diabetes Mellitus: Rationale For Rational Use of InsulinAditya Rachman Van Der ArjunaqueeNo ratings yet
- Prediction of Type 2 Diabetes: A Natural History PerspectiveDocument9 pagesPrediction of Type 2 Diabetes: A Natural History Perspectiveandree_zz4890No ratings yet
- Management of Type 2 Diabetes and Its ChallengesDocument81 pagesManagement of Type 2 Diabetes and Its ChallengesKay BristolNo ratings yet
- Diabetes ComplicationsDocument23 pagesDiabetes ComplicationsSelin SakarNo ratings yet
- 1 Octeto de DefronzoDocument23 pages1 Octeto de DefronzoLesli Rodriguez50% (2)
- Yamabe 2009Document8 pagesYamabe 2009Burcuș AlexandruNo ratings yet
- Autonomic NeuropathyDocument20 pagesAutonomic NeuropathyRegina CaeciliaNo ratings yet
- Trerapi Insulin Siip 2Document10 pagesTrerapi Insulin Siip 2Indra YudaNo ratings yet
- 979 7003 2 PBDocument8 pages979 7003 2 PBJesús Torres MayaNo ratings yet
- Empagliflozin Related To Ketoacidosis and Early Neurological Deterioration in A Patient With Acute Ischemic StrokeDocument9 pagesEmpagliflozin Related To Ketoacidosis and Early Neurological Deterioration in A Patient With Acute Ischemic Stroke王湘淇No ratings yet
- Drug Therapy Prevention and Treatment DiabetesDocument8 pagesDrug Therapy Prevention and Treatment DiabetesBaba diawNo ratings yet
- Modul Diabetes Bersama (5-9)Document13 pagesModul Diabetes Bersama (5-9)Lazuardi FadhullahNo ratings yet
- Dysregulation of Fatty Acid Metabolism in The Etiology of Type 2 DiabetesDocument12 pagesDysregulation of Fatty Acid Metabolism in The Etiology of Type 2 DiabetesanjumNo ratings yet
- Early Urinary Markers of Diabetic Kidney Disease: A Nested Case-Control Study From The Diabetes Control and Complications Trial (DCCT)Document11 pagesEarly Urinary Markers of Diabetic Kidney Disease: A Nested Case-Control Study From The Diabetes Control and Complications Trial (DCCT)Felipe SangiovanniNo ratings yet
- Oxidative Stress, ER Stress, and The JNK Pathway in Type 2 DiabetesDocument11 pagesOxidative Stress, ER Stress, and The JNK Pathway in Type 2 DiabetesLitaDwiNo ratings yet
- Metabolic Changes in Diabetes: R. D. G. Leslie LondonDocument4 pagesMetabolic Changes in Diabetes: R. D. G. Leslie LondonManuNo ratings yet
- NSAID Nephropathy and COX-2 Inhibitors: Kellie A Goldsborough, MD Resident Grand Rounds November 2, 1999Document49 pagesNSAID Nephropathy and COX-2 Inhibitors: Kellie A Goldsborough, MD Resident Grand Rounds November 2, 1999Galon AirnyaNo ratings yet
- CrimesDocument6 pagesCrimesShirmayne TangNo ratings yet
- Rutin NeuropathyDocument9 pagesRutin NeuropathyΔημητρης ΦιλιογλουNo ratings yet
- Diabetes Melitus Jurnal Remed BiomedDocument6 pagesDiabetes Melitus Jurnal Remed BiomedNur Roza Aulia RNo ratings yet
- 28sici 291096 9136 28199802 2915 3A2 3C97 3A 3aaid Dia523 3e3.0.co 3B2 5 PDFDocument16 pages28sici 291096 9136 28199802 2915 3A2 3C97 3A 3aaid Dia523 3e3.0.co 3B2 5 PDFHesbon MomanyiNo ratings yet
- Kalra 2011Document7 pagesKalra 2011jinsung parkNo ratings yet
- NIH Public Access: Diabetic Neuropathy: One Disease or Two?Document10 pagesNIH Public Access: Diabetic Neuropathy: One Disease or Two?AgunkRestuMaulanaNo ratings yet
- GLP1 Renal 1Document11 pagesGLP1 Renal 1miguelcontreraszambranoNo ratings yet
- Spontaneous Akt2 Deficiency in A Colony of NOD Mice Exhibiting Early DiabetesDocument9 pagesSpontaneous Akt2 Deficiency in A Colony of NOD Mice Exhibiting Early DiabetesNormanNo ratings yet
- Serum C-Peptide Concentrations Poorly Phenotype Type 2 Diabetic End-Stage Renal Disease PatientsDocument9 pagesSerum C-Peptide Concentrations Poorly Phenotype Type 2 Diabetic End-Stage Renal Disease PatientsekaNo ratings yet
- Diabetes MellitusDocument18 pagesDiabetes MellitusAadhan ArveeNo ratings yet
- Mod 9 DMDocument3 pagesMod 9 DMRoxanne Nasingao100% (1)
- Penatalaksanaan Tindakan Kedokteran Gigi Pada Pasien Diabetes MellitusDocument35 pagesPenatalaksanaan Tindakan Kedokteran Gigi Pada Pasien Diabetes MellitusgeneNo ratings yet
- New Insights Into The Pathophysiology of Diabetic Nephropathy: From Haemodynamics To Molecular PathologyDocument12 pagesNew Insights Into The Pathophysiology of Diabetic Nephropathy: From Haemodynamics To Molecular PathologyleidoskyNo ratings yet
- Zanoglide Updated Master Slide Deck - Eva MOBILE VERSIONDocument124 pagesZanoglide Updated Master Slide Deck - Eva MOBILE VERSIONMaha BondokNo ratings yet
- Definition of Diabetes Mellitus (DM)Document12 pagesDefinition of Diabetes Mellitus (DM)Romarc Owen CorpuzNo ratings yet
- Glycemic EmergenciesDocument10 pagesGlycemic EmergenciesLily Anggraeni PrayogoNo ratings yet
- Curs Studenti StrainiDocument71 pagesCurs Studenti StrainiAlexandru VisanNo ratings yet
- Diabetes: Activity Levels As Countries Become More Industrialized, and The Aging of The PopulationDocument9 pagesDiabetes: Activity Levels As Countries Become More Industrialized, and The Aging of The PopulationLouije MombzNo ratings yet
- Livro Robbins PathologyDocument18 pagesLivro Robbins Pathologyernestooliveira50% (2)
- Diabetes Mellitus (DM)Document59 pagesDiabetes Mellitus (DM)Crome operatorNo ratings yet
- Hipoglicemiadm2 2004Document8 pagesHipoglicemiadm2 2004Victor Bazan AlvarezNo ratings yet
- SoalDocument8 pagesSoalMutiara Kristiani PutriNo ratings yet
- Dominance: Autosomal RecessiveDocument6 pagesDominance: Autosomal RecessiveMutiara Kristiani PutriNo ratings yet
- Mendeley CiteDocument1 pageMendeley CiteMutiara Kristiani PutriNo ratings yet
- Itinerary 4: 8/10/2 022: Jakarta - BarcelonaDocument4 pagesItinerary 4: 8/10/2 022: Jakarta - BarcelonaMutiara Kristiani PutriNo ratings yet
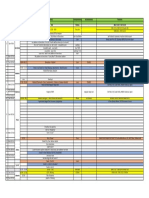
- Day Date City Activities Transportations Accomodation Remarks Malang 11.20-12.45 MLG - CGK Citilink - MLG 11.20 - CGK 12.45 Jakarta 17.55 - 13.25Document1 pageDay Date City Activities Transportations Accomodation Remarks Malang 11.20-12.45 MLG - CGK Citilink - MLG 11.20 - CGK 12.45 Jakarta 17.55 - 13.25Mutiara Kristiani PutriNo ratings yet
- ItineraryDocument155 pagesItineraryMutiara Kristiani PutriNo ratings yet
- Day Date City Activities Transportations Accomodation Remarks Malang 11.20-12.45 MLG - CGK Citilink - MLG 11.20 - CGK 12.45 Jakarta 17.55 - 13.25Document1 pageDay Date City Activities Transportations Accomodation Remarks Malang 11.20-12.45 MLG - CGK Citilink - MLG 11.20 - CGK 12.45 Jakarta 17.55 - 13.25Mutiara Kristiani PutriNo ratings yet
- Research Article Electrophysiological Characterization of Neuropathy Complicating Type 1 Diabetes MellitusDocument7 pagesResearch Article Electrophysiological Characterization of Neuropathy Complicating Type 1 Diabetes MellitusMutiara Kristiani PutriNo ratings yet
- Learning Through PlayDocument8 pagesLearning Through PlayMutiara Kristiani PutriNo ratings yet
- Ir. Gaguk Sukowiyono, MTDocument2 pagesIr. Gaguk Sukowiyono, MTMutiara Kristiani PutriNo ratings yet
- Icd 10 LengkapDocument4 pagesIcd 10 LengkapMutiara Kristiani PutriNo ratings yet
- Icd 9Cm Roo (Tindakan) : Mra, Myy, Gre, Ran, Rof, CadDocument7 pagesIcd 9Cm Roo (Tindakan) : Mra, Myy, Gre, Ran, Rof, CadMutiara Kristiani PutriNo ratings yet
- PAAO2023: Rules & RegulationsDocument4 pagesPAAO2023: Rules & RegulationsMutiara Kristiani PutriNo ratings yet
- Daftar PPDS Accepted Euretina Dan Wspos 2020Document3 pagesDaftar PPDS Accepted Euretina Dan Wspos 2020Mutiara Kristiani PutriNo ratings yet
- Konduksi DSP NcsDocument7 pagesKonduksi DSP NcsMutiara Kristiani PutriNo ratings yet
- Distal Symmetric PolyneuropathyDocument40 pagesDistal Symmetric PolyneuropathyMutiara Kristiani PutriNo ratings yet
- Distal Symmetric PolyneuropathyDocument40 pagesDistal Symmetric PolyneuropathyMutiara Kristiani PutriNo ratings yet
- Research Article Electrophysiological Characterization of Neuropathy Complicating Type 1 Diabetes MellitusDocument7 pagesResearch Article Electrophysiological Characterization of Neuropathy Complicating Type 1 Diabetes MellitusMutiara Kristiani PutriNo ratings yet
- SOALDocument3 pagesSOALMutiara Kristiani PutriNo ratings yet
- Konduksi DSP NcsDocument7 pagesKonduksi DSP NcsMutiara Kristiani PutriNo ratings yet
- 34 - Polyneuropathy Classification by NCS and EMGDocument16 pages34 - Polyneuropathy Classification by NCS and EMGMuhammad Imran MirzaNo ratings yet
- American Academy of Opthalmology, Glaucoma, in Basic and Clinical Science Course, Section 10, 2018-2019, p17-29Document1 pageAmerican Academy of Opthalmology, Glaucoma, in Basic and Clinical Science Course, Section 10, 2018-2019, p17-29Mutiara Kristiani PutriNo ratings yet
- Preterm Premature Rupture of Membranes (PPROM) - Assessment and Management GuidelineDocument6 pagesPreterm Premature Rupture of Membranes (PPROM) - Assessment and Management GuidelineAlexis LambertNo ratings yet
- Repetitio Est Mater StudiorumDocument1 pageRepetitio Est Mater StudiorumMutiara Kristiani PutriNo ratings yet
- Soal Uji KompetensiDocument33 pagesSoal Uji KompetensiMutiara Kristiani PutriNo ratings yet
- DapusDocument1 pageDapusMutiara Kristiani PutriNo ratings yet
- DapusDocument1 pageDapusMutiara Kristiani PutriNo ratings yet
- DM Tipe 1Document6 pagesDM Tipe 1Mutiara Kristiani PutriNo ratings yet
- Chapter 50 51 Prelec Quizzes Case Studies Discussion Topis and Critical Thinking Exercises Work To Be Done..Document8 pagesChapter 50 51 Prelec Quizzes Case Studies Discussion Topis and Critical Thinking Exercises Work To Be Done..Besael BaccolNo ratings yet
- Diabetes and COVID-19: Risks, Management, and Learnings From Other National DisastersDocument9 pagesDiabetes and COVID-19: Risks, Management, and Learnings From Other National DisastersRahmanu ReztaputraNo ratings yet
- Practice Test 6: Your AnswersDocument11 pagesPractice Test 6: Your AnswersTran Phuong LinhNo ratings yet
- NCLEX Practice Test For Endocrine Disorders Part 2Document16 pagesNCLEX Practice Test For Endocrine Disorders Part 2Hasan A AsFourNo ratings yet
- ICMR GuidelinesType2diabetes2018 0Document82 pagesICMR GuidelinesType2diabetes2018 0VISHWANATH MARSHIVANIKARNo ratings yet
- Recalls 2 - Np3Document70 pagesRecalls 2 - Np3Kurt Nino TorresNo ratings yet
- Concours General 2005 KaderDocument5 pagesConcours General 2005 KaderDaouda ThiamNo ratings yet
- The Study of Knowledge, Attitude and Practice Among Diabetic Patients During Ramadan at Hospital Tengku Ampuan AfzanDocument10 pagesThe Study of Knowledge, Attitude and Practice Among Diabetic Patients During Ramadan at Hospital Tengku Ampuan AfzanIzzul HafiyNo ratings yet
- Animal ModelsDocument22 pagesAnimal ModelsM.anwar KhanNo ratings yet
- Exercise Management in Type 1 Diabetes A Consensus Mike Riddell Lancet DE 2017Document14 pagesExercise Management in Type 1 Diabetes A Consensus Mike Riddell Lancet DE 2017Arie AnggaNo ratings yet
- A. Gestational Diabetes Mellitus B. Secondary Diabetes Mellitus D. Type II Diabetes MellitusDocument32 pagesA. Gestational Diabetes Mellitus B. Secondary Diabetes Mellitus D. Type II Diabetes MellitusNebawNo ratings yet
- FERA Internal MedDocument63 pagesFERA Internal Medabdi haychoNo ratings yet
- WELVET701EN - GLUCO CALEA - FolderDocument20 pagesWELVET701EN - GLUCO CALEA - FolderandreisandorNo ratings yet
- (123doc) - De-Thi-Tieng-Anh-De-Test-15-KeyDocument12 pages(123doc) - De-Thi-Tieng-Anh-De-Test-15-KeyLâm Nguyễn hảiNo ratings yet
- Health Problems Most Common in School Aged ChildrenDocument15 pagesHealth Problems Most Common in School Aged ChildrenAsterlyn ConiendoNo ratings yet
- Treating Type 1 Diabetes (For Parents) - Print Version - Nemours KidsHealthDocument2 pagesTreating Type 1 Diabetes (For Parents) - Print Version - Nemours KidsHealthSally LeeNo ratings yet
- Final 1Document7 pagesFinal 1Murti GutoNo ratings yet
- Diagnosis and Management of Type 2 Diabetes Mellitus ©stephen D. Sisson MD/Ambulatory Curriculum 2021Document48 pagesDiagnosis and Management of Type 2 Diabetes Mellitus ©stephen D. Sisson MD/Ambulatory Curriculum 2021Carolina González RiveraNo ratings yet
- Group 1,2,4 QuizDocument221 pagesGroup 1,2,4 QuizPaulNo ratings yet
- Heart Disease Prediction Final ReportDocument31 pagesHeart Disease Prediction Final ReportMUSIC BY LOSTNo ratings yet
- Study Case-Hormones of Adrenal CortexDocument54 pagesStudy Case-Hormones of Adrenal CortexantonNo ratings yet
- Diet Analysis EssayDocument3 pagesDiet Analysis Essayezkep38r100% (2)
- Endo Pancrease ElhDocument27 pagesEndo Pancrease Elhodiodi57No ratings yet
- GP Kaunseling 2019 Isbn FinalDocument90 pagesGP Kaunseling 2019 Isbn FinalAtiqah RamzanNo ratings yet
- Mamma Mia!: Read The Text and Choose The Right AnswerDocument6 pagesMamma Mia!: Read The Text and Choose The Right AnswerJeroen BerxNo ratings yet
- Soliqua 100/33 (Insulin Glargine Plus Lixisenatide) Receives FDA Approval For Adults With Type 2 DiabetesDocument4 pagesSoliqua 100/33 (Insulin Glargine Plus Lixisenatide) Receives FDA Approval For Adults With Type 2 DiabetesBernadet MariaNo ratings yet
- RPN Integrated Test VIDocument27 pagesRPN Integrated Test VIMikaNo ratings yet