You might also like
- Brain ventricles: cavities within the brainDocument23 pagesBrain ventricles: cavities within the brainAndrei Scripcaru100% (1)
- The Ventricular SystemDocument6 pagesThe Ventricular SystemM Arsalan TariqNo ratings yet
- Dura Mater & Cranial SinusDocument30 pagesDura Mater & Cranial SinusSadiq Wadood SiddiquiNo ratings yet
- Dura Mater & Cranial SinusDocument30 pagesDura Mater & Cranial SinusSadiq Wadood Siddiqui100% (1)
- Ventricles of BrainDocument30 pagesVentricles of BrainbegeerizikNo ratings yet
- Neuroanatomy 11: Brain Ventricles: The Anterior HornDocument3 pagesNeuroanatomy 11: Brain Ventricles: The Anterior HornstuffNo ratings yet
- Ventricular System and Cerebrospinal Fluid ProductionDocument35 pagesVentricular System and Cerebrospinal Fluid Productionfarzana25No ratings yet
- The Fourth VentricleDocument16 pagesThe Fourth VentricleHiraNo ratings yet
- Ventricles Sub ArachnoidspaceDocument41 pagesVentricles Sub ArachnoidspaceShivaranjani sakthivelNo ratings yet
- Cerebraal Spinal FluidDocument34 pagesCerebraal Spinal FluidElisa NNo ratings yet
- The Ventricular System & The Cerebrospinal Fluid (Physiotherapy)Document40 pagesThe Ventricular System & The Cerebrospinal Fluid (Physiotherapy)Richmond tohNo ratings yet
- Dural Venous Sinuses and Their FunctionsDocument49 pagesDural Venous Sinuses and Their FunctionsEastma MeiliNo ratings yet
- Scalp: Dr. ManuniDocument18 pagesScalp: Dr. ManuniVinus VaghelaNo ratings yet
- Embryology SlideDocument33 pagesEmbryology Slidethorodison786No ratings yet
- Brain Dura Mater AnatomyDocument25 pagesBrain Dura Mater AnatomyVinus VaghelaNo ratings yet
- Development of Nervous System by Dr Hemant JoshiDocument25 pagesDevelopment of Nervous System by Dr Hemant JoshiHemant JoshiNo ratings yet
- Nasal Cavity Anatomy and Paranasal SinusesDocument39 pagesNasal Cavity Anatomy and Paranasal SinusesJuan Guillermo Leiva BenavidesNo ratings yet
- Meninges وهدانDocument10 pagesMeninges وهدانوسيم جمال مياسNo ratings yet
- Introduction to the Cranial Cavity and its StructuresDocument35 pagesIntroduction to the Cranial Cavity and its StructuresexoNo ratings yet
- Meninges: Dr. Katharina Kian R. Demerre - BacolodDocument78 pagesMeninges: Dr. Katharina Kian R. Demerre - BacolodCyril Jay G. OrtegaNo ratings yet
- Ventricles of the Brain and CSF CirculationDocument14 pagesVentricles of the Brain and CSF Circulationmhr27112002No ratings yet
- Cerebrospinal FluidDocument154 pagesCerebrospinal Fluidabhirox69100% (1)
- Blood Supply of The Brain - ModifiedDocument24 pagesBlood Supply of The Brain - ModifiedSamo BeainoNo ratings yet
- Dural Venous SinusDocument38 pagesDural Venous SinusChipego NyirendaNo ratings yet
- Spinal CordDocument31 pagesSpinal CordMercy DakaNo ratings yet
- The Brain's Blood SupplyDocument41 pagesThe Brain's Blood SupplyRtvc RoldanNo ratings yet
- Lateral Ventricles: The Ventricular System of The Human BrainDocument4 pagesLateral Ventricles: The Ventricular System of The Human BrainMarNo ratings yet
- Gambaran MeningesDocument39 pagesGambaran MeningesPurnomo Ponco Nugroho100% (1)
- External Carotic Artery LigationDocument67 pagesExternal Carotic Artery LigationErnesto Fer FdezNo ratings yet
- MENINGES - Anatomy of Dura Matter, Pia MatterDocument34 pagesMENINGES - Anatomy of Dura Matter, Pia MatterfidhavfathimaNo ratings yet
- Anatomy - Anterior Triangle of The Neck PDFDocument6 pagesAnatomy - Anterior Triangle of The Neck PDFAngel KimNo ratings yet
- The Midbrain and Important ConnectionsDocument118 pagesThe Midbrain and Important ConnectionsBaguma MichaelNo ratings yet
- Anatomy of Meninges Ventricles CerebrospinalfluidDocument120 pagesAnatomy of Meninges Ventricles CerebrospinalfluidSasikala MohanNo ratings yet
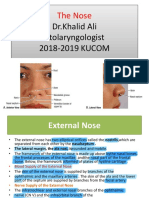
- The Nose 2Document27 pagesThe Nose 2Ahmed JawdetNo ratings yet
- Brain Ventricles: (Rabbia Yousaf) Pharm-D Rashid Latif College of PharmacyDocument29 pagesBrain Ventricles: (Rabbia Yousaf) Pharm-D Rashid Latif College of PharmacyShafaqat Ghani Shafaqat GhaniNo ratings yet
- Lecture FiveDocument35 pagesLecture FivePiniel MatewosNo ratings yet
- Venous Supply of Head, Neck and FaceDocument67 pagesVenous Supply of Head, Neck and FaceAlisha AranhaNo ratings yet
- Chick Embryo ReviewerDocument9 pagesChick Embryo ReviewerKeana TapangNo ratings yet
- Brainstem Anatomy and FeaturesDocument12 pagesBrainstem Anatomy and FeatureslindaNo ratings yet
- Development of Midbrain and HindbrainDocument58 pagesDevelopment of Midbrain and HindbrainBramwell K. MiteiNo ratings yet
- 2-Meninges and SinusesDocument62 pages2-Meninges and SinusesMajd HallakNo ratings yet
- L1 Cerebrovascular Anatomy and Nerves of Lower LimbDocument48 pagesL1 Cerebrovascular Anatomy and Nerves of Lower LimbAshraf NabilNo ratings yet
- Meninges PPT NPDocument21 pagesMeninges PPT NPEmshellr RomeNo ratings yet
- BrainDocument33 pagesBrainGeoffreyNo ratings yet
- Neuro AnatomyDocument191 pagesNeuro Anatomysirima makuraNo ratings yet
- Anatomy of CVS: 4. Blood Vessels of The Head & NeckDocument37 pagesAnatomy of CVS: 4. Blood Vessels of The Head & Necksultan khabeebNo ratings yet
- Blood Supply of The Head NeckDocument21 pagesBlood Supply of The Head NeckShadowStormNo ratings yet
- ENDOCRINE and FEMALE Genital SystemsDocument9 pagesENDOCRINE and FEMALE Genital SystemsIshraq AfifiNo ratings yet
- Spinal CordDocument60 pagesSpinal CordPiyush KumarNo ratings yet
- NaaaaaaaaaaaDocument64 pagesNaaaaaaaaaaaRhea RaveloNo ratings yet
- Ventricular System and Cerebrospinal Fluid: Structure and Clinical CorrelationsDocument22 pagesVentricular System and Cerebrospinal Fluid: Structure and Clinical CorrelationssamiratumananNo ratings yet
- Inner Ear Vestibular SystemDocument44 pagesInner Ear Vestibular Systemdharmendra kirarNo ratings yet
- Cranial Fossae: Zara Denisse Garcia Ella Carmela Chavez Mae Nen Vedeja Mardred MarceloDocument40 pagesCranial Fossae: Zara Denisse Garcia Ella Carmela Chavez Mae Nen Vedeja Mardred MarceloZara Sebastianne GarciaNo ratings yet
- Anatomy Thorax ReviewDocument18 pagesAnatomy Thorax Reviewyachiru121No ratings yet
- Cranial foramina and structures passing throughDocument13 pagesCranial foramina and structures passing throughAndra BauerNo ratings yet
- Blood Supply of BrainDocument29 pagesBlood Supply of BrainbegeerizikNo ratings yet
- Cardiovascular System DevelopmentDocument63 pagesCardiovascular System DevelopmentAdan Iman100% (1)
- Head and NeckDocument63 pagesHead and Neckbayenn100% (1)
- Ant 325materialDocument13 pagesAnt 325materialDestiny BlissNo ratings yet
- Introduction To Physical AgentsDocument25 pagesIntroduction To Physical AgentsCyril Jay G. OrtegaNo ratings yet
- Week 3 Spinal Cord, Spinal NervesDocument53 pagesWeek 3 Spinal Cord, Spinal NervesCyril Jay G. OrtegaNo ratings yet
- Compiled Lecture in Engineering Economy PDFDocument78 pagesCompiled Lecture in Engineering Economy PDFLJ dela PazNo ratings yet
- Meninges: Dr. Katharina Kian R. Demerre - BacolodDocument78 pagesMeninges: Dr. Katharina Kian R. Demerre - BacolodCyril Jay G. OrtegaNo ratings yet
- Amortization and Uniform Arithmetic GradientDocument20 pagesAmortization and Uniform Arithmetic GradientCyril Jay G. OrtegaNo ratings yet
- Basic Computer Structure and KnowledgeDocument22 pagesBasic Computer Structure and KnowledgeCyril Jay G. OrtegaNo ratings yet
- Thermodynamics 1 by Hipolito Sta. Maria (Optimized)Document79 pagesThermodynamics 1 by Hipolito Sta. Maria (Optimized)Gian Carl Doping69% (16)
- Social Studies GuideDocument3 pagesSocial Studies GuideCyril Jay G. OrtegaNo ratings yet
- Electric Circuit Variables ExplainedDocument18 pagesElectric Circuit Variables ExplainedCyril Jay G. OrtegaNo ratings yet
- Tela Choroidea - WikipediaDocument11 pagesTela Choroidea - WikipediaAbhijeetNo ratings yet
- TRANSCALLOSAL TRANSCHOROIDAL APPROACH TO Third VentriclDocument6 pagesTRANSCALLOSAL TRANSCHOROIDAL APPROACH TO Third VentriclNikolay PeevNo ratings yet
- Neuroanatomy NotesDocument26 pagesNeuroanatomy Notesdeyar janblyNo ratings yet
- Meninges وهدانDocument10 pagesMeninges وهدانوسيم جمال مياسNo ratings yet