You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Elizabeth F. Howell - Understanding and TreatingDocument331 pagesElizabeth F. Howell - Understanding and TreatingFlorance Flor100% (4)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Torc 4 Abscohort1 - CompressDocument13 pagesTorc 4 Abscohort1 - CompressFaye MartinezNo ratings yet
- MHI-18 EnglishDocument3 pagesMHI-18 Englisho77777777777777777100% (4)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- A Research Paper Presented To The Faculty of The Senior High School Department Mintal Comprehensive High School Mintal, Tugbok, Davao CityDocument57 pagesA Research Paper Presented To The Faculty of The Senior High School Department Mintal Comprehensive High School Mintal, Tugbok, Davao Cityibganraffy22No ratings yet
- Situational Leadership Theory Proposes That Effective Leadership Requires A Rational Understanding of The Situation and An Appropriate ResponseDocument6 pagesSituational Leadership Theory Proposes That Effective Leadership Requires A Rational Understanding of The Situation and An Appropriate ResponseAmar DeramanNo ratings yet
- Leadership in The Shaping ...Document18 pagesLeadership in The Shaping ...Ritika kumariNo ratings yet
- Self Esteem Study Skills Self Concept Social Support Psychological Distress and Coping Mechanism Effects On Test Anxiety and Academic PerformanceDocument9 pagesSelf Esteem Study Skills Self Concept Social Support Psychological Distress and Coping Mechanism Effects On Test Anxiety and Academic PerformanceFredrick Sibwoga KomboNo ratings yet
- Case Analysis For Does This Milkshake Taste FunnyDocument8 pagesCase Analysis For Does This Milkshake Taste FunnyRAJAT AGARWAL Student, Jaipuria LucknowNo ratings yet
- Bachelor of Science in Medical Laboratory Science Level II-B 9:05-10:30 EuthenicsDocument7 pagesBachelor of Science in Medical Laboratory Science Level II-B 9:05-10:30 EuthenicsRia Elrica DayagNo ratings yet
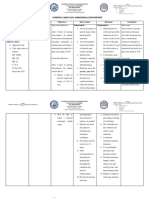
- NCP Abdominal PainDocument3 pagesNCP Abdominal PainShaina Rica TayagNo ratings yet
- SilosDocument3 pagesSilosapi-548205221100% (1)
- Lesson 9Document8 pagesLesson 9Angeline DR. CortesNo ratings yet
- Blackhawks StatementDocument2 pagesBlackhawks StatementCrains Chicago BusinessNo ratings yet
- Tatel ThesisDocument7 pagesTatel Thesisjohnmarkbriol211No ratings yet
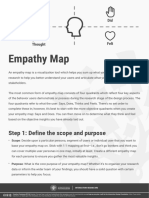
- Empathy Map: Step 1: Define The Scope and PurposeDocument7 pagesEmpathy Map: Step 1: Define The Scope and PurposeInteresado CashNo ratings yet
- Unit 1 RevisionDocument2 pagesUnit 1 Revisionđinh việt dũng -AMOOSENo ratings yet
- Diass Q1 M1Document25 pagesDiass Q1 M1Yna Kaye BalboaNo ratings yet
- Shame and AttachmentDocument8 pagesShame and AttachmentIsidora Kesić100% (1)
- Training Session Evaluation Form CheckDocument5 pagesTraining Session Evaluation Form CheckFelix Villanueva Malone Jr.No ratings yet
- Shahwan 2021. Evaluation of Computer Workstations Ergonomics and Its Relationship With Reported Musculoskeletal and Visual Symptoms Among University Employees in JordanDocument16 pagesShahwan 2021. Evaluation of Computer Workstations Ergonomics and Its Relationship With Reported Musculoskeletal and Visual Symptoms Among University Employees in JordanFioriAmeliaHathawayNo ratings yet
- Multicultural Counseling NotesDocument12 pagesMulticultural Counseling NotesCaitlyn BouldinNo ratings yet
- The Yellow Wallpaper by Charlotte Perkins Gilman RianDocument2 pagesThe Yellow Wallpaper by Charlotte Perkins Gilman RianRian Indra FadillahNo ratings yet
- Safety and Health at Work: Da-Som Choi, Sang-Hee KimDocument6 pagesSafety and Health at Work: Da-Som Choi, Sang-Hee Kimclaaa_fhrNo ratings yet
- Student Activity 5Document5 pagesStudent Activity 5tamayojenny292No ratings yet
- Digital Wellbeing: Sanmesh Sawant, Prof - Neha LodheDocument4 pagesDigital Wellbeing: Sanmesh Sawant, Prof - Neha LodheVIVA-TECH IJRINo ratings yet
- AmeworkDocument11 pagesAmeworkGeorgia De OcampoNo ratings yet
- Desmond NG - 'Stop Being A Girl and Man Up' - Boys Face Gender Police, Even As Men's Roles ChangeDocument3 pagesDesmond NG - 'Stop Being A Girl and Man Up' - Boys Face Gender Police, Even As Men's Roles ChangeFedericoNo ratings yet
- THE Foundation Self-Esteem: Terminology InadequaciesDocument6 pagesTHE Foundation Self-Esteem: Terminology Inadequaciesuki arrownaraNo ratings yet
- College of Health & Allied Sciences: Review of Related LiteratureDocument20 pagesCollege of Health & Allied Sciences: Review of Related LiteratureAngela V. De LunaNo ratings yet
- Not Until Và Only WhenDocument2 pagesNot Until Và Only Whenko bietgamingNo ratings yet