You might also like
- Trauma On Brain DevelopmentDocument29 pagesTrauma On Brain DevelopmentChirra Williams100% (1)
- Grand v. Schwarz - Brainspotting Trademark PDFDocument12 pagesGrand v. Schwarz - Brainspotting Trademark PDFMark JaffeNo ratings yet
- Trauma Therapist ToolkitDocument23 pagesTrauma Therapist ToolkitRoxana100% (1)
- Working With Traumatic Memories To Heal Adults With Unresolved Childhood Trauma - Neuroscience, Attachment Theory and Pesso Boyden System Psychomotor Psychotherapy PDFDocument305 pagesWorking With Traumatic Memories To Heal Adults With Unresolved Childhood Trauma - Neuroscience, Attachment Theory and Pesso Boyden System Psychomotor Psychotherapy PDFAlessandro Papa100% (3)
- ACEs Connected LifeDocument26 pagesACEs Connected LifeYari MarreroNo ratings yet
- Alicia F. Lieberman, Patricia Van Horn - Psychotherapy With Infants and Young Children - Repairing The Effects of Stress and Trauma On Early Attachment (2008)Document385 pagesAlicia F. Lieberman, Patricia Van Horn - Psychotherapy With Infants and Young Children - Repairing The Effects of Stress and Trauma On Early Attachment (2008)rosana80% (5)
- Dissociation Following Traumatic Stress: Etiology and TreatmentDocument19 pagesDissociation Following Traumatic Stress: Etiology and TreatmentNievesNo ratings yet
- Dissociative Amnesia: Epidemiology, Pathogenesis, Clinical Manifestations, Course, and DiagnosisDocument26 pagesDissociative Amnesia: Epidemiology, Pathogenesis, Clinical Manifestations, Course, and DiagnosisZiggy GonNo ratings yet
- Anxiety in The Wake of Loss - Strategies For Working With The Missing Stage of GriefDocument48 pagesAnxiety in The Wake of Loss - Strategies For Working With The Missing Stage of GriefAlguémNo ratings yet
- Psychological First AidDocument16 pagesPsychological First AidYerson Alarcon MoralesNo ratings yet
- Complex Childhood TraumaDocument11 pagesComplex Childhood TraumaAkinosan100% (1)
- Revised Emotion Regulation Homework Sheet 1Document1 pageRevised Emotion Regulation Homework Sheet 1rileyjenNo ratings yet
- Manual Diversity Therapy RoomDocument21 pagesManual Diversity Therapy RoomAlguémNo ratings yet
- Complex PTSDDocument21 pagesComplex PTSDRyne ZuziNo ratings yet
- Janina 1Document6 pagesJanina 1AngelesLunaJuradoNo ratings yet
- Creating A Trauma Informed Child Welfare SystemDocument10 pagesCreating A Trauma Informed Child Welfare SystemiacbermudaNo ratings yet
- The Science of NeglectDocument20 pagesThe Science of NeglectdrdrtsaiNo ratings yet
- Interoception and CompassionDocument4 pagesInteroception and CompassionMiguel A. RojasNo ratings yet
- Relationship of Resilience To Personality, Coping, and Psychiatric Symptoms in Young AdultsDocument15 pagesRelationship of Resilience To Personality, Coping, and Psychiatric Symptoms in Young AdultsBogdan Hadarag100% (1)
- Theory: PolyvagalDocument2 pagesTheory: PolyvagalWayne CasanovaNo ratings yet
- Brief Family-Based Crisis Intervention (Cftsi) - Stephen BerkowitzDocument20 pagesBrief Family-Based Crisis Intervention (Cftsi) - Stephen Berkowitzapi-279694446No ratings yet
- The Polyvagal Parenting Playbook: A Comprehensive Guide to Interactive Strategies for Every Age and StageFrom EverandThe Polyvagal Parenting Playbook: A Comprehensive Guide to Interactive Strategies for Every Age and StageNo ratings yet
- FZ6 Vs Z750Document6 pagesFZ6 Vs Z750Andrea Manca100% (1)
- TlctraumaDocument7 pagesTlctraumaapi-356243627No ratings yet
- Domestic Violence - Shrey & MusabDocument6 pagesDomestic Violence - Shrey & MusabMusab AlbarbariNo ratings yet
- Bowlby - The Nature of The Child's Tie To His MotherDocument26 pagesBowlby - The Nature of The Child's Tie To His Motherinna_rozentsvit100% (1)
- 50 Risks To Take With Your KidsDocument211 pages50 Risks To Take With Your KidsVăn Hải NguyễnNo ratings yet
- Grief During The Pandemic Internet-Resource-GuideDocument76 pagesGrief During The Pandemic Internet-Resource-GuideAnastasija TanevaNo ratings yet
- World Handbook of Existential TherapyDocument10 pagesWorld Handbook of Existential TherapyFaten SalahNo ratings yet
- Star Conference Feeling Buddies - Our JourneyDocument27 pagesStar Conference Feeling Buddies - Our JourneyfernandapazNo ratings yet
- Srimadbhagwata Mahapuran With MahabharataDocument505 pagesSrimadbhagwata Mahapuran With Mahabharataprapnnachari100% (6)
- Article Taming The Terrible MomentsDocument3 pagesArticle Taming The Terrible Momentsapi-232349586No ratings yet
- Profile of A Therapeutic CompanionDocument3 pagesProfile of A Therapeutic CompanionPatricia BaldonedoNo ratings yet
- Emdr Protocol Standard En-GbDocument4 pagesEmdr Protocol Standard En-GbNadia100% (1)
- NICABM InfoG StructuralDissociationModelDocument2 pagesNICABM InfoG StructuralDissociationModelssjeliasNo ratings yet
- What Happened To You Book Discussion Guide-National VersionDocument7 pagesWhat Happened To You Book Discussion Guide-National Versionaulia normaNo ratings yet
- NICABM InfoG Window of Tolerance RevisedDocument1 pageNICABM InfoG Window of Tolerance Revisedsemsem0% (1)
- Congresso Roma BROCHURE ENG DefDocument13 pagesCongresso Roma BROCHURE ENG DefISCFormazione100% (1)
- Teens in Distress SeriesDocument4 pagesTeens in Distress SeriesdarinaralucaNo ratings yet
- Lanius & Frewen 2006 - Toward A PsychobiologyDocument15 pagesLanius & Frewen 2006 - Toward A PsychobiologyCarlos Eduardo NorteNo ratings yet
- Appearance Is Not Always: - We Don't Need A Secure BaseDocument4 pagesAppearance Is Not Always: - We Don't Need A Secure BaseMike ChristopherNo ratings yet
- Taylor 2006 Tend and BefriendDocument6 pagesTaylor 2006 Tend and BefriendGer RubiaNo ratings yet
- CFT HandoutsDocument49 pagesCFT HandoutsEsmeralda Herrera100% (2)
- Hydrogenium Homeopathic RemedyDocument6 pagesHydrogenium Homeopathic RemedySatya PalNo ratings yet
- The 10 Steps & Ogden'S Sensorimotor PsychotherapyDocument29 pagesThe 10 Steps & Ogden'S Sensorimotor Psychotherapydocwavy9481No ratings yet
- Trauma Solutions Relational Empowerment Training Slides PDFDocument23 pagesTrauma Solutions Relational Empowerment Training Slides PDFihcammaNo ratings yet
- Attachment TheoryDocument4 pagesAttachment TheoryMohammedseid AhmedinNo ratings yet
- Grief and Narrative TherapyDocument13 pagesGrief and Narrative TherapySidney OxboroughNo ratings yet
- Play Theraphy (Unfinished)Document21 pagesPlay Theraphy (Unfinished)OmyNo ratings yet
- Ensink 2014 Mentalización TraumaDocument15 pagesEnsink 2014 Mentalización TraumaDanielaMontesNo ratings yet
- Adverse Childhood ExperiencesDocument9 pagesAdverse Childhood Experiencesapi-487854212No ratings yet
- Liotti Trauma Attachment 2004Document39 pagesLiotti Trauma Attachment 2004samathacalmmindNo ratings yet
- Part 1 Artificial Window of Tolerance WorkbookDocument28 pagesPart 1 Artificial Window of Tolerance WorkbookFaten SalahNo ratings yet
- Death Anxiety and Its Association With Hypochondriasis PDFDocument8 pagesDeath Anxiety and Its Association With Hypochondriasis PDFRebeca SilvaNo ratings yet
- Early Interaction and Developmental Psychopathology: Volume I: Infancy Gisèle Apter Emmanuel Devouche Maya GratierDocument229 pagesEarly Interaction and Developmental Psychopathology: Volume I: Infancy Gisèle Apter Emmanuel Devouche Maya GratierRoberto Alexis Molina Campuzano100% (1)
- Motor ArduinoDocument41 pagesMotor ArduinoyankurokuNo ratings yet
- Guilt and ChildrenFrom EverandGuilt and ChildrenJane BybeeNo ratings yet
- DOD-MST-INS-002, MST For Installation of Field Instruments.-Rev-1Document15 pagesDOD-MST-INS-002, MST For Installation of Field Instruments.-Rev-1BharathiNo ratings yet
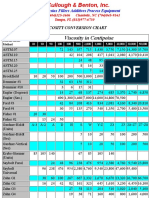
- Viscosity Conversion ChartDocument2 pagesViscosity Conversion ChartCorvetteNo ratings yet
- Schore2001 PDFDocument69 pagesSchore2001 PDFMihaela ButucaruNo ratings yet
- Dennis McGuire: Mental Wellness and Good Health in Teens and Adults With Down SyndromeDocument23 pagesDennis McGuire: Mental Wellness and Good Health in Teens and Adults With Down SyndromeGlobalDownSyndromeNo ratings yet
- Briere ITCT-A Final PDFDocument119 pagesBriere ITCT-A Final PDFDave HenehanNo ratings yet
- Stress and Personality DDocument7 pagesStress and Personality DAdriana NegrescuNo ratings yet
- Trauma Guideline Manual PDFDocument157 pagesTrauma Guideline Manual PDFsilviaemohNo ratings yet
- 12 Quarter 1 Module 12 - Timeline-Of-ExtinctionDocument13 pages12 Quarter 1 Module 12 - Timeline-Of-ExtinctionMah Jane Divina100% (1)
- Strategic Significance of Arabian SeaDocument4 pagesStrategic Significance of Arabian SeaShamshad Ali RahoojoNo ratings yet
- Advances in Fatigue Analysis TechnologiesDocument38 pagesAdvances in Fatigue Analysis TechnologiesMarcelino Pereira Do NascimentoNo ratings yet
- Deep Audio ClassificationDocument10 pagesDeep Audio ClassificationVinayNo ratings yet
- PP No. 61 Tahun 2009 (Kepelabuhan) English VersionDocument54 pagesPP No. 61 Tahun 2009 (Kepelabuhan) English VersionSetyaning KartikaNo ratings yet
- Notes On Eigenvalues 1Document9 pagesNotes On Eigenvalues 1Vivian BiryomumaishoNo ratings yet
- National Building Code of The Philippines SummaryDocument2 pagesNational Building Code of The Philippines SummaryScott AlilayNo ratings yet
- Designated Airspace HandbookDocument153 pagesDesignated Airspace HandbookBradley NorthcotteNo ratings yet
- IMGS - QTF - A20 - For Cargo VesselDocument4 pagesIMGS - QTF - A20 - For Cargo VesselLion DayNo ratings yet
- IUPAC - Practice SheetDocument5 pagesIUPAC - Practice SheetRishi NairNo ratings yet
- Normal Distribution and Standard Normal DistributionDocument46 pagesNormal Distribution and Standard Normal DistributionazmanrafaieNo ratings yet
- On The Optimal Weighting Matrix For The GMM System Estimator in Dynamic Panel Data ModelsDocument28 pagesOn The Optimal Weighting Matrix For The GMM System Estimator in Dynamic Panel Data ModelsNeemaNo ratings yet
- 21wcss Programacao Final PDFDocument279 pages21wcss Programacao Final PDFlocometrallaNo ratings yet
- Grendel ZodiacDocument3 pagesGrendel ZodiacSteven LaiNo ratings yet
- Bowex KaplinDocument30 pagesBowex Kaplinmustafa çetinkayaNo ratings yet
- Grade 6 Maths Practice Sheet Decimals (Ekam and Ena) (01!09!2017)Document5 pagesGrade 6 Maths Practice Sheet Decimals (Ekam and Ena) (01!09!2017)praschNo ratings yet
- CBSE Class 11 Physics Notes For Properties of Bulk MatterDocument20 pagesCBSE Class 11 Physics Notes For Properties of Bulk MatterAyush Kumar100% (1)
- Neligan Vol 4 Chapter 10 MainDocument20 pagesNeligan Vol 4 Chapter 10 MainisabelNo ratings yet
- FO-SHE-02 Risk Assessment FormDocument2 pagesFO-SHE-02 Risk Assessment FormNeil OsenaNo ratings yet
- Law Essay SampleDocument8 pagesLaw Essay Sampleheffydnbf100% (2)
- Respuestas AtlanticaDocument5 pagesRespuestas AtlanticaWilson Zambrano0% (1)
- Jurnal Antropologi: Isu-Isu Sosial Budaya: Modal Sosial Kelompok Rentan Sebagai UpayaDocument10 pagesJurnal Antropologi: Isu-Isu Sosial Budaya: Modal Sosial Kelompok Rentan Sebagai UpayaSari IntanNo ratings yet
- Nikon Metrology SolutionsDocument44 pagesNikon Metrology SolutionsBinh NguyenNo ratings yet