Professional Documents
Culture Documents
Nursing Lessons
Uploaded by
Jarod HembradorOriginal Description:
Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Nursing Lessons
Uploaded by
Jarod HembradorCopyright:
Available Formats
APPENDECTOMY NURSING PROCESS: UNDERGOING AMPUTATION
surgical removal of the appendix which is done Assessment
ASAP to decrease the risk of perforation
neurovascular and functional status of extremity
performed using GA or spinal anesthesia with a
assess function and condition of residual limb
laparotomy or by laparoscopy (faster recovery)
check circulatory status and function of
Nursing Management unaffected extremity
C&S test is obtained to determine appropriate
relieve pain, prevent FVD, reduce anxiety,
antibiotic therapy
eliminate infection, maintain skin integrity, and
diet: protein and vitamins to promote healing
attain optimal nutrition
assess psychological status and emotional
prepare for surgery, infuse IV to replace fluid loss
reaction to amputation
and promote renal function and antibiotic
therapy Diagnosis
with increased risk of paralytic ileus, NGT is
Nursing Diagnoses
inserted and an enema is no given – perforation
after surgery, place in a high-Fowler’s position to Acute pain r/t amputation
reduce tension on incision & abdominal organs Disturbed sensory perception: phantom limb
opioid (morphine sulfate) is given to relieve pain pain r/t amputation
when normal bowel sounds are present, food is Impaired skin integrity r/t surgical amputation
provided as desired and tolerated on the day of Disturbed body image r/t amputation
the surgery Grieving or risk for complicated grieving r/t loss
instruct to make an appointment to have of body part and resulting disability
surgeon remove sutures between the 5th-7th Self-care deficit: feeding, bathing/hygiene,
days after surgery dressing/ grooming, or toileting, r/t loss of
normal activity can be resumed within 2-4 weeks extremity
discharge teachings must include incision care Impaired physical mobility r/t loss of extremity
and dressing changes and irrigations, as needed
Potential Complications
BELOW-KNEE AMPUTATION
Postoperative hemorrhage
preferred because of the importance of the knee Infection
joint and the energy requirements for walking Skin Breakdown
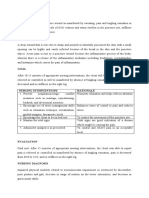
Complications Planning and Nursing Interventions
hemorrhage, infection, skin breakdown, 1. Relieving pain
phantom limb pain (d/t severing of peripheral
controlled with opioid analgesics that may be
nerves), and joint contracture (d/t positioning
accompanied with evacuation of hematoma or
and a protective flexion withdrawal pattern)
accumulated fluid
bleeding, infection, and skin break down
changing position and placing a light sandbag
Medical Management on residual limb to counteract muscle spasm
healing is enhanced by gentle handling of the 2. Minimizing Altered Sensory Perceptions
residual limb, control of residual limb edema
when patient describes phantom pains,
through rigid or soft compression dressings, and
acknowledge feelings as real and encourage
use of aseptic technique in wound care
verbalization when in pain
after surgery, a sterilized residual limb sock is
keeping patient active helps decrease incidence
applied to the residual limb
distraction techniques, TENS, UTZ, or local
cast is changed in about 10-14 days and a
anesthesia may provide relief
removable rigid dressing may be placed over a
beta-blockers may relieve dull, burning pain
soft dressing to control edema, prevent joint
anti-seizures control stabbing or cramping pain
flexion contracture, and protect residual limb
TCAs alleviate phantom pain and improve mood
residual limb wound hematomas are controlled
with wound drainage devices to avoid infection
RLE SEMIFINALS LYNETTESKIE
3. Promoting Wound Healing explain s/s to be reported to the physician
aseptic technique for wound dressing changes Evaluation
if cast/dressing comes off, immediately wrap the
Expected outcomes may include:
limb with an elastic compression bandage to
prevent development of excessive edema 1. Experiences no pain
ace wraps are discouraged because they may 2. Experiences no phantom limb pain
apply inconsistent pressure 3. Achieves wound healing
4. Demonstrates improved body image and
4. Enhancing Body Image
effective coping
encourage to look at, feel, and care for residual 5. Exhibits resolution of grieving
limb and identify strengths and resources to 6. Achieves independent self-care
facilitate rehabilitation 7. Achieves maximum independent mobility
8. Exhibits absence of complications of
5. Helping the Patient to Resolve Grieving
hemorrhage, infection, or skin breakdown
create an accepting and supportive atmosphere DIABETES MELLITUS
in which they are encouraged to share feelings
Epidemiology
6. Promoting Independent Self-care
risk factors
practicing an activity with consistent supervision family history
in a relaxed environment obesity
independence in dressing, toileting, and bathing race/ethnicity
depends on balance, transfer abilities, and ≥ 45 years old
physiologic tolerance impaired fasting glucose or impaired
7. Helping the Patient to Achieve Physical Mobility glucose tolerance
HPN (≥ 140/90 mmHg)
proper positioning and avoid placing on a pillow HDL ≤ 35 mg/dL and/or triglyceride ≥
to prevent hip/knee joint contracture 250 mg/dL
abduction, external rotation, and flexion are history of gestational diabetes of
avoided and residual limb is placed in an delivery of babies > 9 lb
extended position or elevated for a brief period leading cause of non-traumatic amputations,
encourage turning to sides and assume prone blindness, and ESRD
position to prevent flexion contracture of the hip 3rd leading cause of disease d/t high rate of CVD
ROM exercises include hip and knee exercises among people with DM
patient must practice position changes and
transfer techniques, as well as good posture Pathophysiology
assist to stand between parallel bars to allow insulin is secreted by beta cells and when a
extension of temporary prosthesis person eats, secretion increases and moves
teach members of family the bandaging method glucose from the blood into muscle, liver, and fat
8. Monitoring and Managing Potential Complications cells
other roles of insulin include
reestablish homeostasis and prevent transports/metabolizes glucose for
complications r/t surgery, anesthesia, and energy
immobility stimulates storage of glucose (glycogen)
monitor for s/s of bleeding, VS, suction drainage signals liver to stop release of glucose
administer antibiotics and monitor incision, enhances storage of fat in adipose tissue
drainage, and dressing for infection accelerates transport of amino acids
careful skin hygiene to prevent skin breakdown inhibits breakdown of stored glucose,
healed residual limb is wash & dried ≥ 2x a day protein, and fat
insulin and glucagon maintain a constant level
9. Promoting Home and Community-based Care
of glucose in the blood by stimulating its release
give ongoing instructions and practice sessions from the liver
RLE SEMIFINALS LYNETTESKIE
Type 1 DM Clinical Manifestations
acute onset, usually before 30 years of age and polyuria, polydipsia, and polyphagia
is characterized by destruction of pancreatic the first 2 Ps occur d/t excess fluid loss with
beta cells osmotic diuresis and polyphagia results from the
genetic tendency to develop T1DM is found in catabolic state induced by insulin deficiency
people with HLA types (human leukocyte fatigue, weakness, sudden vision changes,
antigen) tingling or numbness, dry skin, lesions/wounds
there is an evidence of an autoimmune response that are slow to heal, and recurrent infections
destruction of beta cells results in decreased T1DM onset: sudden weight loss, N/V, or
insulin production, unchecked glucose abdominal pains, if DKA has developed
production, and fasting hyperglycemia
Assessment and Dx Findings
osmotic diuresis – excess glucose is excreted in
urine accompanied by excessive loss of F&E fasting plasma glucose, random PG, and glucose
diabetic ketoacidosis – accumulation of ketones level 2 hrs. after receiving glucose may be used
d/t fat breakdown and may cause abdominal OGTT and IV GTT are no longer recommended
pain, N/V, hyperventilation, and a fruity breath
Type 2 DM
occurs more commonly among people who are
older than 30 years of age and obese
insulin resistance – decreased insulin sensitivity
to overcome IR, increased amounts of insulin
must be secreted to maintain the glucose level
and is called metabolic syndrome
hypertension
hypercholesterolemia
abdominal obesity
DKA does not typically occur in T2DM because
there is enough insulin to prevent the
breakdown of fat and production of ketones
slow, progressive glucose intolerance; onset may
go undetected for many years
mild symptoms including fatigue, irritability,
polyuria, polydipsia, poor healing skin wounds,
vaginal infections, or blurred vision Medical Management
Gestational DM intensive treatment: 3-4 insulin injections per
day or continuous subcutaneous insulin infusion,
onset: during pregnancy d/t secretion of
insulin pump therapy plus frequent monitoring,
placental hormones, causing insulin resistance
and weekly contacts with diabetes educators
if pt. is high-risk and does not have GDM at 1st
management: nutritional therapy, exercise,
screening, must be retested bet. 24-28 wks. AOG
monitoring, pharmacologic therapy, education
initial management: dietary changes and blood
glucose monitoring and if hyperglycemia Nutritional Therapy
persists, insulin is preseribed
control of total caloric intake to attain or
goal: ≤ 105 mg/dL before meals and ≤ 130
maintain a reasonable body weight, control of
mg/dL 2 hours after meals
blood glucose levels, and normalization of lipids
Prevention and BP to prevent CVD
for obese patients, weight loss is key treatment
standard lifestyle recommendations, metformin,
meals should not be skipped but intake must be
placebo, or an intensive program of lifestyle
controlled
modifications
RLE SEMIFINALS LYNETTESKIE
thorough review of diet history, eating habits, Pharmacologic Therapy
and lifestyle – first step for meal planning
insulin therapy
total cholesterol intake < 300 mg/day
T1DM: life-long exogenous insulin
decreased protein and increased fiber intake
T2DM: long-term to control glucose
food classification systems include exchange
insulin regimens vary from 1-4 injections/day
lists, nutritional labels, healthy food choices,
and there is usually a combination of short and
food guide pyramid, and glycemic index
longer-acting insulin
alcohol consumption must be moderated: 1
conventional
beverage/day for women and 2/day for men
intensive: reduced risk of complications
moderation in the amount of sweetener to avoid
contraindications for intensive insulin regimen
potential adverse effects
nervous system disorders
Exercise recurring severe hypoglycemia
irreversible diabetic complications
lowers blood glucose levels by increasing uptake
cerebrovascular of CV disease
of glucose by body muscles and improving
ineffective self-care skills
insulin utilization
complications of insulin therapy
regular daily exercise at the same time and in the
local allergic reactions
same amount each day is recommended
systemic allergic reactions
those with blood glucose > 250 mg/dL and
insulin lipodystrophy
ketouria must not begin exercising until urine
resistance to injected insulin
test results are negative and closer to normal
morning hyperglycemia
Gerontologic Considerations methods of insulin delivery
insulin pens
use of proper footwear, avoid exercise in
jet injectors
extreme temperatures, inspect feet after
insulin pumps (risk for ketoacidosis)
exercise, and avoid exercise during poor
future insulin delivery
metabolic control periods
transplantation of pancreatic cells
gradual, consistent exercise (with resistance) oral antidiabetic agents
should be planned as tolerated by the elderly sulfonylureas, biguanides, and alpha-
Monitoring Glucose Levels and Ketones glucose inhibitors
non-sulfonylurea insulin secretogogues
self-monitoring of blood glucose allows for thiazolidinediones
detection and prevention of hypo or dipeptide-peptidase-4
hyperglycemia other pharmacologic therapy
SMBG is recommended for the following pramlintide: synthetic analogue of
unstable diabetes (severe swings) human amylin for T1 and T2 DM
tendency to develop severe ketosis or exenatide: derived from a hormone
hypoglycemia produced in the small intestine for T2
hypoglycemia without warning DM only
symptoms
recommended 2-4 times daily before meals and Nursing Management
at bedtime Providing Patient Education
continuous glucose monitoring uses a sensor
attached to an infusion set and is inserted reinforcement of self-management skills
subcutaneously in the abdomen (72 hours) teaching survival skills (simple pathophysiology,
testing for glycated hemoglobin is a blood treatment modalities, recognition/treatment
test reflecting ave. BG levels over a period of and prevention of acute complications,
approx. 2-3 months pragmatic information)
testing for ketones using a urine dipstick to preventive measures (foot/eye care, general
detect ketonuria hygiene, and risk factor management)
self-administration of insulin: storing, selecting
syringes, mixing insulins, withdrawing, selecting
RLE SEMIFINALS LYNETTESKIE
and rotating injection site, skin preparation, proinflammatory state (high levels of C-
needle insertion, and disposing of sharps reactive protein)
prothrombic state (high fibrinogen)
Promoting Home and Community-based Care
to det. overall CV risk, hs-CRP test results with
patient empowerment, behavior change, self- other screening tools are viewed
efficacy, and health beliefs r/t insulin regimen
Prevention
CORONARY ARTERY DISEASE
Controlling Cholesterol Abnormalities
most prevalent type of CVD in adults
LDL < 100 mg/dL
I. CORONARY ATHEROSCLEROSIS total cholesterol < 200 mg/dL
HDL > 60 mg/dL
atherosclerosis – abnormal accumulation of lipid
triglyceride < 150 mg/dL
and fibrous tissue in the lining or arterial blood
weight loss, cessation of tobacco use, and
vessels
increased physical activity (30 min. moderate
Pathophysiology exercise on most days)
lipid-lowering agents can reduce CAD mortality
genetics and environmental factors are involved with elevated lipid levels
in the progression of these lesions
involves an inflammatory response which begins Promoting Cessation of Tobacco Use
with injury to the vascular endothelium
those who stop smoking reduce their risk of
atheromas or plaques protrude into the lumen
heart disease within the first year and the risk
of the vessel, narrowing it and obstructing blood
continues to decline as long as they refrain
flow
meds such as nicotine patch or the
vulnerable plaque – thin cap with inflammation
antidepressant bupropion may assist with
ruptured plaque – focus for thrombus formation
stopping use of tobacco
may lead to acute coronary syndrome (ACS)
resulting in an acute myocardial infarction (MI) Managing Hypertension
Clinical Manifestations early detection and serious adherence to
therapy can prevent the serious consequences
ischemia – deprivation of cardiac muscle cells of
with untreated elevated BP
oxygen needed for survival
angina pectoris – pain brought by myocardial Controlling DM
ischemia
treatment with insulin and metformin and other
a decrease in blood supply from CAD may cause
therapeutic interventions that lower plasma
sudden cardiac death
glucose levels can lead to improved endothelial
dyspnea, nausea, and weakness, prodromal
function
symptoms, or a major cardiac event
Gender
Risk Factors
in women > 55 years of age, the incidence of
CAD risk equivalents: CAD, diabetes, PAD, AAA,
CAD is approx. equal to that in men
or carotid artery disease
women also tend to have a higher incidence of
age (M: > 45 y/o; W: > 55 y/o), systolic
complications from CVD and a higher mortality
BP/hypertension, DM, obesity/physical inactivity,
menopause is a milestone in the aging process
smoking history, level of total cholesterol, level
during which risk factors tend to accumulate
of LDL, and level of HDL
women continue to have poorer outcomes, with
metabolic syndrome (major risk factor for CVD)
increased morbidity and mortality after MI,
whose diagnosis includes 3 of the ff. conditions
CABG, and PCI
insulin resistance
central obesity II. ANGINA PECTORIS
dyslipidemia
episodes or paroxysms of pain or pressure in the
BP persistently > 130/85 mmHg
anterior chest
RLE SEMIFINALS LYNETTESKIE
Pathophysiology calcium channel blockers – negative inotropic
effects; for those not responsive to beta-
caused by atherosclerotic disease and assoc.
blockers; primary TOC for vasospasm
with a significant obstruction of at least one
increase myocardial oxygen supply
major coronary artery
1st gen. CCBs must be avoided in people
types of angina include stable angina, unstable
with HF (reduce myocardial contractility)
angina, intractable or refractory angina,
antiplatelet – prevention of platelet aggregation
variant/Prinmental’s angina, and silent ischemia
aspirin, clopidogrel
factors associated with angina are the following
heparin: effective when aPTT is 2-2.5
physical exertion ( oxygen demand)
times the normal aPTT value
exposure to cold (vasoconstriction and
apply bleeding precautions
elevated BP)
glycoprotein IIb/IIIa agents: unstable
eating a heavy meal (decreases blood
angina and adjunct for PCI
supply to the heart)
anticoagulants – prevention of thrombus
stress/emotion-provoking situation
formation
(releases catecholamines)
Nursing Interventions for Patient with Angina
Clinical Manifestations
1. Treating Angina
pain or other symptoms such as mild
indigestion, choking or heavy sensation in the during an attack, patient must stop all activities,
upper chest accompanied by severe sit or rest in bed in a semi-Fowler’s position to
apprehension and a feeling of impending death reduce oxygen requirements
weakness or numbness in the arms, wrists, and measure VS and observe for respiratory distress
hands, SOB, pallor, diaphoresis, dizziness, N/V nitroglycerin is given SL and patient’s response
important characteristics: subsides with rest or is checked and administration is repeated up to
nitroglycerin 3 doses, if needed
oxygen is given at 2 L/min by nasal cannula, even
Gerontologic Considerations
without evidence of respiratory distress
earliest sign: dyspnea, sometimes there are no
2. Reducing Anxiety
symptoms
stress testing and cardiac catheterization may be stress reduction methods must be done and
used to diagnose CAD in the elderly spiritual needs are addressed
Assessment and Dx Findings 3. Preventing Pain
history r/t clinical manifestations of ischemia alternate rest and activity periods
12-lead ECG (T-wave inversion), laboratory
studies such as CRP and cardiac biomarkers to 4. Promoting Home and Community-Based Care
rule out an ACS, nuclear scan, or invasive discuss the disease process, s/s, actions to take,
procedure and methods to prevent chest pain and
Medical Management advancement of CAD
any pain unrelieved within 15 min. by the usual
Pharmacologic Therapy methods (nitroglycerin) should be treated at the
nitroglycerin – short and long term reduction of closest emergency center
myocardial oxygen consumption through III. ACUTE CORONARY SYNDROME (ACS) AND
vasodilation MYOCARDIAL INFARCTION (MI)
beta-blockers – reduction of myocardial oxygen
consumption by blocking beta-adrenergic emergent situation characterized by an acute
stimulation of the heart onset of myocardial ischemia that results in
CI include hypotension, bradycardia, myocardial death
advanced AV block, and acute HF
RLE SEMIFINALS LYNETTESKIE
Pathophysiology 3. NSTEMI (Non-STEMI)
unstable/pre-infarction angina – reduced blood elevated cardiac biomarkers but no definite ECG
flow in a CA, often d/t rupture of an evidence of acute MI
atherosclerotic plaque, but artery is not
completely occluded Laboratory Tests
MI – area of myocardium is permanently
destroyed leading to complete occlusion of the CK-MB is the cardiac-specific isoenzyme:
artery increases only when there has been damage to
vasospasm of CA, ↓ O2 supply, and demand cardiac cells (acute MI)
for oxygen are other causes of MI as cells are myoglobin – negative results are an excellent
deprived of oxygen, ischemia develops, cellular parameter for ruling out an acute MI
injury occurs, and the lack of oxygen results in troponin – regulates contractile process
infarction troponins I and T are biomarkers which
ECG usually identifies type and location of MI are reliable and critical markers of
Q-wave and pt. history identify the timing myocardial injury
Clinical Manifestations Medical Management
chest pain (sudden and continues with rest and re-perfuse the area with the emergency use of
medication) with ACS thrombolytic medications or by Percutaneous
SOB, indigestion, nausea, anxiety Coronary Intervention
cool, pale, moist skin reducing myocardial O2 demand and increasing
HR and RR are faster than normal O2 supply with medications, O2 administration,
stimulated sympathetic nervous system and bed rest
Assessment and Diagnostic Findings
12-lead ECG to clarify whether unstable angina,
NSTEMI, or STEMI
ECG should be obtained within 10 minutes from
the time a patient reports pain or arrives in the
emergency department
T-wave inversion, ST-segment elevation, and
development of an abnormal Q wave
first ECG signs of an acute MI occur as a result of
myocardial ischemia and injury
key diagnostic indicator for MI: elevation in the
ST segment in two contiguous leads
decreased urinary output may indicate
cardiogenic shock
echocardiogram is used when ECG is non-
diagnostic
1. Unstable Angina
clinical manifestations of coronary ischemia, but
ECG and cardiac biomarkers show no evidence Pharmacologic Therapy
of acute MI
given aspirin (162 to 325 mg), nitroglycerin,
2. STEMI morphine, an IV beta-blocker, and other
medications as indicated while the diagnosis is
ECG evidence of acute MI with characteristic being confirmed
changes in 2 contiguous leads on a 12-lead ECG long-term therapy with beta-blockers can
significant damage to the myocardium decrease the incidence of future cardiac events
RLE SEMIFINALS LYNETTESKIE
unfractionated heparin or an LMWH is O2 administration along with meds (2-4 L/min)
prescribed along with platelet-inhibiting agents physical rest in bed with backrest elevated or in
to prevent further clot formation a supportive chair to decrease chest discomfort
analgesic of choice for acute MI is morphine in and dyspnea
IV boluses to reduce pain and anxiety
decreases workload of the heart and 2. Improving Respiratory Function
enhances oxygenation
monitor fluid volume status to prevent
ACE-inhibitors – decreases BP, facilitates
overloading the heart and lungs
diuresis, and decreases O2 demand of heart
encourage the patient to breathe deeply and
ensure patient is not hypotensive,
change position frequently
hyponatremic, hypovolemic, or
hyperkalemic 3. Promoting Adequate Tissue Perfusion
BP, urine output, and Na, K, and
creatinine levels are closely checked bed or chair rest during the initial phase of
thrombolytics – given to dissolve the thrombus treatment helps reduce myocardial oxygen
in a CA, allowing reperfusion, minimizing the size consumption
of the infarction and preserving ventricular check skin temperature and peripheral pulses
function frequently to monitor tissue perfusion
Emergent PCI 4. Reducing Anxiety
usually for patients with STEMI, may also be decreased sympathetic stimulation decreases
indicated in patients with unstable angina and the workload of the heart, which may relieve
NSTEMI who are at high risk due to persistent pain and other s/s
ischemia 5. Monitoring and Managing Potential Complications
procedure treats the underlying atherosclerotic
lesion monitor the patient closely for changes in
cardiac rate and rhythm, heart sounds, BP, chest
Cardiac Rehabilitation pain, respiratory status, urinary output, skin color
and temperature, sensorium, ECG changes, and
important continuing care program for patients
laboratory values
with CAD that targets risk reduction by means of
education, individual and group support, and 6. Promoting Home and Community-Based Care
physical activity
target heart rate during hospitalization is an teaching patients self-care
increase of less than 10% from the resting heart continuing care: home-care or follow-up
rate, or 120 bpm PLEURAL EFFUSION
Phases of Cardiac Rehabilitation a collection of fluid in the pleural space, rarely a
primary disease process; usually secondary to
Phase 1 – diagnosis of atherosclerosis
other diseases
Phase 2 – after discharge
attends sessions three times a week for Pathophysiology
4 to 6 weeks but may continue for as
effusion can be relatively clear fluid, or it can be
long as 6 months
bloody or purulent
supervised, often ECG-monitored,
transudative (clear) effusion implies that pleural
exercise training
membranes are not diseased and most
Phase 3 – long-term outpatient program which
commonly results from HF
focuses on maintaining cardiovascular stability
exudative effusion results from inflammation by
and long-term conditioning; self-directed phase
bacterial products or tumors in the pleural space
Nursing Interventions for Patient with ACS Clinical Manifestations
1. Relieving pain and other s/s of ischemia pneumonia causes fever, chills, and pleuritic
chest pain
RLE SEMIFINALS LYNETTESKIE
malignant effusion may result in dyspnea, Post-operative Management
difficulty lying flat, and coughing
major risks: infection and hemorrhage
Assessment and Dx Findings an indwelling catheter may be inserted d/t
edema or nerve trauma causing temporary loss
decreased or absent breath sounds, decreased
of bladder tone
fremitus, and a dull, flat sound on percussion
extremely large PE: acute respiratory distress and Nursing Interventions for Patient Undergoing
tracheal deviation away from affected side Hysterectomy
physical examination, CXR, chest CT, and
1. Relieving Anxiety
thoracentesis confirm the presence of fluid
provide explanations about preparations and
Medical Management
procedures to be performed
thoracentesis – remove fluid, obtain specimen, address outcomes of surgery, possible feelings
and relieve dyspnea and respiratory compromise of loss, and options for management of
pleurodesis – chemically irritating agent is symptoms of menopause
instilled or aerosolized into the pleural space
2. Improving Body Image
surgical pleurectomy – insertion of small
catheter attached to a drainage bottle provide reassurance regarding sexual
implantation of pleuroperitoneal shunt relationships, function, and satisfaction
Nursing Management 3. Relieving Pain
prepare and position patient for thoracentesis assess intensity and assist with analgesia as
and offer support throughout the procedure prescribed
record and send fluid amount to the laboratory fluids and food may be restricted for 1-2 days
monitor water-seal system’s function and record passage of flatus indicates peristalsis (facilitated
drainage amount at prescribed intervals by ambulation) and is a sign for permission of a
if chest tube is inserted, pain management is a soft diet
priority and help patient assume positions that
4. Monitoring and Managing Potential Complications
are least painful
TOTAL ABDOMINAL HYSTERECTOMY AND hemorrhage – to detect early, count perineal
BILATERAL SALPINGO-OOPHORECTOMY pads used, assess saturation with blood, and
monitor VS
surgical removal of the uterus to treat cancer, abdominal dressings are monitored for
dysfunctional uterine bleeding, endometriosis, drainage
nonmalignant growths, persistent pain, pelvic give prescribed guidelines for activity
relaxation and prolapse, and previous injury to restrictions to promote healing and
the uterus prevent bleeding
total hysterectomy involves removal of the DVT – caused by positioning, post-op edema,
uterus and the cervix and decreased post-op activity
TAHBSO is usually required in malignant anti-embolism stockings
conditions frequent position changes
Pre-operative Management legs and feet exercises while in bed
assist in early ambulation
discontinue anticoagulant medications, NSAIDs, assess for DVT/phlebitis and PE
and vitamin E to reduce the risk of bleeding avoid prolonged sitting with pressure at
prophylactic antibiotics are given prior to the knees and inactivity
surgery and discontinued the next day bladder dysfunction – after catheter is
prevention of thromboembolic events: heparin, removed, urinary output and abdominal
anti-embolism stockings, intermittent distention is monitored and assessed
pneumatic compression device
5. Promoting Home and Community-Based Care
RLE SEMIFINALS LYNETTESKIE
provide information tailored to patient’s needs thoracotomy (surgery) is done if > 1500 mL of
such as limitations or restrictions to be expected blood is aspirated by thoracentesis or if chest
instruct to check incision daily and contact tube output continues > 200 mL/hr
primary HC provider if redness/purulent before the procedure, prophylactic antibiotics
drainage/discharge occurs may be given and also pain medications, as
remind about importance of adequate oral prescribed
intake and maintaining bowel and UT function
Complications
encourage to resume activities gradually
instruct to avoid straining, lifting, sex, or driving serious infections such as pneumonia
until surgeon permits hemorrhagic shock
remind about the different s/s to be reported cardiac arrest
empyema – pus gathers in pleural space
HEMOPNEUMOTHORAX
respiratory failure
hemothorax – collection of blood in pleural
THYROIDECTOMY
space resulting from torn intercostal vessels,
laceration of the great vessels, or laceration of total thyroidectomy is indicated for certain
the lungs carcinomas and to relieve tracheal or
hemopneumothorax – collection of blood and esophageal compression
air in the chest cavity needs lifelong thyroid replacement
most often occurs as a result of a wound to the therapy because hypocalcemia may
chest (traumatic pneumothorax) and can also occur (no more production of PTH
occur spontaneously without an apparent cause which stimulates calcium production)
(spontaneous pneumothorax) surgical removal of about 5/6 of the thyroid
to treat this condition, blood and air must be tissue/gland (subtotal thyroidectomy) results in
drained from the chest using a tube and a a prolonged remission with exophthalmic goiter
surgery may be needed to repair a wound/injury beta-adrenergic blockers may be used to reduce
HR and other s/s of hyperthyroidism
Clinical Manifestations
iodine may be given to reduce blood loss
pain which is usually sudden and/or pleuritic medications that could prolong clotting are
if pneuomothorax is large, the lung collapses stopped several weeks prior to surgery
totally, resulting in acute respiratory distress nursing priorities: managing hyperthyroid state
anxiety, agitation, hypotension, tachycardia, pre-op, relieving pain, providing info about the
profuse diaphoresis, dyspnea, air hunger, surgery, prognosis, and treatment needs, and
increased use of accessory muscles, and central prevent complications
cyanosis from severe hypoxemia
Position
sudden chest pain which gets worse after
coughing or taking a deep breath, chest supine with rolled towel or sandbag between the
tightness scapulae, hyperextending the neck
if table is in reverse Trendelenberg position, a
Medical Management
padded foot board should be used to prevent
in an emergency, anything may be used that is the patient from slipping down
large enough to fill the chest wound
Pre-operative Teaching
patient is instructed to inhale and strain against
a closed glottis to re-expand lungs and eject air nausea and vomiting may be present 24 hours
from the thorax post-op due to general anesthetic agents
in the hospital, the opening is sealed with gauze anti-emetics will be ordered on a PRN basis
impregnated with petrolatum post-op diet will begin with clear liquids and
pleural cavity can be decompressed by needle advance as tolerated when N/V resolves
aspiration (thoracentesis) or by chest tube head of the bed will be elevated by 30 degrees
drainage (thoracostomy) of the blood ad air ambulation and sitting in chair is encouraged
when awake and alert
RLE SEMIFINALS LYNETTESKIE
support head and back of neck when rising to parts of the body (meninges, kidneys, bones, and
sitting position or lying down lymph nodes)
pain medication will be given (IV) on PRN basis M. tuberculosis is an acid-fast aerobic rod that
drain is surgically placed under skin and grows slowly and is sensitive to heat and UV light
attached to suction to facilitate healing
Transmission
suture line care 2-4 times/day when dressing is
not in place and continued until sutures are airborne transmission; infected person releases
removed droplet nuclei through talking, coughing,
inform of the s/s of hypocalcemia: (+) Chvostek’s sneezing, laughing, or singing
and Trousseau’s sign and decreased serum
Risk Factors
calcium levels
avoid constrictive clothing around neck close contact with someone who has active TB
immunocompromised status
Potential Complications
substance abuse
hypocalcemia, vocal cord paralysis without adequate health care
hematoma, bleeding, and infection preexisting medical conditions or special
transverse neck scar treatment
immigration from countries with a high
Post-operative Teachings/Interventions
prevalence of TB
Wound Care institutionalization
living in overcrowded, substandard housing
place ice bag on the neck wound to reduce
being a health care worker performing high-risk
swelling and pain
activities
frequently check wound dressing and skin near
and on the wound site for any bleeding Pathophysiology
support neck when changing positions or sitting
begins when a susceptible person inhales
speak as little as possible during first few days
mycobacteria and becomes infected
Diet bacteria are transmitted through the airways to
the alveoli, deposited and begin to multiply
cold liquid food may be given when fully aware
body’s immune system responds with an
and if N/V subsides and peristalsis returns, soft
inflammatory reaction
diet may be given as prescribed
phagocytes engulf many of the bacteria, and TB-
include high-protein in diet to promote healing
specific lymphocytes lyse the bacilli and normal
avoid ingesting irritants such as coffee and cola
tissue
Activity and Movement results in accumulation of exudate in the alveoli
– bronchopneumonia
elevate head of bed 25-35 degrees to keep
initial infection: 2-10 weeks after exposure
respiratory tract unobstructed and for sputum to
granulomas are surrounded by macrophages,
be expelled
forming a protective wall
massage back of neck every 1-2 hours for
material becomes necrotic, forming a cheesy
relaxation
mass which may become calcified and form a
patient may get out of bed on the 2nd day postop
collagenous scar
Home Care bacteria become dormant and there is no further
progression of active disease
report s/s such as spasms from any extremity
Ghon tubercle ulcerates, releasing cheesy
during the 1st week, fever, restlessness,
material into the bronchi, the bacteria then
irritability, palpitations, cyanosis, DOB, neck
become airborne
muscle tightness, and wound swelling
ulcerated tubercle heals and forms scar tissue
PULMONARY TUBERCULOSIS and infected lung becomes more inflamed
infectious disease primarily affecting the lung
parenchyma and may be transmitted to other
RLE SEMIFINALS LYNETTESKIE
Clinical Manifestations class 3: disease; clinically active
class 4: disease; not active
low-grade fever, cough, night sweats, fatigue,
class 5: suspected disease; pending
and weight loss
hemoptysis may occur and both systemic & Gerontologic Considerations
pulmonary symptoms are chronic and may have
symptoms may include unusual behavior and
been present for weeks to months
altered mental status, fever, anorexia, and
Assessment and Dx Findings weight loss
tuberculin skin test produces no reaction or
history, PE, tuberculin skin test, chest x-ray, acid-
delayed reactivity for up to 1 week; a 2nd skin test
fast bacillus smear, and sputum culture
is done in 1-2 weeks
CXR reveals lesions in the upper lobes and acid-
fast bacillus smear contains mycobacteria Pharmacologic Therapy
assess lungs for consolidation by evaluating
anti-tuberculosis agents for 6-12 months
breath sounds, fremitus, and egophony
INH, rifampin, pyrazinamide, and ethambutol
Tuberculin Skin Test capreomycin, ethionamide, para-aminosalicylate
sodium, and cycloserine are second-line drugs
Mantoux method – standardized intracutaneous
initial phase: intensive-treatment given daily for
injection procedure and should be performed
8 weeks
only by those trained in its administration and
continuation phase: additional 4 or 7 months
reading
7-month period: recommended for those with
TB extract and purified protein derivative are
cavitary pulmonary TB whose sputum culture
injected into the intradermal layer of the inner
after the initial 2 months of treatment is positive,
aspect of the forearm, 4 inches below the elbow
those initial phase did not include PZA, and
test result is read 48-72 hours after injection and
those treated once weekly with INH and
tests read after 72 hours tend to underestimate
rifapentine whose sputum culture is (+) at the
the true size of induration/hardening
end of the initial phase
a reaction occurs when both induration and
non-infectious: after 2-3 weeks of continuous
erythema are present
medication therapy
0-4 mm: insignificant
prophylactic INH treatment involves taking daily
≥ 5 mm: significant in people at risk
doses for 6 to 12 months
a significant reaction indicates past exposure to
M. tuberculosis or vaccination with BCG vaccine Nursing Management
the more intense the reaction, the greater the
Promoting Airway Clearance
likelihood of an active infection
increase fluid intake and correct positioning to
QuantiFERON-TB Gold Test
facilitate airway drainage
ELISA that detects the release of interferon-
Advocating Adherence to Treatment
gamma by WBCs when the blood of a patient
with TB is incubated with peptides similar to teach patient that TB is communicable and
those in M. tuberculosis taking medications is the most effective way to
results are available in < 24 hours prevent transmission
a (+) QFT-G only indicates that a person has instruct to take meds either on an empty
been infected with TB and does not indicate stomach or at least 1 hour before meals
whether or not the disease is active monitor for other side effects of anti-TB drugs
inform about risk of drug resistance
Classification
Promoting Activity and Adequate Nutrition
data from the history, PE, TB test, CXR, and
microbiologic studies are used to classify TB plan progressive activity schedule that focuses
class 0: no exposure/infection on increasing activity tolerance and muscle
class 1: exposure; no infection strength
class 2: latent infection; no active
disease
RLE SEMIFINALS LYNETTESKIE
a nutritional plan that allows small, frequent
meals may be required
Preventing Spread of Infection
instruct about hygiene measures: moth care,
covering mouth and nose when coughing and
sneezing, proper disposal of tissues, and
handwashing
military TB is the spread of TB infection to
nonpulmonary sites of the body and has the
same treatment regimen with pulmonary TB
RLE SEMIFINALS LYNETTESKIE
You might also like
- Haematology NotesDocument184 pagesHaematology NotesJason royNo ratings yet
- Nursing Care PlansDocument13 pagesNursing Care PlansAngelie Sanchez86% (14)
- CLARENCE TIU - Civil Procedure Rule 1-36 Notes (Last Edit-June 2017) PDFDocument270 pagesCLARENCE TIU - Civil Procedure Rule 1-36 Notes (Last Edit-June 2017) PDFJarod HembradorNo ratings yet
- LaminectomyDocument22 pagesLaminectomyAnonymous 0C4OZmRNo ratings yet
- Length Tension Testing Book 2, Upper Quadrant: A Workbook of Manual Therapy TechniquesFrom EverandLength Tension Testing Book 2, Upper Quadrant: A Workbook of Manual Therapy TechniquesRating: 1 out of 5 stars1/5 (1)
- Basic ECG ReadingDocument41 pagesBasic ECG ReadingBenj100% (4)
- Total Joint ReplacementDocument10 pagesTotal Joint Replacementapi-3764215No ratings yet
- Respiratory System22Document11 pagesRespiratory System22anandbro093No ratings yet
- Length Tension Testing Book 1, Lower Quadrant: A Workbook of Manual Therapy TechniquesFrom EverandLength Tension Testing Book 1, Lower Quadrant: A Workbook of Manual Therapy TechniquesRating: 3.5 out of 5 stars3.5/5 (3)
- NCP OsteoporosisDocument5 pagesNCP OsteoporosisAnonymous gAwcPNVRNo ratings yet
- Comprehensive Nursing Care PlanDocument3 pagesComprehensive Nursing Care PlanJaylord VerazonNo ratings yet
- Open Reduction Internal Fixation PPT With Nursing ResponsibilitiesDocument13 pagesOpen Reduction Internal Fixation PPT With Nursing ResponsibilitiesMiciola Mitch Tanquiamco100% (2)
- Open Reduction and Internal Fixation (ORIF)Document13 pagesOpen Reduction and Internal Fixation (ORIF)Miciola Mitch Tanquiamco50% (2)
- NCP Impaired Skin IntegrityDocument2 pagesNCP Impaired Skin IntegrityEden Marie Francisco100% (2)
- Nursing Diagnosis Related ToDocument9 pagesNursing Diagnosis Related ToGrape JuiceNo ratings yet
- The Musculoskeletal HandoutsDocument3 pagesThe Musculoskeletal Handoutsseigelystic100% (11)
- VanPutte Seeleys Essentials 11e Chap11 PPT AccessibleDocument49 pagesVanPutte Seeleys Essentials 11e Chap11 PPT AccessibleJoshua UyNo ratings yet
- Regaining Bladder Control: For Incontinence on Exertion or Following Pelvic SurgeryFrom EverandRegaining Bladder Control: For Incontinence on Exertion or Following Pelvic SurgeryNo ratings yet
- 4 Amputation Nursing Care Plans - Nurseslabs-1 PDFDocument12 pages4 Amputation Nursing Care Plans - Nurseslabs-1 PDFsaidi MwanamongaNo ratings yet
- NCP - Acute Pain - FractureDocument1 pageNCP - Acute Pain - Fracturemawel73% (22)
- Lesson Plan MIDocument14 pagesLesson Plan MIAnand Bhawna100% (1)
- Nursing Care Plan-1idealDocument30 pagesNursing Care Plan-1idealSheila Mae PanisNo ratings yet
- Assessment Nursing Diagnosis Planning Implementation Scientific Rationale EvaluationDocument5 pagesAssessment Nursing Diagnosis Planning Implementation Scientific Rationale Evaluationjennelyn losanta100% (2)
- NCP AppendicitisDocument2 pagesNCP Appendicitismnms0708100% (2)
- NCP CVA ImmoblityDocument3 pagesNCP CVA ImmoblityAnalyn FloresNo ratings yet
- NCP ImmobilityDocument1 pageNCP ImmobilityBcoi QuilacioNo ratings yet
- Assessmen T Nursing Diagnosi S Nursing Goal Nursing Intervention Rationale Subjective Cues: Independent IndependentDocument3 pagesAssessmen T Nursing Diagnosi S Nursing Goal Nursing Intervention Rationale Subjective Cues: Independent IndependentKim Glaidyl BontuyanNo ratings yet
- NCPDocument2 pagesNCPJanice SolamilloNo ratings yet
- Geria NCP, Dela CruzDocument7 pagesGeria NCP, Dela CruzStephany Dela CruzNo ratings yet
- Report Hard Copy TemplateDocument4 pagesReport Hard Copy TemplateBaileyNo ratings yet
- Nursing Care PlanDocument5 pagesNursing Care PlanLaceth Joyce T. LASATNo ratings yet
- Prostatic CancerDocument3 pagesProstatic CancerShakour El seifyNo ratings yet
- Springfield Technical Community College School of Nursing NURS 202-Nursing Care PlanDocument1 pageSpringfield Technical Community College School of Nursing NURS 202-Nursing Care Plannata654dNo ratings yet
- Total Joint ReplacementDocument10 pagesTotal Joint Replacementmardsz100% (6)
- Problem List 1. Acute Pain 2. Nutrition Less Than Body Requirements 3. Impaired Physical Mobility 4. Impaired Skin Integrity 5. Disturbed Body ImageDocument12 pagesProblem List 1. Acute Pain 2. Nutrition Less Than Body Requirements 3. Impaired Physical Mobility 4. Impaired Skin Integrity 5. Disturbed Body Imagebernadette babaranNo ratings yet
- EXTERNALDocument2 pagesEXTERNALMarissa AsimNo ratings yet
- Assessment Nursing Diagnosis PlanningDocument2 pagesAssessment Nursing Diagnosis PlanningCamille RamosNo ratings yet
- NURSING DIAGNOSIS: Impaired Bone Tissue Perfusion Related To ContinuationDocument5 pagesNURSING DIAGNOSIS: Impaired Bone Tissue Perfusion Related To ContinuationmasterlouieNo ratings yet
- Nursing Care Plan Format Name: - Medical Diagnosis: - DateDocument2 pagesNursing Care Plan Format Name: - Medical Diagnosis: - DateSheryl Ann Barit PedinesNo ratings yet
- Subjective: The PatientDocument2 pagesSubjective: The PatientRoscoe ParaanNo ratings yet
- REF 14 Managing The Elbow Stiffness GrosslyDocument14 pagesREF 14 Managing The Elbow Stiffness GrosslyZahra YousafNo ratings yet
- ArthritisDocument10 pagesArthritisAhana CherianNo ratings yet
- NCP Cholecystectomy RevisedDocument7 pagesNCP Cholecystectomy RevisedMa. Ferimi Gleam BajadoNo ratings yet
- Nursing Intervention (Risk For Trauma) RationaleDocument5 pagesNursing Intervention (Risk For Trauma) RationaleJay VillasotoNo ratings yet
- Bicipital TenosynovitisDocument4 pagesBicipital TenosynovitisMegan SaltmerNo ratings yet
- Nursing Care: Fracture Jay VillasotoDocument11 pagesNursing Care: Fracture Jay VillasotoJay VillasotoNo ratings yet
- CECS ProtocolDocument6 pagesCECS ProtocolTsz Kwan CheungNo ratings yet
- Nursing DiagnosisDocument4 pagesNursing DiagnosisEnzo DyNo ratings yet
- NCP Sas 10Document2 pagesNCP Sas 10Shyn MargarethNo ratings yet
- Nursing Care Plan Cues Nursing Diagnosis Analysis Goal Intervention Rationale Evaluatio NDocument3 pagesNursing Care Plan Cues Nursing Diagnosis Analysis Goal Intervention Rationale Evaluatio NAishleen OrmandoNo ratings yet
- Gastrocnemius Slide SurgeryDocument2 pagesGastrocnemius Slide SurgeryHein Aung ZawNo ratings yet
- Burn NCPDocument37 pagesBurn NCPmildred alidonNo ratings yet
- NCP (BD)Document5 pagesNCP (BD)Nursing LectureNo ratings yet
- Nursing Care Plan (Surgical, CS)Document5 pagesNursing Care Plan (Surgical, CS)Nursing LectureNo ratings yet
- Nursing Care PlanDocument4 pagesNursing Care PlanLjae NatinoNo ratings yet
- Greenhill 2017Document4 pagesGreenhill 2017BSPT BooksNo ratings yet
- NCP604Document2 pagesNCP604Dorice AchiengNo ratings yet
- Limb AmputationDocument4 pagesLimb Amputationxllxxcxm -No ratings yet
- CP: Dislocation of Prosthesis: Nursing Interventions RationaleDocument5 pagesCP: Dislocation of Prosthesis: Nursing Interventions Rationaleapi-3822433No ratings yet
- APPENDICITISDocument15 pagesAPPENDICITISTiffany AdriasNo ratings yet
- Or NCPDocument5 pagesOr NCPjelopigar921No ratings yet
- Nursing Care Plan2Document3 pagesNursing Care Plan2Fc CrisostomoNo ratings yet
- Pre and Post-Operative Care of Patient For Mastectomy: Prepared By: Gianne T. Gregorio RNDocument13 pagesPre and Post-Operative Care of Patient For Mastectomy: Prepared By: Gianne T. Gregorio RNmalathiNo ratings yet
- Amputation 4th YearDocument57 pagesAmputation 4th Yearshubham raulNo ratings yet
- Fast Facts: Perioperative Pain: Effective management has numerous benefitsFrom EverandFast Facts: Perioperative Pain: Effective management has numerous benefitsNo ratings yet
- BSN 4 - First Sem - Batch 2022 - : Fiscal PlanningDocument6 pagesBSN 4 - First Sem - Batch 2022 - : Fiscal PlanningJarod HembradorNo ratings yet
- NCM 119 - Aug. 19, 2021: Emergency Nursing Principles of Emergency CareDocument2 pagesNCM 119 - Aug. 19, 2021: Emergency Nursing Principles of Emergency CareJarod HembradorNo ratings yet
- NCM 119 Rle Emergency CartDocument6 pagesNCM 119 Rle Emergency CartJarod HembradorNo ratings yet
- Osce ChecklistDocument9 pagesOsce ChecklistXeric CedoNo ratings yet
- NSP Oec Ch30 LectureDocument63 pagesNSP Oec Ch30 LecturemaithamNo ratings yet
- Birth Asphyxia: Walter Otieno Consultant PaediatricianDocument21 pagesBirth Asphyxia: Walter Otieno Consultant PaediatricianMalueth AnguiNo ratings yet
- Peel 1996 - Cardiopulmonary System and Movement DysfunctionDocument8 pagesPeel 1996 - Cardiopulmonary System and Movement DysfunctionBeto ZamunérNo ratings yet
- Organisation of The Organism (Multiple Choice) 1 QPDocument16 pagesOrganisation of The Organism (Multiple Choice) 1 QPforyourhonour wongNo ratings yet
- Plant and Animal Tissues: By: Bryce Pimentel, Bruce Pimentel, John Philip Pacho, Matthew ElacionDocument13 pagesPlant and Animal Tissues: By: Bryce Pimentel, Bruce Pimentel, John Philip Pacho, Matthew ElacionArchan Dom ReyesNo ratings yet
- 1circulatory SystemDocument26 pages1circulatory SystemElisa EstebanNo ratings yet
- Yung Mga Na Ka Red Na Questions, Wrong Ba Yung Nakablack Na Answer?????Document44 pagesYung Mga Na Ka Red Na Questions, Wrong Ba Yung Nakablack Na Answer?????KC White Dela RosaNo ratings yet
- CVADocument13 pagesCVAAmlan jyoti thanapatiNo ratings yet
- Christopher Cheung Approach To Cardiac History Taking: Cyanosis or SyncopeDocument6 pagesChristopher Cheung Approach To Cardiac History Taking: Cyanosis or SyncopeApryl Phyllis JimenezNo ratings yet
- Performance Gains Following Resistance Breathing Exercises: Single Subject Case StudyDocument4 pagesPerformance Gains Following Resistance Breathing Exercises: Single Subject Case StudysdjuknicNo ratings yet
- Principles of Human Physiology 5th Edition Stanfield Test BankDocument26 pagesPrinciples of Human Physiology 5th Edition Stanfield Test Banksiennaadelaideatknmp100% (27)
- Heart Failure: Diagnosis and EvaluationDocument29 pagesHeart Failure: Diagnosis and Evaluation黃昱睿No ratings yet
- When Should Blood Pressure Be Measured?: Stage Approximate Age Systolic DiastolicDocument6 pagesWhen Should Blood Pressure Be Measured?: Stage Approximate Age Systolic DiastolicJesrel DelotaNo ratings yet
- A Systematic Approach To The Unconscious PatientDocument5 pagesA Systematic Approach To The Unconscious PatientDoctor RadiologistNo ratings yet
- Vanoxerine: Cellular Mechanism of A New AntiarrhythmicDocument10 pagesVanoxerine: Cellular Mechanism of A New Antiarrhythmicapi-26169290No ratings yet
- Biological Psychology 11Th Ed by James Kalat - Test BankDocument105 pagesBiological Psychology 11Th Ed by James Kalat - Test Bankthivyaashini SellaNo ratings yet
- Body Fluid CompartmentsDocument4 pagesBody Fluid Compartmentsvishnupriya sethuramanNo ratings yet
- Lab Exercise On Blood: .What Is The Blood Volume of An Avernge-Sized Adult Male?Document4 pagesLab Exercise On Blood: .What Is The Blood Volume of An Avernge-Sized Adult Male?سهى الغامديNo ratings yet
- Concept Map 1Document3 pagesConcept Map 1Rubie Ann TillorNo ratings yet
- Modulzáró Szociális Gondozó - ÁpolóDocument4 pagesModulzáró Szociális Gondozó - ÁpolóCsilla Kovalecz-SzabóNo ratings yet
- Zoology Paper IDocument4 pagesZoology Paper IAsad Ali BalochNo ratings yet
- Case Abstract Sir ErikkkkDocument16 pagesCase Abstract Sir ErikkkkLeah Mae TomasNo ratings yet
- The Human Body OrientationDocument6 pagesThe Human Body OrientationHenry BuñagNo ratings yet
- Tolleno Drug Study (Hemo Dialysis)Document5 pagesTolleno Drug Study (Hemo Dialysis)Hannah TollenoNo ratings yet