You might also like
- Battling COVID-19: How I Survived and Tips on How to Stay SafeFrom EverandBattling COVID-19: How I Survived and Tips on How to Stay SafeNo ratings yet
- One Children's Place: Inside a Children's HospitalFrom EverandOne Children's Place: Inside a Children's HospitalRating: 3.5 out of 5 stars3.5/5 (3)
- Young Person With Long COVID After Mild DiseaseDocument4 pagesYoung Person With Long COVID After Mild DiseaseAline RangelNo ratings yet
- A Chance Meeting with Life: Inside an Intensive Care Unit, and OutFrom EverandA Chance Meeting with Life: Inside an Intensive Care Unit, and OutNo ratings yet
- Jesus and Chemo: On a Rock in a Hard Place, 2nd EditionFrom EverandJesus and Chemo: On a Rock in a Hard Place, 2nd EditionNo ratings yet
- The Night Shift: Real Life in the Heart of the E.R.From EverandThe Night Shift: Real Life in the Heart of the E.R.Rating: 4 out of 5 stars4/5 (20)
- Getting Through Cancer: A 32-Year-Old Woman’s Journey and Her Quest for Life’s Meaning. Based on a Personal StoryFrom EverandGetting Through Cancer: A 32-Year-Old Woman’s Journey and Her Quest for Life’s Meaning. Based on a Personal StoryNo ratings yet
- Articles of FARRINGTON, HarveyDocument14 pagesArticles of FARRINGTON, HarveyMuhammad Ata Ul MustafaNo ratings yet
- Patient by Patient: Lessons in Love, Loss, Hope, and Healing from a Doctor's PracticeFrom EverandPatient by Patient: Lessons in Love, Loss, Hope, and Healing from a Doctor's PracticeRating: 4.5 out of 5 stars4.5/5 (8)
- Saving Grace: What Patients Teach Their Doctors about Life, Death, and the Balance in BetweenFrom EverandSaving Grace: What Patients Teach Their Doctors about Life, Death, and the Balance in BetweenNo ratings yet
- Relapse!: And the Legacy of Thyroid Cancer: Living With Thyroid Cancer, #3From EverandRelapse!: And the Legacy of Thyroid Cancer: Living With Thyroid Cancer, #3No ratings yet
- How to Get Out of the Hospital Alive: A Guide to Patient PowerFrom EverandHow to Get Out of the Hospital Alive: A Guide to Patient PowerNo ratings yet
- Burning Rubber: A Memoir of Travelling Wheelchairs in AsiaFrom EverandBurning Rubber: A Memoir of Travelling Wheelchairs in AsiaNo ratings yet
- A License to Heal: Recollections of an ER DoctorFrom EverandA License to Heal: Recollections of an ER DoctorRating: 5 out of 5 stars5/5 (1)
- The Smile Behind The MaskDocument2 pagesThe Smile Behind The MaskAnroe CariasoNo ratings yet
- AdM Home Care Coaching: Family Guide to Improved HealthFrom EverandAdM Home Care Coaching: Family Guide to Improved HealthNo ratings yet
- Hospital Hijinks: A Patient's Memoir: Destiny of a Delinquent Memoir Series #1From EverandHospital Hijinks: A Patient's Memoir: Destiny of a Delinquent Memoir Series #1No ratings yet
- Pulmonary Fibrosis: Coping With a Terminal DiseaseFrom EverandPulmonary Fibrosis: Coping With a Terminal DiseaseRating: 5 out of 5 stars5/5 (1)
- The Diary of a Covid-19 Widow: Including Reflections and Tips for Coping (Part-1)From EverandThe Diary of a Covid-19 Widow: Including Reflections and Tips for Coping (Part-1)No ratings yet
- Flipped: A Drug-Induced Journey to the Event Horizon of InsanityFrom EverandFlipped: A Drug-Induced Journey to the Event Horizon of InsanityNo ratings yet
- Path To Diagnosis: PerspectiveDocument2 pagesPath To Diagnosis: PerspectiveInternational Journal of Clinical and Biomedical Research (IJCBR)No ratings yet
- Nursing During the Outbreak...What I saw, what I felt, and why I chose to stay.From EverandNursing During the Outbreak...What I saw, what I felt, and why I chose to stay.No ratings yet
- A Measure of Truth: The Realistic Idealism, Philosophy Based on EvidenceFrom EverandA Measure of Truth: The Realistic Idealism, Philosophy Based on EvidenceNo ratings yet
- A Path Through the Cancer Fields: A Guide for Patients and FamiliesFrom EverandA Path Through the Cancer Fields: A Guide for Patients and FamiliesNo ratings yet
- Beating Endo: How to Reclaim Your Life from EndometriosisFrom EverandBeating Endo: How to Reclaim Your Life from EndometriosisNo ratings yet
- Strength, Resilience and Triumph: Living with Hydrocephalus: My StoryFrom EverandStrength, Resilience and Triumph: Living with Hydrocephalus: My StoryNo ratings yet
- Clinical ExemplarDocument5 pagesClinical Exemplarapi-283481267No ratings yet
- Listen Listening... : Lake Effect Contributor Bruce Campbell Reads His Essay "Waiting For Coronavirus."Document3 pagesListen Listening... : Lake Effect Contributor Bruce Campbell Reads His Essay "Waiting For Coronavirus."RIMZA RANINo ratings yet
- Assignment Solutions - 161Document5 pagesAssignment Solutions - 161Prof OliviaNo ratings yet
- HP Scanjet 7200s2Document2 pagesHP Scanjet 7200s2Darío FalconíNo ratings yet
- 61xx Service Manual Rev C ml60 70xv 70xvDocument178 pages61xx Service Manual Rev C ml60 70xv 70xvIago NunesNo ratings yet
- How Do Solar Panels WorkDocument6 pagesHow Do Solar Panels WorkprabuparthibanNo ratings yet
- Firdian - Bouguer Anomaly Calculator With MATLAB GUI - Grou A8 - Geophysics ComputationDocument10 pagesFirdian - Bouguer Anomaly Calculator With MATLAB GUI - Grou A8 - Geophysics ComputationFirdianNo ratings yet
- Vantage Card Services ApplicationDocument6 pagesVantage Card Services ApplicationSuraj MohapatraNo ratings yet
- Matrix MLM PlanDocument4 pagesMatrix MLM Plantest1435No ratings yet
- How To Master A Language EasilyDocument22 pagesHow To Master A Language EasilyCharmaine AlipayoNo ratings yet
- Primary Level Care of MalariaDocument26 pagesPrimary Level Care of Malariaokwadha simionNo ratings yet
- Liza Gashi's Emphasis On Ethics Within The Kosovo GovernmentDocument5 pagesLiza Gashi's Emphasis On Ethics Within The Kosovo GovernmentBOHR International Journal of Business Ethics and Corporate GovernanceNo ratings yet
- Islam: A Handbook OnDocument219 pagesIslam: A Handbook OnAfzal AhmadNo ratings yet
- Lab-1: Lab AssignmentsDocument11 pagesLab-1: Lab AssignmentsVaibhav GuptaNo ratings yet
- RPH Module 1Document3 pagesRPH Module 1John William TolentinoNo ratings yet
- The Probability of Spontaneous Regression of Lumbar Herniated Disc - A Systematic ReviewDocument12 pagesThe Probability of Spontaneous Regression of Lumbar Herniated Disc - A Systematic ReviewIsrael VillarrealNo ratings yet
- Proposal of Solar PowerDocument9 pagesProposal of Solar PowerShibu Kumar SNo ratings yet
- Motivation Letter of InternshipDocument1 pageMotivation Letter of InternshipMiftahNo ratings yet
- WINDS (Meteorology) ModuleDocument9 pagesWINDS (Meteorology) ModuleApril Caesar LibarraNo ratings yet
- PL511 URP LECTURE005 - Urban Structure ModelsDocument52 pagesPL511 URP LECTURE005 - Urban Structure Modelsarkiosk100% (3)
- Unit VDocument18 pagesUnit VDr.P. Siva RamakrishnaNo ratings yet
- Management Information and Control Systems Learning Facilitator: Prof. Ashok Kumar WahiDocument16 pagesManagement Information and Control Systems Learning Facilitator: Prof. Ashok Kumar WahisandyjbsNo ratings yet
- A Proof of Tychonoff's TheoremDocument2 pagesA Proof of Tychonoff's TheoremRamya DattaNo ratings yet
- Resource Allocation: Class 7: 3/9/11Document64 pagesResource Allocation: Class 7: 3/9/11Tyas AgustinaNo ratings yet
- Phenomenon of Vortex BreakdownDocument14 pagesPhenomenon of Vortex BreakdownManjul SharmaNo ratings yet
- DR Arpit Agarwal Pharma Capsule 12 - Cholinergic DrugsDocument20 pagesDR Arpit Agarwal Pharma Capsule 12 - Cholinergic DrugsarpitsnmcNo ratings yet
- 1000 Promises of GOD Joy CherionDocument30 pages1000 Promises of GOD Joy Cherionsatish2k3No ratings yet
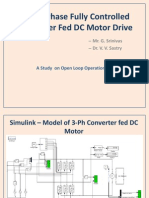
- 3-Ph Converter Fed DC MotorDocument11 pages3-Ph Converter Fed DC MotorSrinivas GudeNo ratings yet
- 6 - Time Response Analysis 2Document21 pages6 - Time Response Analysis 2حساب ويندوزNo ratings yet
- 08 - Chapter 2 PDFDocument27 pages08 - Chapter 2 PDFom prakashNo ratings yet
- Antidepressants in Pregnancy4 2016Document60 pagesAntidepressants in Pregnancy4 2016هناء همة العلياNo ratings yet