You might also like
- Holistic Baby Acupressure System: 12 Acupressure Points for Pediatric Sleep Improvement and Wellness SupportFrom EverandHolistic Baby Acupressure System: 12 Acupressure Points for Pediatric Sleep Improvement and Wellness SupportNo ratings yet
- Hypnosis for a Joyful Pregnancy and Pain-Free Labor and DeliveryFrom EverandHypnosis for a Joyful Pregnancy and Pain-Free Labor and DeliveryNo ratings yet
- Antenatal Self-Hypnosis For Labour and Childbirth: A Pilot StudyDocument6 pagesAntenatal Self-Hypnosis For Labour and Childbirth: A Pilot StudyRahma WatiNo ratings yet
- Hypno 1Document7 pagesHypno 1Eka AfriliaNo ratings yet
- Analgesia For Labour: An Evidence-Based Insight For The ObstetricianDocument9 pagesAnalgesia For Labour: An Evidence-Based Insight For The ObstetricianDiana NeculceaNo ratings yet
- Semple Self Hypnosis For Labour and Birth p16-20 Dec11 PDFDocument5 pagesSemple Self Hypnosis For Labour and Birth p16-20 Dec11 PDFEverly Christian CorputtyNo ratings yet
- Anesthesia Research ChildbirthDocument7 pagesAnesthesia Research ChildbirthPutri Ramadiana SariNo ratings yet
- Clinical Hypnosis in Paediatric OncologyDocument7 pagesClinical Hypnosis in Paediatric OncologyihsansabridrNo ratings yet
- Interventions For The Prevention of Pain Associated With The Placement of Intrauterine Contraceptives: An Updated ReviewDocument14 pagesInterventions For The Prevention of Pain Associated With The Placement of Intrauterine Contraceptives: An Updated ReviewLeonardo Daniel MendesNo ratings yet
- HypnobirthingDocument5 pagesHypnobirthingBrili AnenoNo ratings yet
- Management of Pain Associated With The Insertion of Intrauterine ContraceptivesDocument9 pagesManagement of Pain Associated With The Insertion of Intrauterine ContraceptivesLeonardo Daniel MendesNo ratings yet
- Jurnal Remifentanyl For Pain LaborDocument11 pagesJurnal Remifentanyl For Pain LaborAshadi CahyadiNo ratings yet
- Poster Session I: Results: ResultsDocument2 pagesPoster Session I: Results: ResultsCoc OfclansNo ratings yet
- Neetu, Poonam Sheoran, Rashmi PanchalDocument6 pagesNeetu, Poonam Sheoran, Rashmi PanchalMuzdalifah Karina DMNo ratings yet
- Shaw Battista2017Document14 pagesShaw Battista2017Laura RojasNo ratings yet
- ABM ProtocoloDocument7 pagesABM ProtocoloRetina MaranhaoNo ratings yet
- Perry: Maternal Child Nursing Care, 4 Edition: Chapter 16: Management of Discomfort Test Bank Multiple ChoiceDocument12 pagesPerry: Maternal Child Nursing Care, 4 Edition: Chapter 16: Management of Discomfort Test Bank Multiple ChoiceChristopher Endicott100% (3)
- Effects of Continuous Midwifery Labour Support For Women With Severe Fear of ChildbirthDocument5 pagesEffects of Continuous Midwifery Labour Support For Women With Severe Fear of ChildbirthBadriatus SholihahNo ratings yet
- A Randomised Controlled Trial of Care Of20160818-27475-1nxd8l8-With-Cover-Page-V2Document12 pagesA Randomised Controlled Trial of Care Of20160818-27475-1nxd8l8-With-Cover-Page-V2linggaNo ratings yet
- History of Past IllnessDocument4 pagesHistory of Past IllnesspachichoyNo ratings yet
- Conti 2018Document7 pagesConti 2018Felicia HalimNo ratings yet
- Acta Obstet Gynecol Scand - 2020 - Broberg - Effect of Supervised Group Exercise On Psychological Well Being Among PregnantDocument10 pagesActa Obstet Gynecol Scand - 2020 - Broberg - Effect of Supervised Group Exercise On Psychological Well Being Among PregnantReni Tri AstutiNo ratings yet
- Infertility TreatmentDocument7 pagesInfertility TreatmentWulan CerankNo ratings yet
- Research About HypnobirthingDocument4 pagesResearch About HypnobirthingMarsaidNo ratings yet
- Manejo Del Dolor en RNDocument30 pagesManejo Del Dolor en RNtadessetogaNo ratings yet
- Self-Hypnosis For Sleep Disturbances - OTTEpdfDocument3 pagesSelf-Hypnosis For Sleep Disturbances - OTTEpdflucasaguiar1996No ratings yet
- Antenatal Intranatal PostnatalDocument4 pagesAntenatal Intranatal PostnatalEviza K. NadyaNo ratings yet
- Artikel 2 DheaDocument16 pagesArtikel 2 Dheadayana nopridaNo ratings yet
- Effect of Couple-Based Cognitive BehaviouralDocument8 pagesEffect of Couple-Based Cognitive Behaviouralaudy saviraNo ratings yet
- Labour Analgesi2Document17 pagesLabour Analgesi2manish086No ratings yet
- Birth Room ResearchDocument15 pagesBirth Room ResearchCalin BabNo ratings yet
- Ger - Leung, Brenda Takeda, Wendy Holec, Victoria. (2018)Document8 pagesGer - Leung, Brenda Takeda, Wendy Holec, Victoria. (2018)Rafael CostaNo ratings yet
- Sedation and Analgesia in Children Undergoing Invasive ProceduresDocument7 pagesSedation and Analgesia in Children Undergoing Invasive ProceduresSantosa TandiNo ratings yet
- Anesthesia and Analgesia in The NICUDocument19 pagesAnesthesia and Analgesia in The NICUPaulHerreraNo ratings yet
- Neonatal Pain Management DissertationDocument8 pagesNeonatal Pain Management DissertationWillSomeoneWriteMyPaperForMeNorman100% (1)
- Akupuntur PDFDocument5 pagesAkupuntur PDFjayanti indrayaniNo ratings yet
- Evidence Based Practices For The Fetal TDocument11 pagesEvidence Based Practices For The Fetal TYena KartinaNo ratings yet
- DBF and AKUPDocument10 pagesDBF and AKUPwidad syairoziNo ratings yet
- Hypnosedation CervixDocument8 pagesHypnosedation CervixihsansabridrNo ratings yet
- Apu Cunt UraDocument22 pagesApu Cunt UraAlekhine Cubas MarinaNo ratings yet
- An Evaluation of Chest Physiotherapy in The Management of Acute Bronchiolitis Changing Clinical Practice PDFDocument6 pagesAn Evaluation of Chest Physiotherapy in The Management of Acute Bronchiolitis Changing Clinical Practice PDFbuku fisioNo ratings yet
- 2010 Early CPAP Vs Surfactant in EPTI NEJMDocument10 pages2010 Early CPAP Vs Surfactant in EPTI NEJMFiorella VilcaNo ratings yet
- Keywords: Ambulatory Epidurals, Labour Analgesia, Recent AdvancesDocument12 pagesKeywords: Ambulatory Epidurals, Labour Analgesia, Recent Advancesmanish086No ratings yet
- Analgesia For Labour: An Evidence-Based Insight For The ObstetricianDocument9 pagesAnalgesia For Labour: An Evidence-Based Insight For The ObstetricianNyeinTunNo ratings yet
- Supported By: None.: AbstractsDocument1 pageSupported By: None.: AbstractsFerry DimyatiNo ratings yet
- A Review of Sleep-Promoting Medications Used in PregnancyDocument14 pagesA Review of Sleep-Promoting Medications Used in PregnancyDanitza YhovannaNo ratings yet
- Jurnal Fentanil Dan BucainDocument7 pagesJurnal Fentanil Dan BucainAdhiny IslamNo ratings yet
- Wa0008. PDFDocument12 pagesWa0008. PDFLal NandaniNo ratings yet
- Owais 2018Document57 pagesOwais 2018Guillermo MoranteNo ratings yet
- Content ServerDocument9 pagesContent ServerJohn SteplNo ratings yet
- Obsgyn 6Document13 pagesObsgyn 6Teguh SulistiyantoNo ratings yet
- Bedah Iskandar Japardi53Document8 pagesBedah Iskandar Japardi53Ria Ulfha IndrianyNo ratings yet
- Prevention of Hypotension During Spinal Anesthesia For Cesarean DeliveryDocument7 pagesPrevention of Hypotension During Spinal Anesthesia For Cesarean DeliveryPalwasha MalikNo ratings yet
- Complementary Therapies For Labour and Birth Study: A Randomised Controlled Trial of Antenatal Integrative Medicine For Pain Management in LabourDocument11 pagesComplementary Therapies For Labour and Birth Study: A Randomised Controlled Trial of Antenatal Integrative Medicine For Pain Management in LabourAini HiolaNo ratings yet
- D3kepma2a - Tika Dwi Aprilliani - P17210182044Document17 pagesD3kepma2a - Tika Dwi Aprilliani - P17210182044mufid dodyNo ratings yet
- AWARENESS AND ACCEPTABILITY OF EPIDURAL ANESTHESIA IN LABOUR AMONG PREGNANT WOMEN ATTENDING ANTENATAL CLINIC IN CENTRAL HospitalDocument34 pagesAWARENESS AND ACCEPTABILITY OF EPIDURAL ANESTHESIA IN LABOUR AMONG PREGNANT WOMEN ATTENDING ANTENATAL CLINIC IN CENTRAL Hospitalojofolasayo8No ratings yet
- Early Analgesia For Children With Acute Abdominal Pain: ObjectivesDocument8 pagesEarly Analgesia For Children With Acute Abdominal Pain: Objectivescrizt tyanNo ratings yet
- Practice Bullet In: Obstetric Analgesia and AnesthesiaDocument17 pagesPractice Bullet In: Obstetric Analgesia and AnesthesiaKatherine ReyesNo ratings yet
- Antidepressants PregnancyDocument12 pagesAntidepressants PregnancyCarolinaNo ratings yet
- Anbar Hypnosis PediatricsDocument7 pagesAnbar Hypnosis PediatricsClaudio Alonso MoyNo ratings yet
- Kehamilan EktopikDocument9 pagesKehamilan EktopikEka AfriliaNo ratings yet
- ISGH Project Presentation - Eka Mardiana ADocument9 pagesISGH Project Presentation - Eka Mardiana AEka AfriliaNo ratings yet
- Hypno 7Document11 pagesHypno 7Eka AfriliaNo ratings yet
- Hypno 11 BookIntegratingTechnologyinPositivePsychologyPracticeDocument401 pagesHypno 11 BookIntegratingTechnologyinPositivePsychologyPracticeEka Afrilia100% (1)
- Hypno 10 Complementary - and - Alternative - TherapiesDocument45 pagesHypno 10 Complementary - and - Alternative - TherapiesEka AfriliaNo ratings yet
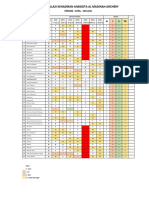
- Rekapitulasi Kehadiran Anggota Al Madinah Archery: STK H IDocument1 pageRekapitulasi Kehadiran Anggota Al Madinah Archery: STK H IEka AfriliaNo ratings yet
- ME Sci 10 Q3 1001 PSDocument17 pagesME Sci 10 Q3 1001 PSsino56601No ratings yet
- Government College of Nursing Jodhpur (Raj.) : Procedure On-Cordiotocography Subject-Obstetrics & Gynecology Specialty-IDocument6 pagesGovernment College of Nursing Jodhpur (Raj.) : Procedure On-Cordiotocography Subject-Obstetrics & Gynecology Specialty-Ipriyanka100% (1)
- Medical Terms and Definitons Commonly Used in MCNDocument15 pagesMedical Terms and Definitons Commonly Used in MCNjoemel gregoriNo ratings yet
- Essay On Vision 2020Document3 pagesEssay On Vision 2020b71p1gqh100% (2)
- Percentile RankDocument8 pagesPercentile RankJohn Philip ReyesNo ratings yet
- The Estrous CycleDocument31 pagesThe Estrous Cyclebenn_sibinNo ratings yet
- Operative Vaginal Delivery: Ralphe Robert C. CajucomDocument41 pagesOperative Vaginal Delivery: Ralphe Robert C. CajucomThea ConcepcionNo ratings yet
- Pathophysiology of Abortion Case Study (Vizconde, Ehreiz Raiden C. BSN2-A)Document4 pagesPathophysiology of Abortion Case Study (Vizconde, Ehreiz Raiden C. BSN2-A)Raiden VizcondeNo ratings yet
- Moral Issue OF Prenatal Personhood AND AbortionDocument12 pagesMoral Issue OF Prenatal Personhood AND AbortionRekkusu MakeinuNo ratings yet
- Skripsi Tanpa Bab Pembahasan PDFDocument75 pagesSkripsi Tanpa Bab Pembahasan PDFYulianaNo ratings yet
- Mechanisms of Action and Effectiveness of Contraception MethodsDocument2 pagesMechanisms of Action and Effectiveness of Contraception Methodsjaimedelafuente22No ratings yet
- NCM - 207 RLE (Delivery Room Nursing)Document9 pagesNCM - 207 RLE (Delivery Room Nursing)Tintin HonraNo ratings yet
- NCMA 217 Lec Performance Task # 3 Responsible ParenthoodDocument2 pagesNCMA 217 Lec Performance Task # 3 Responsible ParenthoodByren PacpacoNo ratings yet
- RESEARCHDocument69 pagesRESEARCHDesiree Joy GutierrezNo ratings yet
- Jurnal Sabhanga: Vol. 1 No. 2 Juli 2019: 111-116Document6 pagesJurnal Sabhanga: Vol. 1 No. 2 Juli 2019: 111-116onni candra saputriNo ratings yet
- Family Planning: Natural MethodDocument5 pagesFamily Planning: Natural MethodAngelaNo ratings yet
- Nur 145 (Exam Gina) : Concealed HemorrhageDocument26 pagesNur 145 (Exam Gina) : Concealed HemorrhageAntoinette PeleñaNo ratings yet
- WHO Partograph ExampleDocument1 pageWHO Partograph ExampleAlyssa DejanNo ratings yet
- Nur 146 (Rle)Document138 pagesNur 146 (Rle)Antoinette PeleñaNo ratings yet
- Municipal Health Office Municipality of Claveria, CagayanDocument2 pagesMunicipal Health Office Municipality of Claveria, CagayanSophia Kaye AguinaldoNo ratings yet
- H. Mole Case ScenarioDocument1 pageH. Mole Case ScenarioJR Rolf NeuqeletNo ratings yet
- Gordon'S Functional Health Patterns: University of San Jose - Recoletos School of Allied Medical Sciences NursingDocument2 pagesGordon'S Functional Health Patterns: University of San Jose - Recoletos School of Allied Medical Sciences NursingIvan A. EleginoNo ratings yet
- Hypnobirthing - The Mongan Method - Is A Unique Method of Relaxed, NaturalDocument3 pagesHypnobirthing - The Mongan Method - Is A Unique Method of Relaxed, NaturalZhaii Garcia MariacaNo ratings yet
- Ncma217 Lec PrelimDocument38 pagesNcma217 Lec PrelimIVY SUPNETNo ratings yet
- Aaplog Myth V FactDocument6 pagesAaplog Myth V FactWashington ExaminerNo ratings yet
- Lesson Plan of Conference PDFDocument44 pagesLesson Plan of Conference PDFRahul DamorNo ratings yet
- Embryology of The Female Genital Tract: Pranab Chatterjee Medical College, KolkataDocument31 pagesEmbryology of The Female Genital Tract: Pranab Chatterjee Medical College, KolkataPranab Chatterjee100% (4)
- PRISCA PresentationDocument42 pagesPRISCA PresentationAlexandr ChuvakovNo ratings yet
- Breech PresentationDocument27 pagesBreech PresentationHomeground entertainmentNo ratings yet
- Weebly Teaching Plan Childbirth PreparationDocument1 pageWeebly Teaching Plan Childbirth Preparationapi-272566401No ratings yet