You might also like
- Giant Cell Tumor of The Bone: Radiography, CT, MRI, and Angiography FindingsDocument7 pagesGiant Cell Tumor of The Bone: Radiography, CT, MRI, and Angiography FindingsRashif AkmalNo ratings yet
- Giant Cell-Rich Osteosarcoma: A Case ReportDocument7 pagesGiant Cell-Rich Osteosarcoma: A Case ReportRashif AkmalNo ratings yet
- Shetty 2018Document5 pagesShetty 2018Rashif AkmalNo ratings yet
- He 2019Document10 pagesHe 2019Rashif AkmalNo ratings yet
- Vanderheijden 2020Document7 pagesVanderheijden 2020Rashif AkmalNo ratings yet
- Potensial (MSC-EVS) Sebagai Terapi Terbaru Dalam Obat Iskemik RetinalDocument9 pagesPotensial (MSC-EVS) Sebagai Terapi Terbaru Dalam Obat Iskemik RetinalRashif AkmalNo ratings yet
- 10.1186@s12891 020 03569 8Document9 pages10.1186@s12891 020 03569 8Rashif AkmalNo ratings yet
- Posterior Dislocation of The Elbow With Fractures of The Radial Head and CoronoidDocument5 pagesPosterior Dislocation of The Elbow With Fractures of The Radial Head and CoronoidRashif AkmalNo ratings yet
- Infographic: Surgical Treatment of The Radial Head in Terrible Triad Injuries of The ElbowDocument2 pagesInfographic: Surgical Treatment of The Radial Head in Terrible Triad Injuries of The ElbowRashif AkmalNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
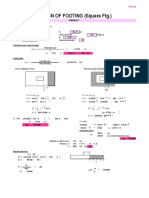
- Design of Footing (Square FTG.) : M Say, L 3.75Document2 pagesDesign of Footing (Square FTG.) : M Say, L 3.75victoriaNo ratings yet
- CreatorsXO JuneDocument9 pagesCreatorsXO JuneGaurav KarnaniNo ratings yet
- 1962 BEECHCRAFT P35 Bonanza - Specifications, Performance, Operating Cost, Valuation, BrokersDocument12 pages1962 BEECHCRAFT P35 Bonanza - Specifications, Performance, Operating Cost, Valuation, BrokersRichard LundNo ratings yet
- IllustratorDocument27 pagesIllustratorVinti MalikNo ratings yet
- SPI To I2C Using Altera MAX Series: Subscribe Send FeedbackDocument6 pagesSPI To I2C Using Altera MAX Series: Subscribe Send FeedbackVictor KnutsenbergerNo ratings yet
- Centaur Profile PDFDocument5 pagesCentaur Profile PDFChandra MohanNo ratings yet
- BCK Test Ans (Neha)Document3 pagesBCK Test Ans (Neha)Neha GargNo ratings yet
- Msds 77211 enDocument13 pagesMsds 77211 enJulius MwakaNo ratings yet
- Option - 1 Option - 2 Option - 3 Option - 4 Correct Answer MarksDocument4 pagesOption - 1 Option - 2 Option - 3 Option - 4 Correct Answer MarksKISHORE BADANANo ratings yet
- Book Shop InventoryDocument21 pagesBook Shop InventoryAli AnsariNo ratings yet
- MAYA1010 EnglishDocument30 pagesMAYA1010 EnglishjailsondelimaNo ratings yet
- Transparency in Organizing: A Performative Approach: Oana Brindusa AlbuDocument272 pagesTransparency in Organizing: A Performative Approach: Oana Brindusa AlbuPhương LêNo ratings yet
- Indian Institute of Technology (Indian School of Mines) DhabadDocument23 pagesIndian Institute of Technology (Indian School of Mines) DhabadAmit KumarNo ratings yet
- X25Document10 pagesX25RajNo ratings yet
- WHS Hazard Identification and Incident Reporting ProcedureDocument6 pagesWHS Hazard Identification and Incident Reporting ProcedureJessica SimsNo ratings yet
- Uploading, Sharing, and Image Hosting PlatformsDocument12 pagesUploading, Sharing, and Image Hosting Platformsmarry janeNo ratings yet
- Expanded Breastfeeding ActDocument9 pagesExpanded Breastfeeding ActJohn Michael CamposNo ratings yet
- 7a.simple InterestDocument50 pages7a.simple InterestJanani MaranNo ratings yet
- Samsung UDC and UEC Series Video Wall DisplaysDocument12 pagesSamsung UDC and UEC Series Video Wall DisplaysWebAntics.com Online Shopping StoreNo ratings yet
- Fixed Plug-In Motor A2Fe: Series 6Document24 pagesFixed Plug-In Motor A2Fe: Series 6Michail ArmitageNo ratings yet
- Id or Class Are SimplyDocument5 pagesId or Class Are SimplyK CorNo ratings yet
- Bill (Law) : Jump To Navigation Jump To SearchDocument9 pagesBill (Law) : Jump To Navigation Jump To SearchPunitNo ratings yet
- A Job InterviewDocument8 pagesA Job Interviewa.rodriguezmarcoNo ratings yet
- Serious Game Overview PDFDocument28 pagesSerious Game Overview PDFjuanan.peterNo ratings yet
- TDS - Total - Carter 68 - Wyh - 202201 - en - IdnDocument1 pageTDS - Total - Carter 68 - Wyh - 202201 - en - IdnAnya J PamungkasNo ratings yet
- Muster List: Vessel: M/T "Stena President" Call Sign: ZCDR6 Master: YURIY YASHINDocument9 pagesMuster List: Vessel: M/T "Stena President" Call Sign: ZCDR6 Master: YURIY YASHINwwaallNo ratings yet
- Service Bulletin: Service Bulletin NUMBER: 8.8/134A Caterpillar: Confidential Green Page 1 of 8Document8 pagesService Bulletin: Service Bulletin NUMBER: 8.8/134A Caterpillar: Confidential Green Page 1 of 8GutsavoNo ratings yet
- Arvind Textiles Internship ReportDocument107 pagesArvind Textiles Internship ReportDipan SahooNo ratings yet
- In The High Court of Delhi at New DelhiDocument3 pagesIn The High Court of Delhi at New DelhiSundaram OjhaNo ratings yet
- Gamesa Wind Turbine Element UpgradesDocument1 pageGamesa Wind Turbine Element Upgradesstanislav uzunchevNo ratings yet