Professional Documents
Culture Documents
Jco 2017 72 7362
Uploaded by
anon_769547714Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Jco 2017 72 7362
Uploaded by
anon_769547714Copyright:
Available Formats
VOLUME 35 • NUMBER 21 • JULY 20, 2017
JOURNAL OF CLINICAL ONCOLOGY R E V I E W A R T I C L E
Integrating Evidence-Based Medicine for Treatment of Spinal
Metastases Into a Decision Framework: Neurologic,
Oncologic, Mechanicals Stability, and Systemic Disease
Ori Barzilai, Ilya Laufer, Yoshiya Yamada, Daniel S. Higginson, Adam M. Schmitt, Eric Lis, and Mark H. Bilsky
Author affiliations and support information
(if applicable) appear at the end of this A B S T R A C T
article.
Patients with cancer are frequently affected by spinal metastases. Treatment is palliative, with the
Published at jco.org on June 22, 2017.
principle goals of pain relief, preservation of neurologic function, and improvement in quality of life. In
Corresponding author: Mark H. Bilsky,
the past decade, we have witnessed a dramatic change in the treatment paradigms due to the
MD, Department of Neurosurgery,
Memorial Sloan Kettering Cancer Center,
development of improved surgical strategies and systemic and radiation therapy. The most im-
1275 York Ave, New York, NY 10065; portant change to these paradigms has been the integration of spinal stereotactic radiosurgery
e-mail: bilskym@mskcc.org. (SSRS), allowing delivery of tumoricidal radiation doses with sparing of nearby organs at risk. High-
© 2017 by American Society of Clinical dose SSRS provides durable tumor control when used either as definitive therapy or as a post-
Oncology operative adjuvant therapy. Integration of SSRS has fundamentally changed the indications for and
0732-183X/17/3521w-2419w/$20.00 type of surgery performed for metastatic spine tumors. Although the role for surgical intervention is
well established, a clear trend toward less-aggressive, often minimally invasive techniques has been
observed. Targeted therapies are also rapidly changing the way cancer is being treated and have
demonstrated improved survival for a number of malignancies. As these treatment decisions
become more complex, a multidisciplinary approach including medical oncologists, radiation on-
cologists, surgeons, interventionalists, and pain specialists is required. In this article, the current
evidence affecting the treatment of spinal metastases is integrated into a decision framework that
considers four principal assessments of a patient’s spine disease: NOMS (neurologic, oncologic,
mechanical instability, and systemic disease).
J Clin Oncol 35:2419-2427. © 2017 by American Society of Clinical Oncology
ambulation, maintenance of spinal stability, du-
INTRODUCTION
rable local tumor control, and improved quality of
life. Treatment options have evolved from simple
Approximately 40% of all people with cancer decisions regarding the need for either conven-
develop spinal metastases.1,2 Almost 20% of pa- tional external beam radiation therapy (cEBRT)
tients diagnosed with spinal metastases progress or surgery to complex multimodality assessments
to symptomatic spinal cord compression. 3-5 commensurate with the development of numerous
These metastases most commonly affect the effective treatments, most importantly, spine ste-
thoracic spine (70%), followed by the lumbar reotactic radiosurgery (SSRS) and minimally in-
(20%) and cervical spine (10%).6 The com- vasive spine procedures. A decision framework,
bination of an aging population at risk for NOMS (neurologic, oncologic, mechanical instabil-
developing cancer and the widespread availability ity, and systemic disease), has been developed to
of improved diagnostic imaging, such as magnetic facilitate decision making in the evolving and
resonance and 18F-labeled fluorodeoxyglucose pos- increasingly important treatment of metastatic
itron emission tomography, have increased the scope spine tumors.
of this problem. Furthermore, targeted therapies are
extending survival for many patients with can-
cer, requiring the treatment goals for metastatic THE NOMS FRAMEWORK
spine tumors to shift from short-term palliation
to long-term durable control. The NOMS decision framework7 provides a com-
Specific treatment goals for patients with prehensive assessment of four sentinel decision
DOI: https://doi.org/10.1200/JCO.2017. spine metastases are palliative, including preser- points: neurologic, oncologic, mechanicals sta-
72.7362 vation or restoration of neurologic function and bility, and systemic disease. This framework
© 2017 by American Society of Clinical Oncology 2419
Downloaded from ascopubs.org by 182.253.63.4 on January 12, 2021 from 182.253.063.004
Copyright © 2021 American Society of Clinical Oncology. All rights reserved.
Barzilai et al
standardizes the assessment of metastatic spine tumors and allows responders (ie, radiosensitive).12,13 The remainder of the solid
for the incorporation of evidence-based medicine and the rational tumors are considered to be unfavorable responders (ie, radio-
use of new radiation, surgical, interventional radiology, and systemic resistant), including sarcoma, melanoma, renal cell, thyroid, he-
therapies (Fig 1). The neurologic assessment evaluates both clinical patocellular, colorectal, and non–small-cell lung carcinoma.9-13
and radiologic parameters, including the presence of myelopathy, Several studies confirm that patients with favorable histologies
functional radiculopathy, and the degree of epidural spinal cord are more likely to have good postradiation ambulation and remain
compression (ESCC). A validated magnetic resonance–based ESCC ambulatory longer than patients with unfavorable histologies.13,14
scoring system is used to define the extent of epidural spinal cord Katagiri et al15 found that 72% of patients with favorable histol-
compression, and patients are dichotomized into high-grade and ogies exhibited improvement in their motor strength, functional
low-grade ESCC groups (Fig 2). The oncologic consideration is ability, and pain scores, with only a 33% success rate in unfavorable
based on the expected tumoral response, principally to radiation but tumors. Maranzano et al11 showed recovery of ambulation in 67%
also to systemic therapy. The neurologic and oncologic assessments of patients with breast cancer compared with only 20% in hepa-
are combined to determine the optimal radiation strategy to achieve tocellular carcinoma. The duration of response was 10 to 16 months
tumor control and/or the need for a surgical intervention. Me- for radiosensitive tumors compared with 3 months for radioresistant
chanical instability is a separate consideration, because symptomatic tumors. It is currently accepted that regardless of the degree of ESCC,
pathologic fractures do not respond to radiation alone. Patients patients with radiosensitive tumors and no evidence of myelopathy
diagnosed with mechanical instability typically require stabilization can be treated effectively with cEBRT, obviating the need for surgical
with bone cement or spinal instrumentation. The fourth consid- intervention.9,11
eration is the extent of systemic disease and medical comorbidities
that affect the risk-benefit ratio of a proposed intervention, taking
The Role of SSRS
into account the overall expected survival and the ability of a patient
The biggest advancement in the treatment of spinal metastases
to tolerate spine-specific treatment.
has been the evolution and integration of SSRS. The introduction
of high–dose per fraction conformal radiation for use in the treatment
of patients with spinal metastases has facilitated the delivery of cy-
NEUROLOGIC AND ONCOLOGIC ASSESSMENTS totoxic tumoral doses and completely changed treatment paradigms.16
High-dose single (16 to 24 Gy) or hypofractionated (24 to 30 Gy in
The Role of cEBRT two or three fractions) SSRS offers a significantly higher biologic
Historically, spinal metastases were treated using cEBRT, effective dose and more precise dose delivery to the tumor with
commonly delivered to a total dose of 30 Gy in 10 fractions. A shorter treatment schedules compared with the cEBRT. The improved
review of the published literature demonstrates radiosensitivity tumor control with SSRS is proposed to be a result of an increased
stratifications on the basis of tumor histology.9-11 Hematologic percentage of lethal double-stranded DNA breaks, endothelial dys-
malignancies and selective solid tumors, such as seminoma, breast, function mediated through the acid sphingomyelinase pathway, and
prostate, and ovarian carcinomas, are considered to be favorable immunogenic CD8+ T cell–mediated responses.17,18 The safe and
Low-grade ESCC
Neurologic
no myelopathy
Radiation
High-grade ESCC cEBRT
± myelopathy
SRS
Oncologic
Radiosensitive
Radioresistant/ Fig 1. The neurologic, oncologic, mechani-
previously radiated cals stability and systemic disease framework.
cEBRT, conventional external beam radiation
Separation surgery
therapy; ESCC, epidural spinal cord compres-
Mechanical
Stable sion; SRS, stereotactic radiosurgery. Adapted
with permission from Laufer et al.7
Unstable Stabilization
Able to tolerate
Systemic
surgery
Unable to tolerate
surgery
2420 © 2017 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Downloaded from ascopubs.org by 182.253.63.4 on January 12, 2021 from 182.253.063.004
Copyright © 2021 American Society of Clinical Oncology. All rights reserved.
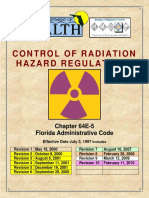
Current Decision Making for Spinal Metastases: NOMS
3
1c 2
1b
1a Fig 2. The Epidural Spinal Cord Com-
0
pression (ESCC) scale. Adapted with per-
mission from Bilsky et al.8
Schematic representation of the 6-point ESCC grading scale.
Grade 0 Bone-only disease
Grade 1a Epidural impingement, without deformation of thecal sac
Grade 1b Deformation of thecal sac, without spinal cord abutment
Grade 1c Deformation of thecal sac, with spinal cord abutment, without cord compression
Grade 2 Spinal cord compression, with CSF visible around the cord
Grade 3 Spinal cord compression, no CSF visible around the cord
effective implementation of SSRS is the result of technological as en bloc spondylectomy, to definitive oncologic treatment
advancements in patient immobilization, image guidance, inverse with radiosurgery. 29
treatment planning, and sophisticated delivery systems.19,20
Complications and Limitations
Redefining Radiosensitivity The successful application of SSRS has led to a large growth
Multiple authors have reported excellent outcomes with spine in its use and raised awareness of its potential complications.
radiosurgery for traditionally radioresistant histologies in patients Currently, major efforts are being directed at defining and pre-
with minimal or no spinal cord compression (ESCC 0 to 1c). In venting SSRS toxicity. Reported structures at risk for radiation-
a prospective trial by Garg et al,21 61 patients who had 63 tumors of associated toxicity include the spinal cord, cauda equina, skin,
the noncervical spine were enrolled and received SSRS as a first-line esophagus, peripheral nerves, paraspinal muscles, and vertebrae.
treatment in doses that ranged from 16 to 24 Gy single fraction. Fortunately, high-grade toxicity after SSRS occurs infrequently,
The actuarial 18-month imaging local control rate for all patients and most of the observed complications are mild,31 including
was 88%, and no significant differences in outcomes were noted esophagitis, mucositis, dysphagia, diarrhea, paresthesias, tran-
with respect to tumor histology.21 Guckenberger et al22 reported sient laryngitis, and radiculitis.32-37 Dose constraints have been
the results of a multi-institutional analysis of 387 patients treated established for the majority of organs at risk.38,39 Vertebral
with SBRT with 2-year local control of 84%. The cohort was compression fractures (VCFs) have recently been described after
composed of patients with various solid tumor histologies, and the SSRS, with a wide range in incidence reported, from 6% to 39%40.
median treatment dose was 24 Gy in three fractions.22 In a recent, A multi-institutional analysis found that a VCF after SSRS is more
large, single-institution experience, Yamada et al23 described a total likely to occur after treatment with high-prescription doses for
of 811 lesions treated in 657 patients with single-fraction SSRS. The a solitary spinal metastasis.41 Importantly, the majority of ra-
prescription dose ranged from 18 to 26 Gy, and, for analysis, dosing diographically observed VCFs remain asymptomatic and do not
was considered as a continuous variable. The median dose that require stabilization.40
covered 95% of the planning target volume was 16.44 Gy in the Radiation-induced spinal cord injury from SSRS is rare. One
low-dose group and 22.40 Gy in the high-dose group. Local failure multicenter publication found only six out of 1,075 cases of
rates for the low- and high-dose groups were 5% versus 0.41% at spinal radiosurgery developed radiation-induced myelopathy.42
12 months, 15% versus 1.6% at 24 months, and 20% versus 2.1% at Although institutional variability in accepted spinal cord dose
48 months, respectively. Of note, 82% of the tumors were radi- exists, one of the commonly used constraints is a cord maximum
oresistant histologies, and responses were determined to be both dose of 14 Gy.32 An analysis of 476 cervical and thoracic levels
histology and volume independent.23 SSRS yields a clinical benefit treated with single-fraction SSRS using this spinal cord constraint
regardless of histology, providing a more durable symptomatic resulted in only two patients (0.42%) developing self-limited,
response and higher local control rates than historical controls steroid-responsive myelopathy.23 However, it is this spinal cord
using cEBRT23-26 constraint that prohibits the use of SSRS in the setting of high-
A prospective randomized phase III trial is currently underway grade ESCC. In part, the rationale for this is predicated on a study
comparing cEBRT to SSRS.27 Although SSRS is still considered by by Lovelock et al,42a which demonstrated that all local failures
some to be an experimental treatment,28 the ability to deliver ab- occurred in tumors that received , 15 Gy to any portion of the
lative doses to tumor sites has fundamentally changed treat- planning target volume. Given a 10%/mm falloff of the radiation
ment paradigms,29particularly for solitary and oligometastatic dose and a cord maximum dose of 14 Gy, the tumor would either
disease30 (Fig 3). In the last several years, we have witnessed be underdosed at the margin of the spinal cord, risking epidural
a transition from treatment with aggressive cytoreductive surgeries, such progression, or overdosed, causing myelitis. Delivery of SSRS
jco.org © 2017 by American Society of Clinical Oncology 2421
Downloaded from ascopubs.org by 182.253.63.4 on January 12, 2021 from 182.253.063.004
Copyright © 2021 American Society of Clinical Oncology. All rights reserved.
Barzilai et al
Fig 3. Low-grade metastatic epidural
spinal cord compression can be effectively
treated nonoperatively with spinal ste-
reotactic radiosurgery (SSRS). A 62-year-
old woman with stage IV metastatic colon
cancer. Routine imaging work-up revealed
an L2 lesion. The patient was neurologi-
cally intact, with mild biologic back pain.
A1 A2 Spinal Instability Neoplastic Score 4 (sta-
ble). Computed tomography myelography
and magnetic resonance imaging dem-
onstrated epidural disease, Epidural Spinal
Cord Compression grade 1b. She un-
derwent up-front SSRS, treated with 24 Gy
in a single fraction (maximum dose to the
cauda, 17.60 Gy). At 3-month follow-up
there was improvement of pain and well-
controlled disease with near-complete
resolution of the epidural tumor compo-
nent. Pre- and post-SSRS imaging: (A1)
Computed tomography myelogram (mid-
sagittal) demonstrating a sclerotic L2 le-
sion; and (A2) axial cut demonstrating
the epidural component. (B1) At 2-month
follow-up, magnetic resonance T2 (mid-
sagittal); (B2) T1 with contrast enhancement
demonstrating near-complete resolution of
the epidural component. SSRS treatment
B1 B2 planning: color wash representation of
the treatment dose in (C1) axial and (C2)
sagittal views. A dose of 24 Gy (repre-
sented in orange) was prescribed to the
tumor and delivered in a single fraction.
The maximum dose delivered to the
cauda equina was 17.6 GY (outlined in
pink).
C1 C2
within the spinal cord constraints while delivering the minimal The Evolving Role of Surgery
radiation dose to the tumor volume requires a separation be- The rationale for surgery in patients with metastatic spine
tween the tumor and the spinal cord.43 Therefore, patients with tumors is largely predicated on the study by Patchell et al,45
spinal cord compression (ESCC 2 to 3) secondary to radio- which provides class 1 evidence in support of direct surgical
resistant tumors require surgical decompression of the spinal decompression for patients with solid tumor metastases resulting
cord before SSRS. Currently, the safety of SSRS in the setting of in high-grade ESCC and/or myelopathy.45 In this landmark trial,
spinal cord compression is being studied; however, an early patients randomly assigned to direct surgical decompression fol-
report indicates that a significant risk of neurologic de- lowed by cEBRT had longer overall survival, improved mainte-
terioration exists in this clinical scenario, especially in radio- nance or recovery of ambulation, better preservation of bowel and
resistant tumors. 44 bladder function, and decreased narcotic requirements compared
2422 © 2017 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Downloaded from ascopubs.org by 182.253.63.4 on January 12, 2021 from 182.253.063.004
Copyright © 2021 American Society of Clinical Oncology. All rights reserved.
Current Decision Making for Spinal Metastases: NOMS
with cEBRT alone. On the basis of this and a number of other surgery followed by SSRS in a retrospective review of 186 patients
series, the Spine Oncology Study Group, in a systematic literature and found the strategy to be both safe and effective for establishing
review, made a strong recommendation for surgical stabilization durable local tumor control regardless of tumor histology–specific
followed by decompression in patients with radioresistant tumors radiosensitivity. In this series, the three SSRS dose strategies used
in the setting of high-grade compression.29 were single fraction (24 Gy), high-dose hypofractionated (24 to
The integration of SSRS as postoperative adjuvant therapy has 30 Gy in three fractions), or low-dose hypofractionated (18 to
fundamentally changed the goals of surgery and significantly de- 36 Gy in five to six fractions). Overall, the 1-year local rate of
creased the associated morbidity compared with techniques tra- progression was 16.4%. The only significant factor affecting local
ditionally used with cEBRT. Patients with high-grade ESCC from tumor progression was the SSRS dose when comparing high-dose
radioresistant tumors require spinal cord decompression for hypofractionated versus low-dose hypofractionated, 4% versus
neurologic salvage and instrumented fusions for spinal stabiliza- 22%, respectively.47 The 24-Gy single-fraction cohort had a 9% risk
tion; however, the paradigm shift in surgery is reflected in the of progression. There was no impact of tumor histology, prior
extent of tumor resection (Fig 4). Using cEBRT, surgeons pre- failed radiation, or the degree of preoperative epidural compres-
viously relied on invasive procedures to achieve maximal cytor- sion on recurrence rates, and no patient suffered a neurologic
eduction. Despite this aggressive surgery, local recurrence rates complication. Rock et al48 also reported a 92% local-control rate in
were on the order of 60% at 6 months and 96% at 4 years.46 With 18 patients treated with radiosurgery after open surgical pro-
the use of SSRS, the surgical goal became simply to create a target cedures, and similar results have been demonstrated in other
for the safe delivery of SSRS. The term separation surgery was smaller series.49 Al-Omair et al50 noted that patients with post-
coined to describe a posterolateral epidural decompression with operative scans that showed continued compression of the spinal
posterior instrumented fusion that focused on reconstitution of cord (ie, ESCC 2 to 3) had a significantly higher risk of local
spinal fluid space to create a 2-mm margin between the tumor and recurrence after postoperative SSRS compared with patients with
spinal cord, but without resection of the vertebral body or para- sufficient separation between the tumor and the spinal cord (ie,
spinal tumor. Laufer et al47 evaluated the efficacy of separation ESCC 0 to 1c). Furthermore, patients with circumferential spinal
Fig 4. Separation surgery with spinal
stereotactic radiosurgery (SSRS) has replaced
more extensive surgeries, such as complete
vertebrectomies in selected patients. A 76-
year-old man with renal cell carcinoma pre-
sented with severe back pain and no signs of
myelopathy. Evaluation including spinal imag-
ing demonstrated a T4 tumor with high-grade
(ie, Epidural Spinal Cord Compression grade 3)
cord compression. Preoperative tumor
embolization was followed by separation
surgery (ie, posterolateral decompression
with pedicle screw fixation). Note the left rib
and vertebral body tumor were not resec-
ted. Postoperatively, the patient remained
neurologically intact and subsequently un-
derwent hypofractionated stereotactic ra-
A B1 B2 diosurgery (27 Gy in three fractions) with
well-controlled disease at long-term follow-
up. Pre- and postoperative sagittal imag-
ing: (A) Preoperative magnetic resonance
imaging T2 demonstrating a T4 tumor. (B1)
Postoperative computed tomography
myelography demonstrating the surgical
and reconstituted thecal sac. (B2) upright
x-ray representing the stabilizing construct.
Pre- and postoperative axial imaging: (C)
Preoperative magnetic resonance imaging
T1 with contrast enhancement. (D) Post-
operative computed tomography myelog-
raphy. Note the high-grade cord compression
preoperatively and the CSF-filled thecal sac
and stabilizing construct postoperatively.
This new distance between the tumor and
the spinal cord allows for safe concurrent
radiosurgical treatment.
C D
jco.org © 2017 by American Society of Clinical Oncology 2423
Downloaded from ascopubs.org by 182.253.63.4 on January 12, 2021 from 182.253.063.004
Copyright © 2021 American Society of Clinical Oncology. All rights reserved.
Barzilai et al
cord compression represent challenging postoperative SSRS tar- treated with stabilization procedures, such as percutaneous cement
gets51 and may benefit from intraoperative brachytherapy using augmentation, pedicle screw fixation, or open surgery (Fig 5). The
32 52
P. Intraoperative brachytherapy facilitates improved post- Cancer Patient Fracture Evaluation (CAFE) trial provided prospective
operative SSRS dosimetry in patients with circumferential tumors randomized data showing significant pain reduction and improve-
of the spine.53 ment in disability indexes that persist for up to 6 months when
kyphoplasty was performed compared with the noninterventional
control arm.55
MECHANICAL INSTABILITY Spinal instability is an independent indication for an inter-
ventional procedure regardless of the radiosensitivity of the tumor or
Mechanical instability serves as an independent surgical indication degree of spinal cord compression. The suspicion of instability
regardless of the neurologic or oncologic assessment. Spinal in- should facilitate referral for early surgical evaluation and the ra-
stability, as defined by the Spine Oncology Study Group, is the “loss tionale for routine multidisciplinary evaluation of spine metastases.
of spinal integrity as a result of a neoplastic process that is asso-
ciated with movement-related pain, symptomatic or progressive de-
formity, and/or neural compromise under physiologic loads.”54(pE1226) SYSTEMIC DISEASE AND MEDICAL COMORBIDITIES
The Spinal Instability Neoplastic Score (SINS) was developed to
facilitate the assessment and communication of mechanical sta- Once the decision has been made regarding treatment on the basis
bility.54 SINS incorporates both clinical and radiologic factors of assessments of neurologic, oncologic, and mechanical stability,
important for maintenance of spinal integrity and includes tumors the remaining question is whether the patient can tolerate the
location, pain, alignment, lesion character (ie, osteolysis), vertebral proposed procedure and whether it makes sense in the clinical
body collapse, and posterior element involvement (Table 1). Be- context. Extent of disease, medical comorbidities, and expected
cause pain is one of the primary determinants of spinal instability, survival all play a critical role in this assessment. Patients most
differentiating biologic from mechanical pain is crucial for treating often undergo magnetic resonance imaging of the entire spinal axis
oncologists. Biologic pain increases in severity at night, abates with and histology-specific staging. Medical work-up should be directed
glucocorticoid administration, and is not exacerbated by move- toward known patient comorbidities but often includes pulmonary
ment. Mechanical pain is generally relieved with rest, exacerbated function tests, Doppler ultrasounds, and echocardiogram.
by movement, and does not respond to glucocorticoid administration. Several scoring systems, such as the Tokuhashi revised score,56 the
Oncolytic therapy reduces biologic pain, whereas mechanical pain is Tomita score,57 and the Bauer modified score,58,59 have been developed
to estimate expected survival in patients with spinal metastases. The
accuracy of these scores has been questioned, and along with the
Table 1. The Spinal Instability Neoplastic Score54
current change in survival, the reliability of these methods remains
uncertain.60,61 Currently, the ability of molecular markers to provide
Spinal Instability Neoplastic Score Component Score
prognostic information is changing cancer treatment schemes. Because
Location
treatment in this population serves a palliative purpose, physicians
Junctional (occiput-C2, C7-T2, T11-L1, L5-S1) 3
Mobile spine (C3-C6, L2-L4) 2 should focus on whether the patients are likely to adequately recover
Semirigid (T3-T10) 1 from the indicated procedure and become candidates for systemic
Rigid (S2-S5) 0 therapy. The minimally invasive nature of procedures such as per-
Pain
Yes 3
cutaneous cement augmentation or pedicle screw fixation can dra-
Occasional pain but not mechanical 1 matically improve quality of life even in patients with limited survival.
Pain-free lesion 0 The prevention, diagnosis, treatment, and general manage-
Bone lesion ment of cancer have recently been influenced by major scientific
Lytic 2
Mixed (lytic/blastic) 1
advances. Modern technologies allow for the assessment of ge-
Blastic 0 nomic and proteomic alterations and epigenetic and posttranslational
Radiographic spinal alignment modifications at the molecular level.62 The understanding of how
Subluxation/translation present 4 these influence tumors of the spine is ongoing, and interest is
De novo deformity (kyphosis/scoliosis) 2
Normal alignment 0 growing, predominantly for metastatic melanoma.63,64
Vertebral body collapse Generally, systemic therapy is considered to be more effec-
. 50% collapse 3 tive for visceral than for osseous disease, yet it may still play a
, 50% collapse 2
significant role in the treatment of spine metastases, particularly
No collapse with . 50% body involved 1
None of the above 0 when combined with stereotactic radiosurgery (SRS). One strategy
Posterolateral involvement of spinal elements that has demonstrated promising results is the combination of SRS
Bilateral 3 with checkpoint inhibitors inducing the abscopal effect and po-
Unilateral 1
None of the above 0
tentiating the effects of local radiation. This immune-mediated
Total score effect of SRS with checkpoint inhibitors has been demonstrated in
Stable 0-6 murine models65 and is believed to be associated with both
Indeterminate 7-12 hypofractionated and high-dose single-fraction radiation therapy66
Unstable 13-18
but suppressed with conventionally fractionated radiotherapy.67
Postow et al68 reported the abscopal effect in a patient with
2424 © 2017 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Downloaded from ascopubs.org by 182.253.63.4 on January 12, 2021 from 182.253.063.004
Copyright © 2021 American Society of Clinical Oncology. All rights reserved.
Current Decision Making for Spinal Metastases: NOMS
Fig 5. Mechanical instability should be
addressed with stabilization. A 66-year-old
woman with newly diagnosed multiple
osseous lesions and lung lesion. She
presented with severe mechanical back
pain with a visual analog score of 9. She
underwent imaging including a chest-
abdomen-pelvis computed tomography
scan, bone scan, and full spinal axis
magnetic resonance imaging (MRI). Im-
aging demonstrated a left lung nodule,
lytic disease at T10, and sclerotic bone
disease at T6. The T10 lesion had a Spinal
Instability Neoplastic Score of 14 but
without spinal cord compression. Given
the presence of mechanical instability, the
patient underwent T9-T11 percutaneous
A B pedicle screw stabilization with cement-
augmented screws and kyphoplasty at
T10. Needle biopsy obtained during the
kyphoplasty revealed non–small-cell lung
carcinoma. The patient received 24 single-
fraction spinal stereotactic radiosurgery.
She is currently 6 months post spinal
stereotactic radiosurgery with well-
controlled disease, visual analog score
of 1, and neurologically intact. Pre- and
postoperative imaging: (A) Preoperative
sagittal MRI (T1 without contrast en-
hancement) demonstrating the T6 and T10
lesions. (B) Axial T2 MRI at T10 level
demonstrating epidural spinal cord com-
pression. (C) Postoperative sagittal x-ray
with the stabilizing construct and kypho-
plasty. (D) Postoperative anterior-posterior
x-ray with the stabilizing construct and
kyphoplasty.
C D
melanoma receiving ipilimumab who received high-dose hypo- also for spinal stabilization as facilitated by SINS. The role for
fractionated radiation to a paraspinal lesion with subsequent res- less-invasive surgical options such as separation surgery and
olution of multiple lung lesions and a 30-fold increase in the titer of percutaneous stabilization followed by SSRS is growing. These
antibodies to a melanoma epitope. Harnessing the abscopal effect techniques are largely replacing highly morbid surgical approaches,
may lead to treatment strategies in which local radiation can sig- such as en bloc spondylectomy or transcavitary vertebrectomy.
nificantly affect systemic disease control. In addition, vascular Targeted therapies are, at present, redefining cancer treatment, yet
endothelial growth factor has been shown to inhibit the acid their precise role for spinal tumors is yet to be fully determined.
sphingomyelinase pathway that leads to endothelial dysfunction.
Experimental murine models have demonstrated that axitinib, an oral
tyrosine kinase inhibitor–vascular endothelial growth factor inhibitor, AUTHORS’ DISCLOSURES OF POTENTIAL CONFLICTS
in combination with SRS, can derepress this pathway, potentially OF INTEREST
acting as a radiosensitizer.69 From a spine tumor perspective, the
understanding of the effect of these therapies is premature, and as data Disclosures provided by the authors are available with this article at
accumulate it is likely to continue evolving treatment strategies. jco.org.
In conclusion, optimal management of spinal metastases
requires a multidisciplinary team effort. The NOMS framework
provides an algorithm for consistent and up-to-date management AUTHOR CONTRIBUTIONS
that is highly reproducible. The integration of radiosurgery has
completely evolved the way this patient population is being treated, Conception and design: Ori Barzilai, Mark H. Bilsky
Collection and assembly of data: Ori Barzilai, Mark H. Bilsky
and overcoming radioresistance has provided a giant leap in the Data analysis and interpretation: All authors
ability to control these tumors. Surgery still plays a key role in this Manuscript writing: All authors
paradigm, particularly for those with high-grade ESCC, necessi- Final approval of manuscript: All authors
tating separation of the epidural tumor from the spinal cord, but Accountable for all aspects of the work: All authors
jco.org © 2017 by American Society of Clinical Oncology 2425
Downloaded from ascopubs.org by 182.253.63.4 on January 12, 2021 from 182.253.063.004
Copyright © 2021 American Society of Clinical Oncology. All rights reserved.
Barzilai et al
20. Chang BK, Timmerman RD: Stereotactic body 39. Sahgal A, Weinberg V, Ma L, et al: Probabilities
REFERENCES radiation therapy: A comprehensive review. Am J of radiation myelopathy specific to stereotactic body
Clin Oncol 30:637-644, 2007 radiation therapy to guide safe practice. Int J Radiat
1. Cobb CA III, Leavens ME, Eckles N: In- 21. Garg AK, Shiu AS, Yang J, et al: Phase 1/2 trial Oncol Biol Phys 85:341-347, 2013
dications for nonoperative treatment of spinal cord of single-session stereotactic body radiotherapy for 40. Virk MS, Han JE, Reiner AS, et al: Frequency
compression due to breast cancer. J Neurosurg 47: previously unirradiated spinal metastases. Cancer of symptomatic vertebral body compression frac-
653-658, 1977 118:5069-5077, 2012 tures requiring intervention following single-fraction
2. Wong DA, Fornasier VL, MacNab I: Spinal 22. Guckenberger M, Mantel F, Gerszten PC, et al: stereotactic radiosurgery for spinal metastases.
metastases: The obvious, the occult, and the im- Safety and efficacy of stereotactic body radiotherapy Neurosurg Focus 42:E8, 2017
postors. Spine 15:1-4, 1990 as primary treatment for vertebral metastases: A 41. Jawad MS, Fahim DK, Gerszten PC, et al:
3. Klimo P Jr, Schmidt MH: Surgical manage- multi-institutional analysis. Radiat Oncol 9:226, 2014 Vertebral compression fractures after stereotactic
ment of spinal metastases. Oncologist 9:188-196, 23. Yamada Y, Katsoulakis E, Laufer I, et al: The body radiation therapy: A large, multi-institutional,
2004 impact of histology and delivered dose on local multinational evaluation. J Neurosurg Spine 24:
4. North RB, LaRocca VR, Schwartz J, et al: control of spinal metastases treated with stereotactic 928-936, 2016
Surgical management of spinal metastases: Analysis radiosurgery. Neurosurg Focus 42:E6, 2017 42. Gibbs IC, Patil C, Gerszten PC, et al: Delayed
of prognostic factors during a 10-year experience. 24. Gerszten PC, Burton SA, Ozhasoglu C, et al: radiation-induced myelopathy after spinal radio-
J Neurosurg Spine 2:564-573, 2005 Radiosurgery for spinal metastases: Clinical experi- surgery. Neurosurgery 64:A67-A72, 2009 (suppl 2)
5. Sinson GP, Zager EL: Metastases and spinal ence in 500 cases from a single institution. Spine 32: 42a. Lovelock DM, Zhang Z, Jackson A, et al:
cord compression. N Engl J Med 327:1953-1955 193-199, 2007 Correlation of local failure with measures of dose
1992 25. Ghia AJ, Chang EL, Bishop AJ, et al: Single- insufficiency in the high-dose single-fraction treat-
6. Sciubba DM, Petteys RJ, Dekutoski MB, et al: fraction versus multifraction spinal stereotactic ment of bony metastases. Int J Radiat Oncol Biol
Diagnosis and management of metastatic spine radiosurgery for spinal metastases from renal cell Phys 77:1282-7, 2010
disease. A review. J Neurosurg Spine 13:94-108, carcinoma: Secondary analysis of Phase I/II trials. 43. Joaquim AF, Powers A, Laufer I, et al: An
2010 J Neurosurg Spine 24:829-836, 2016 update in the management of spinal metastases. Arq
26. Miller JA, Balagamwala EH, Angelov L, et al:
7. Laufer I, Rubin DG, Lis E, et al: The NOMS Neuropsiquiatr 73:795-802, 2015
Stereotactic radiosurgery for the treatment of primary 44. Ryu S, Rock J, Jain R, et al: Radiosurgical
framework: Approach to the treatment of spinal
and metastatic spinal sarcomas. Technol Cancer Res decompression of metastatic epidural compression.
metastatic tumors. Oncologist 18:744-751, 2013
Treat 16:276-284, 2017
8. Bilsky MH, Laufer I, Fourney DR, et al: Re- Cancer 116:2250-2257, 2010
27. Ryu S, Pugh SL, Gerszten PC, et al: RTOG
liability analysis of the epidural spinal cord com- 45. Patchell RA, Tibbs PA, Regine WF, et al: Direct
0631 phase 2/3 study of image guided stereotactic
pression scale. J Neurosurg Spine 13:324-328, 2010 decompressive surgical resection in the treatment of
radiosurgery for localized (1-3) spine metastases:
9. Gerszten PC, Mendel E, Yamada Y: Radio- spinal cord compression caused by metastatic can-
Phase 2 results. Pract Radiat Oncol 4:76-81, 2014
therapy and radiosurgery for metastatic spine disease: cer: A randomised trial. Lancet 366:643-648, 2005
28. Lutz S, Balboni T, Jones J, et al: Palliative
What are the options, indications, and outcomes? 46. Klekamp J, Samii H: Surgical results for spinal
radiation therapy for bone metastases: Update of an
Spine 34:S78-S92, 2009 (suppl 22) metastases. Acta Neurochir (Wien) 140:957-967,
ASTRO Evidence-Based Guideline. Pract Radiat
10. Mizumoto M, Harada H, Asakura H, et al: 1998
Oncol 7:4-12, 2017
Radiotherapy for patients with metastases to the 47. Laufer I, Iorgulescu JB, Chapman T, et al:
29. Bilsky MH, Laufer I, Burch S: Shifting para-
spinal column: A review of 603 patients at Shizuoka Local disease control for spinal metastases following
digms in the treatment of metastatic spine disease.
Cancer Center Hospital. Int J Radiat Oncol Biol Phys “separation surgery” and adjuvant hypofractionated
Spine 34:S101-S107, 2009 (suppl 22)
79:208-213, 2011 or high-dose single-fraction stereotactic radiosurgery:
30. Ho JC, Tang C, Deegan BJ, et al: The use of
11. Maranzano E, Latini P: Effectiveness of radi- outcome analysis in 186 patients. J Neurosurg Spine
spine stereotactic radiosurgery for oligometastatic
ation therapy without surgery in metastatic spinal 18:207-214, 2013
disease. J Neurosurg Spine 25:239-247, 2016
cord compression: Final results from a prospective
31. Moussazadeh N, Lis E, Katsoulakis E, et al: 48. Rock JP, Ryu S, Shukairy MS, et al: Post-
trial. Int J Radiat Oncol Biol Phys 32:959-967, 1995 operative radiosurgery for malignant spinal tumors.
Five-year outcomes of high-dose single-fraction spi-
12. Rades D, Fehlauer F, Stalpers LJ, et al: A nal stereotactic radiosurgery. Int J Radiat Oncol Biol Neurosurgery 58:891-898, 2006; discussion 891-898
prospective evaluation of two radiotherapy sched- Phys 93:361-367, 2015 49. Bate BG, Khan NR, Kimball BY, et al: Stereo-
ules with 10 versus 20 fractions for the treatment of 32. Yamada Y, Bilsky MH, Lovelock DM, et al: tactic radiosurgery for spinal metastases with or
metastatic spinal cord compression: Final results of High-dose, single-fraction image-guided intensity- without separation surgery. J Neurosurg Spine 22:
a multicenter study. Cancer 101:2687-2692, 2004 modulated radiotherapy for metastatic spinal le- 409-415, 2015
13. Rades D, Fehlauer F, Schulte R, et al: Prog- sions. Int J Radiat Oncol Biol Phys 71:484-490, 2008 50. Al-Omair A, Masucci L, Masson-Cote L, et al:
nostic factors for local control and survival after ra- 33. Benzil DL, Saboori M, Mogilner AY, et al: Surgical resection of epidural disease improves local
diotherapy of metastatic spinal cord compression. Safety and efficacy of stereotactic radiosurgery for control following postoperative spine stereotactic
J Clin Oncol 24:3388-3393, 2006 tumors of the spine. J Neurosurg 101:413-418, 2004 body radiotherapy. Neuro-oncol 15:1413-1419, 2013
14. Gilbert RW, Kim JH, Posner JB: Epidural spinal (suppl 3) 51. Chan MW, Thibault I, Atenafu EG, et al: Pat-
cord compression from metastatic tumor: Diagnosis 34. Degen JW, Gagnon GJ, Voyadzis JM, et al: terns of epidural progression following postoperative
and treatment. Ann Neurol 3:40-51, 1978 CyberKnife stereotactic radiosurgical treatment of spine stereotactic body radiotherapy: Implications for
15. Katagiri H, Takahashi M, Inagaki J, et al: spinal tumors for pain control and quality of life. clinical target volume delineation. J Neurosurg Spine
Clinical results of nonsurgical treatment for spinal J Neurosurg Spine 2:540-549, 2005 24:652-659, 2016
metastases. Int J Radiat Oncol Biol Phys 42: 35. Chang EL, Shiu AS, Mendel E, et al: Phase I/II 52. Folkert MR, Bilsky MH, Cohen GN, et al:
1127-1132, 1998 study of stereotactic body radiotherapy for spinal Intraoperative 32P high-dose rate brachytherapy of
16. Chan NK, Abdullah KG, Lubelski D, et al: metastasis and its pattern of failure. J Neurosurg the dura for recurrent primary and metastatic in-
Stereotactic radiosurgery for metastatic spine tu- Spine 7:151-160, 2007 tracranial and spinal tumors. Neurosurgery 71:1003-
mors. J Neurosurg Sci 58:37-44, 2014 36. Hamilton AJ, Lulu BA: A prototype device for 1010, 2012; discussion 1010-1011
17. Garcia-Barros M, Paris F, Cordon-Cardo C, linear accelerator-based extracranial radiosurgery. 53. Folkert MR, Bilsky MH, Cohen GN, et al: Local
et al: Tumor response to radiotherapy regulated by Acta Neurochir Suppl (Wien) 63:40-43, 1995 recurrence outcomes using the 32P intraoperative
endothelial cell apoptosis. Science 300:1155-1159, 37. Cox BW, Jackson A, Hunt M, et al: Esophageal brachytherapy plaque in the management of malig-
2003 toxicity from high-dose, single-fraction paraspinal nant lesions of the spine involving the dura. Bra-
18. Vignard J, Mirey G, Salles B: Ionizing-radiation stereotactic radiosurgery. Int J Radiat Oncol Biol chytherapy 14:202-208, 2015
induced DNA double-strand breaks: A direct and in- Phys 83:e661-e667, 2012 54. Fisher CG, DiPaola CP, Ryken TC, et al: A novel
direct lighting up. Radiother Oncol 108:362-369, 2013 38. Schipani S, Wen W, Jin JY, et al: Spine radi- classification system for spinal instability in neo-
19. Alongi F, Arcangeli S, Filippi AR, et al: Review osurgery: A dosimetric analysis in 124 patients who plastic disease: An evidence-based approach and
and uses of stereotactic body radiation therapy for received 18 Gy. Int J Radiat Oncol Biol Phys 84: expert consensus from the Spine Oncology Study
oligometastases. Oncologist 17:1100-1107, 2012 e571-e576, 2012 Group. Spine 35:E1221-E1229, 2010
2426 © 2017 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Downloaded from ascopubs.org by 182.253.63.4 on January 12, 2021 from 182.253.063.004
Copyright © 2021 American Society of Clinical Oncology. All rights reserved.
Current Decision Making for Spinal Metastases: NOMS
55. Berenson J, Pflugmacher R, Jarzem P, et al: 60. Dardic M, Wibmer C, Berghold A, et al: Eval- 65. Demaria S, Bhardwaj N, McBride WH, et al:
Balloon kyphoplasty versus non-surgical fracture uation of prognostic scoring systems for spinal me- Combining radiotherapy and immunotherapy: A re-
management for treatment of painful vertebral body tastases in 196 patients treated during 2005-2010. vived partnership. Int J Radiat Oncol Biol Phys 63:
compression fractures in patients with cancer: A Eur Spine J 24:2133-2141, 2015 655-666, 2005
multicentre, randomised controlled trial. Lancet Oncol 61. Zoccali C, Skoch J, Walter CM, et al: The 66. Dewan MZ, Galloway AE, Kawashima N, et al:
12:225-235, 2011 Tokuhashi score: effectiveness and pitfalls. Eur Spine Fractionated but not single-dose radiotherapy in-
56. Tokuhashi Y, Matsuzaki H, Oda H, et al: A J 25:673-678, 2016 duces an immune-mediated abscopal effect when
revised scoring system for preoperative evalua- 62. Goodwin CR, Abu-Bonsrah N, Bilsky MH, et al: combined with anti-CTLA-4 antibody. Clin Cancer
tion of metastatic spine tumor prognosis. Spine 30: Clinical decision making: Integrating advances in the Res 15:5379-5388, 2009
2186-2191, 2005 molecular understanding of spine tumors. Spine 41: 67. Filatenkov A, Baker J, Mueller AM, et al: Ab-
57. Tomita K, Kawahara N, Kobayashi T, et al: S171-S177, 2016 (suppl 20) lative tumor radiation can change the tumor immune
Surgical strategy for spinal metastases. Spine 26: 63. Caruso JP, Cohen-Inbar O, Bilsky MH, et al: cell microenvironment to induce durable complete
298-306, 2001 Stereotactic radiosurgery and immunotherapy for remissions. Clin Cancer Res 21:3727-3739, 2015
58. Bauer HC, Wedin R: Survival after surgery for metastatic spinal melanoma. Neurosurg Focus 38: 68. Postow MA, Callahan MK, Barker CA, et al:
spinal and extremity metastases. Prognostication in E6, 2015 Immunologic correlates of the abscopal effect in a pa-
241 patients. Acta Orthop Scand 66:143-146, 1995 64. Shankar GM, Choi BD, Grannan BL, et al: Ef- tient with melanoma. N Engl J Med 366:925-931, 2012
59. Leithner A, Radl R, Gruber G, et al: Predictive fect of immunotherapy status on outcomes in pa- 69. Miller JA, Balagamwala EH, Angelov L, et al:
value of seven preoperative prognostic scoring sys- tients with metastatic melanoma to the spine. Spine Spine stereotactic radiosurgery with concurrent ty-
tems for spinal metastases. Eur Spine J 17:1488-1495, (Phila Pa 1976) 10.1097/BRS.0000000000001993 rosine kinase inhibitors for metastatic renal cell car-
2008 [epub ahead of print on November 22, 2016] cinoma. J Neurosurg Spine 25:766-774, 2016
Affiliations
Ori Barzilai, Ilya Laufer, Yoshiya Yamada, Daniel S. Higginson, Adam M. Schmitt, Eric Lis, and Mark H. Bilsky, Memorial Sloan
Kettering Cancer Center; Ilya Laufer and Mark H. Bilsky, Weill Cornell Medical College, New York, NY.
nnn
jco.org © 2017 by American Society of Clinical Oncology 2427
Downloaded from ascopubs.org by 182.253.63.4 on January 12, 2021 from 182.253.063.004
Copyright © 2021 American Society of Clinical Oncology. All rights reserved.
Barzilai et al
AUTHORS’ DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST
Integrating Evidence-Based Medicine for Treatment of Spinal Metastases Into a Decision Framework: Neurologic, Oncologic, Mechanicals Stability,
and Systemic Disease
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated. Relationships are
self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more
information about ASCO’s conflict of interest policy, please refer to www.asco.org/rwc or ascopubs.org/jco/site/ifc.
Ori Barzilai Adam M. Schmitt
No relationship to disclose No relationship to disclose
Ilya Laufer Eric Lis
Consulting or Advisory Role: DePuy Synthes Companies, Globus Consulting or Advisory Role: Medtronic
Medical, Spine Wave, Brainlab, Medtronic Speakers’ Bureau: Medtronic
Yoshiya Yamada Mark H. Bilsky
Consulting or Advisory Role: Varian Medical Systems, Chordoma Honoraria: Globus Medical
Foundation Consulting or Advisory Role: Varian Medical Systems
Speakers’ Bureau: Institute for Medical Education Patents, Royalties, Other Intellectual Property: DePuy Synthes Spine,
Travel, Accommodations, Expenses: National Cancer Center Malaysia Globus Medical
Travel, Accommodations, Expenses: Globus Medical
Daniel S. Higginson
No relationship to disclose
© 2017 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Downloaded from ascopubs.org by 182.253.63.4 on January 12, 2021 from 182.253.063.004
Copyright © 2021 American Society of Clinical Oncology. All rights reserved.
You might also like
- Comprehensive Surgical Treatment Strategy For Spinal MetastasesDocument11 pagesComprehensive Surgical Treatment Strategy For Spinal MetastasessukiyantoNo ratings yet
- Radiotherapy and OncologyDocument14 pagesRadiotherapy and OncologyJavier RodríguezNo ratings yet
- Metastatic Spine Disease: A Guide to Diagnosis and ManagementFrom EverandMetastatic Spine Disease: A Guide to Diagnosis and ManagementRex A. W. MarcoNo ratings yet
- Advanced Magnetic Resonance Imaging in Glioblastoma A ReviewDocument12 pagesAdvanced Magnetic Resonance Imaging in Glioblastoma A Reviewafdhal.888980No ratings yet
- Metastatic Spinal Tumor: Chong-Suh Lee, MDDocument17 pagesMetastatic Spinal Tumor: Chong-Suh Lee, MDMarlin Berliannanda TawayNo ratings yet
- Enneking Stadializare OS MSKDocument15 pagesEnneking Stadializare OS MSKVlad RakoczyNo ratings yet
- LWBK836 Ch137 p1485-1486Document2 pagesLWBK836 Ch137 p1485-1486metasoniko81No ratings yet
- ZJ 4852Document10 pagesZJ 4852Christopher BermeoNo ratings yet
- Metastase Cerebrale 2Document19 pagesMetastase Cerebrale 2Nouhad BenNo ratings yet
- Kapoor SchwannomaDocument7 pagesKapoor SchwannomaAna Clara Nunes SartoriNo ratings yet
- (Journal of Neurosurgery - Spine) Need For Arthrodesis Following Facetectomy For Spinal Peripheral Nerve Sheath Tumors - An Institutional Experience and Review of The Current LiteratureDocument146 pages(Journal of Neurosurgery - Spine) Need For Arthrodesis Following Facetectomy For Spinal Peripheral Nerve Sheath Tumors - An Institutional Experience and Review of The Current LiteratureMohammed Ali AlviNo ratings yet
- Stereotactic Body Radiation Therapy For Spinal Metas - 2023 - Seminars in RadiatDocument13 pagesStereotactic Body Radiation Therapy For Spinal Metas - 2023 - Seminars in Radiate paperNo ratings yet
- Nanda 2016Document15 pagesNanda 2016Novia AyuNo ratings yet
- New Horizons in The Treatment of Osteosarcoma: Review ArticleDocument11 pagesNew Horizons in The Treatment of Osteosarcoma: Review ArticleRucelia Michiko PiriNo ratings yet
- Vestibular SchwanomaDocument10 pagesVestibular SchwanomaUsman Agus PrasetyoNo ratings yet
- Spinal Tumor Surgery: A Case-Based ApproachFrom EverandSpinal Tumor Surgery: A Case-Based ApproachDaniel M. SciubbaNo ratings yet
- DefaultDocument46 pagesDefaultNairo CanoNo ratings yet
- Target Volume Delineation for Pediatric CancersFrom EverandTarget Volume Delineation for Pediatric CancersStephanie A. TerezakisNo ratings yet
- (10920684 - Neurosurgical Focus) Decompression Surgery For Spinal Metastases - A Systematic ReviewDocument35 pages(10920684 - Neurosurgical Focus) Decompression Surgery For Spinal Metastases - A Systematic ReviewsukiyantoNo ratings yet
- Payer 2015Document10 pagesPayer 2015esinsubozatliNo ratings yet
- Bacciu 2013Document10 pagesBacciu 2013AshokNo ratings yet
- Fifty Years of Bone TumorsDocument7 pagesFifty Years of Bone TumorsOstazNo ratings yet
- Who Are The Best Candidates For DecompressiveDocument8 pagesWho Are The Best Candidates For DecompressiverecolenciNo ratings yet
- Imaging Updates To Breast Cancer Lymph Node ManagementDocument17 pagesImaging Updates To Breast Cancer Lymph Node ManagementMinh Thư DươngNo ratings yet
- Wilson 2017Document13 pagesWilson 2017DaniNo ratings yet
- Brain Metastasis TreatmentDocument28 pagesBrain Metastasis TreatmentMonica AngNo ratings yet
- TMP 33 BFDocument6 pagesTMP 33 BFFrontiersNo ratings yet
- JurnalDocument10 pagesJurnalAde MayashitaNo ratings yet
- Choi 2021Document12 pagesChoi 2021paul_androideNo ratings yet
- Radiation Therapy-Guidelines For PhysiotherapistsDocument9 pagesRadiation Therapy-Guidelines For PhysiotherapistsSofia Adão da FonsecaNo ratings yet
- Management of Atypical Cranial Meningiomas Part 2Document8 pagesManagement of Atypical Cranial Meningiomas Part 2Edie DelgadoNo ratings yet
- A Case Report of Chest Wall Desmoplastic Sma - 2024 - International Journal of SDocument4 pagesA Case Report of Chest Wall Desmoplastic Sma - 2024 - International Journal of SRonald QuezadaNo ratings yet
- A Volume Matched Comparison of Survival After Radiosurgery in Non Small Cell Lung Cancer Patients With One Versus More Than Twenty Brain MetastasesDocument7 pagesA Volume Matched Comparison of Survival After Radiosurgery in Non Small Cell Lung Cancer Patients With One Versus More Than Twenty Brain MetastasesPablo Castro PenaNo ratings yet
- Malignant Bone Tumors - Sparing Vs AmpDocument13 pagesMalignant Bone Tumors - Sparing Vs AmpAnonymous wJTlxhINo ratings yet
- MainDocument8 pagesMainIoana CucuNo ratings yet
- Brain Metastases Management, A ReviewDocument10 pagesBrain Metastases Management, A ReviewVita Kusuma RahmawatiNo ratings yet
- Capture D'écran . 2022-07-11 À 10.45.43 P.M.Document10 pagesCapture D'écran . 2022-07-11 À 10.45.43 P.M.universeloNo ratings yet
- Management of Metastatic Spinal Cord Compression: Southern Medical Journal September 2017Document9 pagesManagement of Metastatic Spinal Cord Compression: Southern Medical Journal September 2017Rudy Arindra WijayaNo ratings yet
- Systemic Therapy For Advanced Appendiceal Adenocarcinoma: An Analysis From The NCCN Oncology Outcomes Database For Colorectal CancerDocument8 pagesSystemic Therapy For Advanced Appendiceal Adenocarcinoma: An Analysis From The NCCN Oncology Outcomes Database For Colorectal Canceralberto cabelloNo ratings yet
- Surgical Management of Primary and Metastatic Spinal TumorsDocument7 pagesSurgical Management of Primary and Metastatic Spinal TumorskikyfauziasuryaNo ratings yet
- Complications After Thigh Sarcoma ResectionDocument7 pagesComplications After Thigh Sarcoma ResectionElaine IllescasNo ratings yet
- Management of Single Brain Metastasis: A Practice GuidelineDocument13 pagesManagement of Single Brain Metastasis: A Practice GuidelineAndreea IduNo ratings yet
- Review Update On TX of Spine MetastasisDocument13 pagesReview Update On TX of Spine MetastasisDr Zaw Hein HtetNo ratings yet
- MainDocument11 pagesMainDella Alvita SNo ratings yet
- Bone Tumor Risk Stratification and Management System A Consensus Guideline from the ACR Bone Reporting and Data System CommitteeDocument15 pagesBone Tumor Risk Stratification and Management System A Consensus Guideline from the ACR Bone Reporting and Data System CommitteeJuana GalloNo ratings yet
- Cancers: Rare Primary Malignant Bone SarcomasDocument14 pagesCancers: Rare Primary Malignant Bone SarcomasNGUYEN QUYNHNo ratings yet
- DUMBBELL TUMORS - REGA Surgical Treatment RegaDocument7 pagesDUMBBELL TUMORS - REGA Surgical Treatment Regajorgeroca2009No ratings yet
- Columna Paper Anato 2Document7 pagesColumna Paper Anato 2Claudio Cofré MansillaNo ratings yet
- Pi Is 0025619611619654Document10 pagesPi Is 0025619611619654Ivo Baaron ZarkovNo ratings yet
- Diagnosis and Management of Partial Thickness Rotator Cuff Tears_ A Comprehensive ReviewDocument13 pagesDiagnosis and Management of Partial Thickness Rotator Cuff Tears_ A Comprehensive ReviewKarim SabaNo ratings yet
- Bind Al 1996Document7 pagesBind Al 1996fira rifaNo ratings yet
- Xray Mri Vs HistopaDocument9 pagesXray Mri Vs HistopaDinda SaviraNo ratings yet
- Lahat2010 AngiosarcomaDocument9 pagesLahat2010 AngiosarcomaAntania IsyatiraNo ratings yet
- Association Between Changes in Body CompositionDocument7 pagesAssociation Between Changes in Body Compositionbouh aichetouNo ratings yet
- 02.28 - Required Lecture Reading - ClearDocument2 pages02.28 - Required Lecture Reading - Clearwhateverman123No ratings yet
- Kemoterapi AjuvanDocument18 pagesKemoterapi AjuvanAmberbu GabooNo ratings yet
- Radiofrequency AblationDocument9 pagesRadiofrequency AblationSwapnil BelsareNo ratings yet
- Curroncol 29 00465Document10 pagesCurroncol 29 00465jongsu kimNo ratings yet
- Cancer Treatment and Research CommunicationsDocument6 pagesCancer Treatment and Research CommunicationsCG MadeleineNo ratings yet
- In Vitro Chromosomal Aberration Frequency by Electrofishing on Poecilia latipinnaDocument29 pagesIn Vitro Chromosomal Aberration Frequency by Electrofishing on Poecilia latipinnaanon_769547714No ratings yet
- Jurnal Nyamuk Aedes AegyptiDocument7 pagesJurnal Nyamuk Aedes Aegyptianon_769547714No ratings yet
- Anatomi CorDocument3 pagesAnatomi Coranon_769547714No ratings yet
- Should You Take Dietary Supplements - NIH News in Health, August 2013Document2 pagesShould You Take Dietary Supplements - NIH News in Health, August 2013anon_769547714No ratings yet
- Migraines - Simple Steps To Head Off The Pain - Mayo ClinicDocument4 pagesMigraines - Simple Steps To Head Off The Pain - Mayo Clinicanon_769547714No ratings yet
- Personality Traits & Personality Types: What Is Personality?Document3 pagesPersonality Traits & Personality Types: What Is Personality?anon_769547714100% (1)
- Should You Take Dietary Supplements - NIH News in Health, August 2013Document2 pagesShould You Take Dietary Supplements - NIH News in Health, August 2013anon_769547714No ratings yet
- Radiation Therapy PrinciplesDocument22 pagesRadiation Therapy PrinciplesBMTNo ratings yet
- Final STEREOTACTIC RADIOSURGERY AND RADIOTHERAPYDocument61 pagesFinal STEREOTACTIC RADIOSURGERY AND RADIOTHERAPYGAGANPREET SINGHNo ratings yet
- Versa HD Product Brochure PDFDocument16 pagesVersa HD Product Brochure PDFFranciscoNo ratings yet
- Deep Brain Stimulation For The Treatment of Chronic, Intractable PainDocument15 pagesDeep Brain Stimulation For The Treatment of Chronic, Intractable PainnaimNo ratings yet
- World Survey On Parkinson Surgery Jourdain & SchechtmannDocument9 pagesWorld Survey On Parkinson Surgery Jourdain & SchechtmannGaston SchechtmannNo ratings yet
- KamasutraDocument20 pagesKamasutraBlach MentholNo ratings yet
- PDFDocument20 pagesPDFAtul JainNo ratings yet
- 41 - Mammograf Diamond - BR ENGDocument16 pages41 - Mammograf Diamond - BR ENGDerviş CalkuNo ratings yet
- Final - Specifications of Stereotactic FrameDocument2 pagesFinal - Specifications of Stereotactic FrameadeshdrNo ratings yet
- Quality Control in Cone-Beam Computed Tomography (CBCT) Efomp-Estro-Iaea ProtocolDocument151 pagesQuality Control in Cone-Beam Computed Tomography (CBCT) Efomp-Estro-Iaea ProtocolWira Hadi KusumaNo ratings yet
- Pineal Guidelines PDFDocument61 pagesPineal Guidelines PDFWilliam LeeNo ratings yet
- Aapm TG 179Document18 pagesAapm TG 179Ahmet Kürşat ÖzkanNo ratings yet
- Paragangliomas and Paraganglioma SyndromesDocument26 pagesParagangliomas and Paraganglioma SyndromessanasharNo ratings yet
- Clinical Practice 4: RadiotherapyDocument18 pagesClinical Practice 4: RadiotherapyallordNo ratings yet
- CK (S7) TDS PegDocument715 pagesCK (S7) TDS PegRadha SoniNo ratings yet
- Giotto-Brochure-3D Ing WebDocument16 pagesGiotto-Brochure-3D Ing WebMayra Marmolejo VargasNo ratings yet
- Occupational Safety HealthDocument729 pagesOccupational Safety HealthSarah AqirahNo ratings yet
- Benefits and CoverageDocument13 pagesBenefits and CoverageKelly VillarealNo ratings yet
- Oncologic Breast Surgery (2014) Veronesi Italia 290 Str.Document291 pagesOncologic Breast Surgery (2014) Veronesi Italia 290 Str.Nikola DolovacNo ratings yet
- Giotto Image3D BrochureDocument16 pagesGiotto Image3D BrochureGriselda Maria Pinto SanchezNo ratings yet
- Cosman: The Next Generation RF Pain ManagementDocument8 pagesCosman: The Next Generation RF Pain ManagementDaniel ParNo ratings yet
- Handbook of Evidence Based SRS and SBRT 2016Document258 pagesHandbook of Evidence Based SRS and SBRT 2016Piotr Jankowski100% (1)
- Dos 741 Clinical Protocol PresDocument25 pagesDos 741 Clinical Protocol Presapi-504593245No ratings yet
- Millers Anesthesia - Sixth Edition - Chapter 66 - Anesthesia For Robotic Surgery - 233Document44 pagesMillers Anesthesia - Sixth Edition - Chapter 66 - Anesthesia For Robotic Surgery - 233Adriana VickNo ratings yet
- Elekta Versa HD: Push The Boundaries of Your Stereotactic CapabilitiesDocument12 pagesElekta Versa HD: Push The Boundaries of Your Stereotactic CapabilitiesaminudinrahmanNo ratings yet
- BARD - Biopsy Product CatalogDocument36 pagesBARD - Biopsy Product CatalogRicardo DananNo ratings yet
- Roils Case StudyDocument3 pagesRoils Case Studyapi-483339757No ratings yet
- NIH Public Access: Author ManuscriptDocument26 pagesNIH Public Access: Author ManuscriptPaul RodrigoNo ratings yet
- MycrazylifepDocument302 pagesMycrazylifeplalaloopsy123No ratings yet
- LINAC HistoryDocument19 pagesLINAC Historycrusader8880% (1)