You might also like
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Capturing and Handling Wild Animals PDFDocument55 pagesCapturing and Handling Wild Animals PDFscrane@100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Solution Manual For Nesters Microbiology A Human Perspective 10th Edition Denise Anderson Sarah Salm Eugene NesterDocument9 pagesSolution Manual For Nesters Microbiology A Human Perspective 10th Edition Denise Anderson Sarah Salm Eugene NesterChristianColemannsja100% (40)
- Full Download Ebook PDF Prehospital Emergency Care 11th Edition PDFDocument41 pagesFull Download Ebook PDF Prehospital Emergency Care 11th Edition PDFrodney.pace130100% (29)
- Self Assessment ToolDocument25 pagesSelf Assessment ToolReinald Raven Guerrero100% (3)
- Final Module Food Borne Disease DiplomaDocument114 pagesFinal Module Food Borne Disease Diplomadoctormussieaberra100% (1)
- Handbook of Systemic Treatments For Cancer - 8th EditionDocument186 pagesHandbook of Systemic Treatments For Cancer - 8th EditionLaurențiu Acostioaei67% (3)
- The Difference of Tensile Bond Strength Between Total and Self Etch Adhesive Systems in DentinDocument5 pagesThe Difference of Tensile Bond Strength Between Total and Self Etch Adhesive Systems in Dentinmilleny faizaNo ratings yet
- Jukka MatilanaDocument41 pagesJukka Matilanamilleny faizaNo ratings yet
- Milleny Deyan - 030 - Pie ChartDocument1 pageMilleny Deyan - 030 - Pie Chartmilleny faizaNo ratings yet
- The Relationship Between Knowledge and Habit of Brushing Teeth With The Incidence of Dental Caries in Adolescents in MuntilanDocument3 pagesThe Relationship Between Knowledge and Habit of Brushing Teeth With The Incidence of Dental Caries in Adolescents in Muntilanmilleny faizaNo ratings yet
- Arguemntative Essay - Milleny DeyanDocument1 pageArguemntative Essay - Milleny Deyanmilleny faizaNo ratings yet
- Asphyxia NeonatorumDocument35 pagesAsphyxia NeonatorumMuhammad RagilNo ratings yet
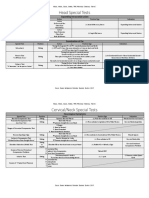
- 15 Head Neck Back Spine TMJ (Special Tests) (FINAL)Document8 pages15 Head Neck Back Spine TMJ (Special Tests) (FINAL)kath-kathNo ratings yet
- University of Kerbala College of Medicine Department of Pediatrics Clerkship Log-Book (Years 4) 2020-2021Document57 pagesUniversity of Kerbala College of Medicine Department of Pediatrics Clerkship Log-Book (Years 4) 2020-2021صفا أحمد هاشم جبار 4No ratings yet
- Laboratory and Diagnostic Tests Answer KeyDocument25 pagesLaboratory and Diagnostic Tests Answer KeyCourtney Dela FierraNo ratings yet
- Literature Entertainment Natural Sci - KasDocument9 pagesLiterature Entertainment Natural Sci - KasJoshua RomeaNo ratings yet
- College Name Number of Student Name Roll No Branch NameDocument4 pagesCollege Name Number of Student Name Roll No Branch NameNaman MishraNo ratings yet
- Neem Tree Extract As An Effective Insect Repellent CandleDocument9 pagesNeem Tree Extract As An Effective Insect Repellent CandlePol BearNo ratings yet
- The Extract of Banaba LeavesDocument6 pagesThe Extract of Banaba LeavesALDREW ENOCHNo ratings yet
- Emerging Adulthood As A Critical Stage in The Life Course - SpringerLinkDocument47 pagesEmerging Adulthood As A Critical Stage in The Life Course - SpringerLinkalmaasNo ratings yet
- Cues/Data Nursing Diagnosis Rationale Goals and Objectives Interventions Rationale Evaluation Subjective DataDocument5 pagesCues/Data Nursing Diagnosis Rationale Goals and Objectives Interventions Rationale Evaluation Subjective Datatimie_reyesNo ratings yet
- Name: - DateDocument3 pagesName: - DateMarv MarvNo ratings yet
- Power Point Hiv InggrisDocument8 pagesPower Point Hiv InggrisFitriNo ratings yet
- 2007 SAE Gov Ind MTG - ScarboroDocument15 pages2007 SAE Gov Ind MTG - Scarborogamusino2No ratings yet
- Diabetic Ketoacidosis (D.K.A) Beaumont Hospital Protocol: DiagnosisDocument1 pageDiabetic Ketoacidosis (D.K.A) Beaumont Hospital Protocol: Diagnosislouglee9174100% (1)
- Aktifitas Anti Jamur SerehDocument7 pagesAktifitas Anti Jamur SerehUlfaEstarinaNo ratings yet
- Epidemiology of Childhood Cancer in "Dharmais" Cancer HospitalDocument16 pagesEpidemiology of Childhood Cancer in "Dharmais" Cancer HospitalIndonesian Journal of CancerNo ratings yet
- Vol24no5 Pdf-Version PDFDocument152 pagesVol24no5 Pdf-Version PDFPuspaNo ratings yet
- Left Vs Right: Heart FailureDocument3 pagesLeft Vs Right: Heart FailureRosalinda PerigoNo ratings yet
- Malaria: Definition: Infection Due To PlasmodiumDocument17 pagesMalaria: Definition: Infection Due To PlasmodiumCLEMENTNo ratings yet
- Tourist Destination Residents Attitudes Towards Tourism During and After The COVID 19 PandemicDocument17 pagesTourist Destination Residents Attitudes Towards Tourism During and After The COVID 19 PandemicMusavi TouqeerNo ratings yet
- Post Extraction Lingual Mucosal Ulceration With Bone NecrosisDocument11 pagesPost Extraction Lingual Mucosal Ulceration With Bone NecrosisKrisbudiSetyawanNo ratings yet
- A Study of Kalo: Grade Level: Plan Duration: Unit Plan GoalDocument32 pagesA Study of Kalo: Grade Level: Plan Duration: Unit Plan Goalapi-294237871No ratings yet
- Tgs B. Inggris SalinanDocument11 pagesTgs B. Inggris SalinanDevita YuliantyNo ratings yet
- Stroke Iskemik (Dr. Dr. Syahrul, SPS (K) )Document14 pagesStroke Iskemik (Dr. Dr. Syahrul, SPS (K) )YogaNo ratings yet