You might also like
- Cracking Passwords GuideDocument45 pagesCracking Passwords GuideKorben100% (6)
- Unpriced Proposed Renovation of Bugolobi Flat, Block C For Uganda Coffee Development AuthorityDocument39 pagesUnpriced Proposed Renovation of Bugolobi Flat, Block C For Uganda Coffee Development AuthoritynicolasNo ratings yet
- Lesson Plan - Organization and ManagementDocument5 pagesLesson Plan - Organization and ManagementBilly Joe80% (15)
- Motivational QuotesDocument39 pagesMotivational QuotesNarayanan SubramanianNo ratings yet
- A320 Abnormal Notes: Last UpdatedDocument13 pagesA320 Abnormal Notes: Last UpdatedDevdatt SondeNo ratings yet
- Recurrent MeningitisDocument14 pagesRecurrent Meningitisidno1008No ratings yet
- Lethal Midline Granuloma-Stewart Nasal Nk/T-Cell Lymphoma-0ur ExperienceDocument9 pagesLethal Midline Granuloma-Stewart Nasal Nk/T-Cell Lymphoma-0ur Experienceopi akbarNo ratings yet
- Nk-Cell Lymphomas of The Head and Neck: AuthorDocument8 pagesNk-Cell Lymphomas of The Head and Neck: AuthorCharmila SariNo ratings yet
- Primary Nasal LymphomaDocument5 pagesPrimary Nasal LymphomaRini RahmawulandariNo ratings yet
- Extranodal Natural Killer T Cell Lymphoma, Nasal.1-1Document9 pagesExtranodal Natural Killer T Cell Lymphoma, Nasal.1-1kumar biradarNo ratings yet
- Primary Thyroid MALT Lymphoma With A Probable BR 2024 International JournalDocument5 pagesPrimary Thyroid MALT Lymphoma With A Probable BR 2024 International JournalRonald QuezadaNo ratings yet
- Lethal Midline Granuloma Importance of Early Diagnosis: A Case ReportDocument0 pagesLethal Midline Granuloma Importance of Early Diagnosis: A Case ReportdeolukmanaNo ratings yet
- Lee Et Al 2001 Case Report Meningococcal MeningitisDocument3 pagesLee Et Al 2001 Case Report Meningococcal MeningitisAsmae OuissadenNo ratings yet
- London F, Acta Neurol Belg, 2023Document4 pagesLondon F, Acta Neurol Belg, 2023Fabrizio Quiñonez FlorentinNo ratings yet
- Malignant Otitis External-Our Experience: R. B. Sardesai, T. KrishnakumarDocument4 pagesMalignant Otitis External-Our Experience: R. B. Sardesai, T. KrishnakumarSuci PramadianiNo ratings yet
- Tse 2017Document13 pagesTse 2017Ke XuNo ratings yet
- Non Hodgkin Lymphoma NasofaringDocument4 pagesNon Hodgkin Lymphoma Nasofaringsuci triana putriNo ratings yet
- Non-Hodgkin's Malignant Lymphomas of The Palatine Tonsils: A Case ReportDocument4 pagesNon-Hodgkin's Malignant Lymphomas of The Palatine Tonsils: A Case ReportWorld Journal of Case Reports and Clinical Images (ISSN: 2835-1568) CODEN:USANo ratings yet
- NKT CellDocument18 pagesNKT CelltisaprimaputriNo ratings yet
- Tuberculomas of The Brain With and Without Associated Meningitis: A Cohort of 28 Cases Treated With Anti-Tuberculosis Drugs at A Tertiary Care CentreDocument4 pagesTuberculomas of The Brain With and Without Associated Meningitis: A Cohort of 28 Cases Treated With Anti-Tuberculosis Drugs at A Tertiary Care CentreDestyNo ratings yet
- Kwong 2012Document8 pagesKwong 2012Ke XuNo ratings yet
- Diagnosis in OncologyDocument22 pagesDiagnosis in OncologyAndi SuryajayaNo ratings yet
- Medicine: An Unusual Extranodal Natural Killer/t-Cell Lymphoma Presenting As Chronic LaryngitisDocument4 pagesMedicine: An Unusual Extranodal Natural Killer/t-Cell Lymphoma Presenting As Chronic Laryngitisnurul atika havizNo ratings yet
- Extracranial Metastases of Anaplastic Meningioma: Case ReportDocument6 pagesExtracranial Metastases of Anaplastic Meningioma: Case ReportRizky AdriansahNo ratings yet
- Malignant Otitis Externa: An Emerging Complication: Original ArticleDocument3 pagesMalignant Otitis Externa: An Emerging Complication: Original ArticleWa Ode Meutya ZawawiNo ratings yet
- 13 CR Lethal MidlineDocument3 pages13 CR Lethal MidlineSudhir BayyaNo ratings yet
- How We Treat NK/T-cell Lymphomas: Review Open AccessDocument13 pagesHow We Treat NK/T-cell Lymphomas: Review Open AccessRucelia Michiko PiriNo ratings yet
- Follicular Dendritic Cell Sarcoma of The Tonssilar About A CaseDocument4 pagesFollicular Dendritic Cell Sarcoma of The Tonssilar About A CaseInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Leptomeningeal DiseaseDocument17 pagesLeptomeningeal DiseaseForem ZayneNo ratings yet
- Molecular Biomarkers in Sinonasal Cancers: New Frontiers in Diagnosis and TreatmentDocument13 pagesMolecular Biomarkers in Sinonasal Cancers: New Frontiers in Diagnosis and TreatmentventyperdanasariNo ratings yet
- Dermatomyositis and Undifferentiated Nasopharyngeal Carcinoma. A Rare Presentation of A Rare MalignancyDocument4 pagesDermatomyositis and Undifferentiated Nasopharyngeal Carcinoma. A Rare Presentation of A Rare MalignancyasclepiuspdfsNo ratings yet
- Sinonasal Diffuse Large B Cell LymphomaDocument6 pagesSinonasal Diffuse Large B Cell LymphomaRini RahmawulandariNo ratings yet
- The Melanoma SLN Invasion Level As A PrognositicDocument11 pagesThe Melanoma SLN Invasion Level As A PrognositicMariana UsatiiNo ratings yet
- A Tuzcu M Bahceci MK Celen N Kilinc S Ozmen: Correspondence AddressDocument4 pagesA Tuzcu M Bahceci MK Celen N Kilinc S Ozmen: Correspondence AddressiqbaladiNo ratings yet
- Otitis ExternaDocument4 pagesOtitis ExternaCesar Mauricio Daza CajasNo ratings yet
- Encrucijadas ModelosDocument4 pagesEncrucijadas ModelosArandano L.No ratings yet
- 035 Quick Queries Acute RhinosinusitisDocument4 pages035 Quick Queries Acute RhinosinusitisRika FitriaNo ratings yet
- Review Article: Early Detection of Nasopharyngeal CarcinomaDocument7 pagesReview Article: Early Detection of Nasopharyngeal CarcinomaajengdenandaNo ratings yet
- Cancer, Nasopharyngeal Carcinoma (NPC) : Statpearls (Internet) - Treasure Island (FL) : Statpearls Publishing 2020 JanDocument11 pagesCancer, Nasopharyngeal Carcinoma (NPC) : Statpearls (Internet) - Treasure Island (FL) : Statpearls Publishing 2020 JanikaNo ratings yet
- Multiple Cavitary Lung Lesions in An Adolescent - Case Report of A Rare Presentation of Nodular Lymphocyte Predominant Hodgkin LymphomaDocument4 pagesMultiple Cavitary Lung Lesions in An Adolescent - Case Report of A Rare Presentation of Nodular Lymphocyte Predominant Hodgkin LymphomaManisha UppalNo ratings yet
- Unknown Primary Cancer of The Head and Neck - A MultidisciplinaryDocument10 pagesUnknown Primary Cancer of The Head and Neck - A MultidisciplinaryFreddy Eduardo Navarro BautistaNo ratings yet
- Invasive Cryptococcal Meningitis Presenting As A Skull Base Mass in An Immunocompetent Host: A Case ReportDocument5 pagesInvasive Cryptococcal Meningitis Presenting As A Skull Base Mass in An Immunocompetent Host: A Case ReportAsep RiswandiNo ratings yet
- Kern 2003Document8 pagesKern 2003Eryc Luan DiasNo ratings yet
- HTMLDocument2 pagesHTMLbishoy raflaNo ratings yet
- The History Holds The Key in This Gardener With A Skin InfectionDocument4 pagesThe History Holds The Key in This Gardener With A Skin InfectionPercy Ureta SierraNo ratings yet
- Efficacy of Doxycycline in The Treatment of Early Stages of Mycosis Fungoides, A Randomized Controlled TrialDocument29 pagesEfficacy of Doxycycline in The Treatment of Early Stages of Mycosis Fungoides, A Randomized Controlled TrialMelvin Florens Tania GongaNo ratings yet
- 0550262Document3 pages0550262Bagoes Ario BimoNo ratings yet
- Bronchogenic CaDocument4 pagesBronchogenic CaFortune RubengoNo ratings yet
- Confirmed Tuberculous Brain Miliary in An Immunocompetent Patient: A Case ReportDocument3 pagesConfirmed Tuberculous Brain Miliary in An Immunocompetent Patient: A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Synchronous Squamous Cell Carcinoma of The Lip and Nasopharyngeal Carcinoma - A Rare Case Report.Document4 pagesSynchronous Squamous Cell Carcinoma of The Lip and Nasopharyngeal Carcinoma - A Rare Case Report.International Journal of Innovative Science and Research Technology100% (1)
- Mycosis Fungoides and Sézary Syndrome: SeminarDocument13 pagesMycosis Fungoides and Sézary Syndrome: Seminarapi-26302710No ratings yet
- 6324-Article Text-21760-1-10-20210620Document3 pages6324-Article Text-21760-1-10-20210620Fritzienico BaskoroNo ratings yet
- Leukemia Research Paper Thesis StatementDocument9 pagesLeukemia Research Paper Thesis Statementaparnaharrisonstamford100% (1)
- RetinoblastomaDocument16 pagesRetinoblastomaDiego Joaquín RiveraNo ratings yet
- Artigo 39Document5 pagesArtigo 39raudneimNo ratings yet
- LungIndia323241-4636559 125245Document5 pagesLungIndia323241-4636559 125245Nishant AggarwalNo ratings yet
- AbscessDocument12 pagesAbscesslittlecandiesNo ratings yet
- New 1Document12 pagesNew 1Muhammad SyaifullahNo ratings yet
- Ref 31 Meningeal LeukemiaDocument9 pagesRef 31 Meningeal LeukemiamuarifNo ratings yet
- Extra Renal Rhabdoid Tumor in An Adult Presentin 2024 International JournalDocument5 pagesExtra Renal Rhabdoid Tumor in An Adult Presentin 2024 International JournalRonald QuezadaNo ratings yet
- NocardiaDocument6 pagesNocardiadocalsultanNo ratings yet
- Nasal Vestibular Furunculosis Presenting As The Rudolph SignDocument2 pagesNasal Vestibular Furunculosis Presenting As The Rudolph Signyeni novi yantiNo ratings yet
- Swaiman Chapter 133Document9 pagesSwaiman Chapter 133Van John MagallanesNo ratings yet
- Jurnal Tonsil Limfoma Non HodgkinDocument5 pagesJurnal Tonsil Limfoma Non HodgkinAhmad RamadhanuNo ratings yet
- Fast Facts: Blastic Plasmacytoid Dendritic Cell Neoplasm: Shedding light on a rare diseaseFrom EverandFast Facts: Blastic Plasmacytoid Dendritic Cell Neoplasm: Shedding light on a rare diseaseNo ratings yet
- Hong2015Document13 pagesHong2015Andi Imam Buchari nstNo ratings yet
- Title: DDGP Versus SMILE in Newly Diagnosed Advanced NaturalDocument29 pagesTitle: DDGP Versus SMILE in Newly Diagnosed Advanced NaturalAndi Imam Buchari nstNo ratings yet
- Xu2017Document9 pagesXu2017Andi Imam Buchari nstNo ratings yet
- What We Should Know About Natural Killer/t Cell Lymphomas: Jie Xiong Weili ZhaoDocument7 pagesWhat We Should Know About Natural Killer/t Cell Lymphomas: Jie Xiong Weili ZhaoAndi Imam Buchari nstNo ratings yet
- Eng - Kronoligis Ani ManurungDocument9 pagesEng - Kronoligis Ani ManurungAndi Imam Buchari nstNo ratings yet
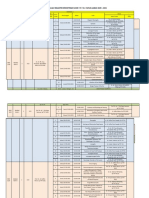
- Jadwal MKK Sem 2 Fix 2021Document2 pagesJadwal MKK Sem 2 Fix 2021Andi Imam Buchari nstNo ratings yet
- Exercise Chapter 4 This Is How You Do ItDocument10 pagesExercise Chapter 4 This Is How You Do ItAgustina WidiyantiNo ratings yet
- Entropy (Information Theory)Document17 pagesEntropy (Information Theory)joseph676No ratings yet
- Pre-Socratic Pluralism AtomismDocument1 pagePre-Socratic Pluralism AtomismpresjmNo ratings yet
- Shower Tapware: For More Information and Detailed Specifications Please Refer To Our Website: WWW - Plumbline.co - NZDocument11 pagesShower Tapware: For More Information and Detailed Specifications Please Refer To Our Website: WWW - Plumbline.co - NZNoman KhanNo ratings yet
- FYP List 2020 21RDocument3 pagesFYP List 2020 21RSaif UllahNo ratings yet
- E650E650M-17 Guía Estándar para El Montaje de Sensores Piezoeléctricos de Emisión Acústica1Document4 pagesE650E650M-17 Guía Estándar para El Montaje de Sensores Piezoeléctricos de Emisión Acústica1fredy lopezNo ratings yet
- History of Nursing: Nursing in The Near EastDocument7 pagesHistory of Nursing: Nursing in The Near EastCatherine PradoNo ratings yet
- Lab 4 SimulationDocument8 pagesLab 4 SimulationaziziNo ratings yet
- Itf EssayDocument18 pagesItf EssayTharshiNo ratings yet
- Network Models For Seat Allocation On Flights: Moshe Dror,?Document12 pagesNetwork Models For Seat Allocation On Flights: Moshe Dror,?Isabel VillaNo ratings yet
- Egalitarianism As UK: Source: Hofstede Insights, 2021Document4 pagesEgalitarianism As UK: Source: Hofstede Insights, 2021kamalpreet kaurNo ratings yet
- Introduction To SAP: Venkat Emani FICO Certified Consultant / TrainerDocument22 pagesIntroduction To SAP: Venkat Emani FICO Certified Consultant / TrainerVenkat EmaniNo ratings yet
- Perfume 130Document3 pagesPerfume 130Gurdeep BhattalNo ratings yet
- Durham E-ThesesDocument203 pagesDurham E-ThesesH Man SharifNo ratings yet
- Metric Conversion WorksheetDocument3 pagesMetric Conversion WorksheetKaiden HughesNo ratings yet
- Machine Learning and Supply Chain Management - ADocument5 pagesMachine Learning and Supply Chain Management - AAhmed AbassNo ratings yet
- Helena HelsenDocument2 pagesHelena HelsenragastrmaNo ratings yet
- Free Vibration of SDOFDocument2 pagesFree Vibration of SDOFjajajajNo ratings yet
- Thetford c250 InstallationDocument19 pagesThetford c250 InstallationCatalin Bejan100% (1)
- McMurdo FastFind 220 PLB DatasheetDocument4 pagesMcMurdo FastFind 220 PLB DatasheetGiorgos PapadopoulosNo ratings yet
- Hatchery Practice: InternationalDocument40 pagesHatchery Practice: Internationalabhe prasetyaNo ratings yet
- Fastener Torque Charts: Phone: 1-800-558-2808 Fax: 1-800-553-8769Document2 pagesFastener Torque Charts: Phone: 1-800-558-2808 Fax: 1-800-553-8769KOMATSU SHOVELNo ratings yet
- Al Rafay ProfileDocument8 pagesAl Rafay ProfileRana UsmanNo ratings yet
- Baptismal DelayDocument20 pagesBaptismal DelayfiohdiohhodoNo ratings yet
- VisualizationDocument2 pagesVisualizationKIRAN H SNo ratings yet