You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Auerbach's Wilderness Medicine PDFDocument1,672 pagesAuerbach's Wilderness Medicine PDFKieran D90% (10)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- CPR Study Guide 2021: Online CPR Cheat SheetDocument14 pagesCPR Study Guide 2021: Online CPR Cheat SheetHenz Freeman0% (1)
- Chapter 1 Introduction To Emergency Medical CareDocument19 pagesChapter 1 Introduction To Emergency Medical Carejmmos207064100% (1)
- GuideDocument52 pagesGuidemihaelklajner100% (1)
- A Focused Update On NPWT With Instillation1636470749287Document41 pagesA Focused Update On NPWT With Instillation1636470749287Peter KhanhNo ratings yet
- Hapwoc 1636470869099Document6 pagesHapwoc 1636470869099Peter KhanhNo ratings yet
- Woundcon Fall 2021 Syllabus and Exhibitor GuideDocument25 pagesWoundcon Fall 2021 Syllabus and Exhibitor GuidePeter KhanhNo ratings yet
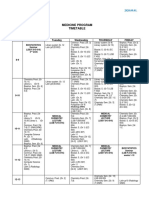
- 1 YEAR (Group 1-12) : Medicine Program TimetableDocument20 pages1 YEAR (Group 1-12) : Medicine Program TimetablePeter KhanhNo ratings yet
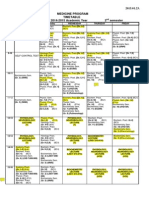
- 2nd Semester GM GR.1Document1 page2nd Semester GM GR.1Peter KhanhNo ratings yet
- FIGURE: Haemobartonella Felis in Blood From A Cat. Organisms Appear As Small Cocci, Rods, orDocument3 pagesFIGURE: Haemobartonella Felis in Blood From A Cat. Organisms Appear As Small Cocci, Rods, orabdulNo ratings yet
- (PDF) Impact of Orthodontic Treatment On Periodontal Tissues A Narrative Review of Multidisciplinary LiteratureDocument10 pages(PDF) Impact of Orthodontic Treatment On Periodontal Tissues A Narrative Review of Multidisciplinary LiteratureMirnaLizNo ratings yet
- Activity Intolerance YAp ER NCPDocument2 pagesActivity Intolerance YAp ER NCPmecz26100% (2)
- Katharina Hiria Daundy - Premature Contraction in PregnancyDocument11 pagesKatharina Hiria Daundy - Premature Contraction in PregnancyObgyn AgustusNo ratings yet
- Feeding Device Shaju V Cherian and Dipu KCDocument20 pagesFeeding Device Shaju V Cherian and Dipu KCShaju V CherianNo ratings yet
- Methods of Nutrient DeliveryDocument3 pagesMethods of Nutrient DeliveryFarmisa MannanNo ratings yet
- Surgical Complication of Typhoid FeverDocument10 pagesSurgical Complication of Typhoid FeverHelsa Eldatarina JNo ratings yet
- Resume Nad Part 111Document2 pagesResume Nad Part 111api-374698901No ratings yet
- Askep CKDDocument55 pagesAskep CKDyuli ariyantiNo ratings yet
- Role of MDCT in Coronary Artery Disease: Swachchhanda Songmen 2071Document63 pagesRole of MDCT in Coronary Artery Disease: Swachchhanda Songmen 2071Dr KhanNo ratings yet
- Personal Notes Excpetional StuffDocument352 pagesPersonal Notes Excpetional StuffYagyeshNo ratings yet
- Judgment: in The High Court of The Republic of SingaporeDocument26 pagesJudgment: in The High Court of The Republic of SingaporeTerryNo ratings yet
- RM Mcom Part 1 AssignmentDocument13 pagesRM Mcom Part 1 AssignmentBrayan AlmeidaNo ratings yet
- Science: Modified Strategic Intervention MaterialsDocument42 pagesScience: Modified Strategic Intervention Materialsmichelle sumatNo ratings yet
- Module 7 Anxiety Disorders PDFDocument12 pagesModule 7 Anxiety Disorders PDFprashansha kumudNo ratings yet
- Essay On Fracture ComplicationsDocument9 pagesEssay On Fracture ComplicationsadibahNo ratings yet
- New Cystic Fibrosis Diagnosis FinalDocument26 pagesNew Cystic Fibrosis Diagnosis FinalSuman DeshmukhNo ratings yet
- Tracheostomy Site CancerDocument2 pagesTracheostomy Site CancerСварооп СатурнскыNo ratings yet
- HIRA ToolDocument26 pagesHIRA Toolsreekala2007No ratings yet
- Kawasaki Disease-Case-Study LATEST CHANGESDocument24 pagesKawasaki Disease-Case-Study LATEST CHANGESJesse James Advincula Edjec100% (7)
- Non Communicable DiseasesDocument13 pagesNon Communicable Diseaseszzzsubedi100% (1)
- Common Poison in ChildrenDocument31 pagesCommon Poison in ChildrenNimi BatuboNo ratings yet
- Activity On Lesson 2 Common Injuries in DanceDocument10 pagesActivity On Lesson 2 Common Injuries in DancePammy AlivenNo ratings yet
- QSE6034: Teknologi Dan Inovasi Dalam Sains SukanDocument3 pagesQSE6034: Teknologi Dan Inovasi Dalam Sains SukanMohamad Ramlan RamliNo ratings yet
- Rajkumar PDFDocument5 pagesRajkumar PDFAmaradeepika JagannathanNo ratings yet
- Focus Diagnosis Action Response Subjective: "I Hate Water and I Don't Drink It Much " DXDocument2 pagesFocus Diagnosis Action Response Subjective: "I Hate Water and I Don't Drink It Much " DXGrape Juice100% (1)