You might also like
- Urinary Stones: Medical and Surgical ManagementFrom EverandUrinary Stones: Medical and Surgical ManagementMichael GrassoNo ratings yet
- Pathophysiology-Based Treatment of UrolithiasisDocument7 pagesPathophysiology-Based Treatment of UrolithiasisLea Bali Ulina SinurayaNo ratings yet
- jurnal kel. 3Document12 pagesjurnal kel. 3ho himmaNo ratings yet
- DR MarwanDocument8 pagesDR MarwanMarwan Ibrahim0% (1)
- Kidney Tissue Targeted Metabolic Profiling of Unilateral Ureteral Obstruction Rats by NMRDocument12 pagesKidney Tissue Targeted Metabolic Profiling of Unilateral Ureteral Obstruction Rats by NMRkmdfwkefmNo ratings yet
- An Experimental Study of Ascorbic Acid Effects in Acute RenalDocument9 pagesAn Experimental Study of Ascorbic Acid Effects in Acute RenalfgonzalezNo ratings yet
- Review Article Renal Stone Disease: Causes, Evaluation and Medical TreatmentDocument9 pagesReview Article Renal Stone Disease: Causes, Evaluation and Medical TreatmentZulfikar BasriNo ratings yet
- A Role For Uric Acid in The Progression of Renal DiseaseDocument10 pagesA Role For Uric Acid in The Progression of Renal DiseaseFausiah Ulva MNo ratings yet
- Nephrology - 2017 - Heidari - Mechanism of Valproic Acid Induced Fanconi Syndrome Involves Mitochondrial Dysfunction andDocument11 pagesNephrology - 2017 - Heidari - Mechanism of Valproic Acid Induced Fanconi Syndrome Involves Mitochondrial Dysfunction andmatheus.tenorioNo ratings yet
- Molecular mechanisms of Selaginella lepidophylla chloroform extract's protective effect in lithiasic ratsDocument11 pagesMolecular mechanisms of Selaginella lepidophylla chloroform extract's protective effect in lithiasic ratsPlacido Rojas FrancoNo ratings yet
- Recurrent Renal Colic: A Case StudyDocument2 pagesRecurrent Renal Colic: A Case StudyTheQueensafa90No ratings yet
- Research Article A Specific Urinary Amino Acid Profile Characterizes People With Kidney StonesDocument7 pagesResearch Article A Specific Urinary Amino Acid Profile Characterizes People With Kidney StonesNandy SwariNo ratings yet
- Dosis Vitamin C Pada TimbalDocument7 pagesDosis Vitamin C Pada Timbalintan permata balqisNo ratings yet
- Kidney StonesDocument50 pagesKidney StonesMaxi SpositoNo ratings yet
- NEFOLITIASISDocument10 pagesNEFOLITIASISjim manuel dominguez rosalesNo ratings yet
- Renal Tubular Acidosis PDFDocument7 pagesRenal Tubular Acidosis PDFishtiaq ahmadNo ratings yet
- Molecules 1 PDFDocument11 pagesMolecules 1 PDFanuNo ratings yet
- Vit ADocument8 pagesVit AshandraNo ratings yet
- 2012 The Effects of Medical Ozone Therapy On Renal Ischemia:Reperfusion InjuryDocument6 pages2012 The Effects of Medical Ozone Therapy On Renal Ischemia:Reperfusion InjuryAcupuntura de EquinosNo ratings yet
- Lan 2014Document7 pagesLan 2014GHUJNo ratings yet
- Rajiv Gandhi University of Health Sciences, Karnataka, BangaloreDocument11 pagesRajiv Gandhi University of Health Sciences, Karnataka, BangaloreDiksifableNo ratings yet
- Toxicology and Applied Pharmacology: Séin O'Connell, Craig Slattery, Michael P. Ryan, Tara McmorrowDocument10 pagesToxicology and Applied Pharmacology: Séin O'Connell, Craig Slattery, Michael P. Ryan, Tara McmorrowDoyin AwodeleNo ratings yet
- Core Curriculum NefrolitiasisDocument13 pagesCore Curriculum NefrolitiasisOscar MoralesNo ratings yet
- Lacto BacillusDocument12 pagesLacto BacillusGiancarlo CajahuaringaNo ratings yet
- Ionized Alkaline Water New Strategy For ManagementDocument6 pagesIonized Alkaline Water New Strategy For ManagementninoNo ratings yet
- Biomarkers in UrolithiasisselloDocument11 pagesBiomarkers in Urolithiasisselloregigaby02No ratings yet
- Patofisiologi Kidney StonesDocument8 pagesPatofisiologi Kidney StonespipitNo ratings yet
- Pastor 1997Document8 pagesPastor 1997Alexsandro Nicolay PontoanNo ratings yet
- IJAPB PAPERDocument25 pagesIJAPB PAPERDurga MadhuriNo ratings yet
- THESIS-Phyllantus Chapter OneDocument8 pagesTHESIS-Phyllantus Chapter OneGeddah Grace RanocoNo ratings yet
- Predictive Value of Kidney Stone Composition in The Detection of Metabolic AbnormalitiesDocument7 pagesPredictive Value of Kidney Stone Composition in The Detection of Metabolic Abnormalitiesjarivera1300No ratings yet
- Kalantar Zadeh Etal 2021 Preserving Kidney Function in PeopleDocument61 pagesKalantar Zadeh Etal 2021 Preserving Kidney Function in Peoplenpuspa243No ratings yet
- Design of Drug Like Hepsin Inhibitors Against Prostat - 2020 - Acta PharmaceuticDocument12 pagesDesign of Drug Like Hepsin Inhibitors Against Prostat - 2020 - Acta PharmaceuticMohammed Shuaib AhmedNo ratings yet
- Pathophysiology of Nephrolithiasis PDFDocument9 pagesPathophysiology of Nephrolithiasis PDFLayuganlovelyNo ratings yet
- Sweet potato leaves inhibit nitric oxide productionDocument7 pagesSweet potato leaves inhibit nitric oxide productionDessy Erlyani Mugita SariNo ratings yet
- Jcem 1847Document14 pagesJcem 1847jess peltraNo ratings yet
- Calcium Renal Lithiasis Metabolic Diagnosis and MeDocument8 pagesCalcium Renal Lithiasis Metabolic Diagnosis and MefafoulolNo ratings yet
- An Overview On Potent Indigenous Herbs For Urinary Tract InfirmityDocument6 pagesAn Overview On Potent Indigenous Herbs For Urinary Tract InfirmityE PrenssaNo ratings yet
- Uric Acid in Chronic Kidney Disease: CA Murakami, SM SozioDocument6 pagesUric Acid in Chronic Kidney Disease: CA Murakami, SM SozioHanny Friska YudistyawanNo ratings yet
- Effect of Thymoquinone On Ethylene Glycol-Induced Kidney Calculi in RatsDocument7 pagesEffect of Thymoquinone On Ethylene Glycol-Induced Kidney Calculi in RatsrajkiranENo ratings yet
- Etm 14 02 1496Document9 pagesEtm 14 02 1496Bella La Rosa HusnaNo ratings yet
- 1 s2.0 S2161831323002715 MainDocument15 pages1 s2.0 S2161831323002715 MainAdiyanto DidietNo ratings yet
- Phyllanthus Niruri As A Promising Alternative Treatment For NephrolithiasisDocument8 pagesPhyllanthus Niruri As A Promising Alternative Treatment For NephrolithiasisIndra PradanaNo ratings yet
- AsdasdDocument6 pagesAsdasdjonoNo ratings yet
- Validation of A Novel Diagnostic Test For Assessing The Risk of Urinary Uric ACID CRYSTALLIZACIONDocument6 pagesValidation of A Novel Diagnostic Test For Assessing The Risk of Urinary Uric ACID CRYSTALLIZACIONMARIANNE CASTILLO ESCOBARNo ratings yet
- Effects of Sevelamer Hydrochloride On Uremic Toxins Serum Indoxyl Sulfate and P-Cresyl Sulfate in Hemodialysis PatientsDocument6 pagesEffects of Sevelamer Hydrochloride On Uremic Toxins Serum Indoxyl Sulfate and P-Cresyl Sulfate in Hemodialysis PatientsprimaNo ratings yet
- Metabolic Acidosis - An Underestimated Problem After Kidney Transplantation?Document6 pagesMetabolic Acidosis - An Underestimated Problem After Kidney Transplantation?Daphne HernaezNo ratings yet
- Lead Induced Hepato-Renal Damage in Male Albino Rats and Effects of Activated CharcoalDocument10 pagesLead Induced Hepato-Renal Damage in Male Albino Rats and Effects of Activated Charcoaldicky saputraNo ratings yet
- MM NefrolitiasisDocument22 pagesMM NefrolitiasisRudi HandokoNo ratings yet
- Jvim 29 028Document7 pagesJvim 29 028Marilyn Patricia Abello GarciaNo ratings yet
- Uuo 1Document7 pagesUuo 1asaNo ratings yet
- Hypercalcemia and Calcium Oxalate Urolithiasis in Cats: A Report of Five CasesDocument5 pagesHypercalcemia and Calcium Oxalate Urolithiasis in Cats: A Report of Five CasesJean AmorinNo ratings yet
- Impact of Stone Removal On Renal Function A Review - PMCDocument1 pageImpact of Stone Removal On Renal Function A Review - PMCTazyeen AlamNo ratings yet
- Uric AcidDocument6 pagesUric Acidmonday125100% (1)
- Fmed 07 617786Document5 pagesFmed 07 617786Ashifa AshfaNo ratings yet
- Fmed 07 617786Document5 pagesFmed 07 617786Ashifa AshfaNo ratings yet
- Are All Fluids Bad For The Kidney?Document10 pagesAre All Fluids Bad For The Kidney?Xavier AbrilNo ratings yet
- ATP5B and ETFB Metabolic Markers in Children With Congenital HydronephrosisDocument5 pagesATP5B and ETFB Metabolic Markers in Children With Congenital HydronephrosisZwinglie SandagNo ratings yet
- Hydrogen Therapy For Diabetic Erectile DysfunctionDocument4 pagesHydrogen Therapy For Diabetic Erectile DysfunctionIhorNo ratings yet
- s11255-018-1819-8Document8 pagess11255-018-1819-8Aaron Paul BernasNo ratings yet
- Chemical Carcinogenesis: Metabolic Activation, DNA Adducts, Multistage ModelDocument85 pagesChemical Carcinogenesis: Metabolic Activation, DNA Adducts, Multistage ModelNidyaletchmy ReddyNo ratings yet
- Intl Journal of Cancer - 2014 - Lakritz - Beneficial Bacteria Stimulate Host Immune Cells To Counteract Dietary and GeneticDocument12 pagesIntl Journal of Cancer - 2014 - Lakritz - Beneficial Bacteria Stimulate Host Immune Cells To Counteract Dietary and GeneticTrang MốcNo ratings yet
- Lund-Browder Chart Estimates Burn ExtentDocument7 pagesLund-Browder Chart Estimates Burn ExtentMarco1998No ratings yet
- Cytology Sample Collection and Preparation For Veterinary PractitionersDocument8 pagesCytology Sample Collection and Preparation For Veterinary PractitionersKmo mastnNo ratings yet
- Anti Dengue Campaign ProposalDocument2 pagesAnti Dengue Campaign Proposalprithib0% (1)
- Five Animals of Shaolin Dissemination AnDocument41 pagesFive Animals of Shaolin Dissemination Angouthamk5151No ratings yet
- Outpatient InformationDocument2 pagesOutpatient InformationBobdNo ratings yet
- Rheumatoid Arthritis Drug StudyDocument2 pagesRheumatoid Arthritis Drug StudyChristaNo ratings yet
- Parasitology Guide Questions 1Document2 pagesParasitology Guide Questions 1Cess LacatangoNo ratings yet
- Movie Review - Seven Sundays (Barredo)Document2 pagesMovie Review - Seven Sundays (Barredo)Julienne BarredoNo ratings yet
- Strokeaha 120 030653Document5 pagesStrokeaha 120 030653indanazulfaaNo ratings yet
- Protect Yourself and Others: Get the COVID-19 Vaccine (39Document4 pagesProtect Yourself and Others: Get the COVID-19 Vaccine (39Shane Patrick PanilagNo ratings yet
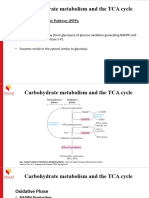
- Carbohydrate Metabolism TCA Cycle - (PPP and Glycogen Metabolism)Document17 pagesCarbohydrate Metabolism TCA Cycle - (PPP and Glycogen Metabolism)Frolian MichaelNo ratings yet
- Unit 10Document7 pagesUnit 10Minh Đức NghiêmNo ratings yet
- 50 Pediatric Anesthesia Questions: © 2004, Roy G. Soto, M.DDocument4 pages50 Pediatric Anesthesia Questions: © 2004, Roy G. Soto, M.DGanda SilitongaNo ratings yet
- Maharashtra PG Medical Entrance Review CorrectionsDocument38 pagesMaharashtra PG Medical Entrance Review Correctionsklingon45No ratings yet
- Trend Analysis of Exponential Increase of COVID-19 Cases in Pakistan: An InterpretationDocument21 pagesTrend Analysis of Exponential Increase of COVID-19 Cases in Pakistan: An InterpretationBongoNo ratings yet
- Golden Shield BrochureDocument11 pagesGolden Shield BrochureRak Esh RakeshNo ratings yet
- Reglan Indication Side Effects NursingDocument2 pagesReglan Indication Side Effects NursingRem remNo ratings yet
- Drug Education, Prevention and ControlDocument18 pagesDrug Education, Prevention and ControlMaurene MendozaNo ratings yet
- BathingDocument53 pagesBathingRandySandovalNo ratings yet
- MoniliniaDocument2 pagesMoniliniaFany25No ratings yet
- TLE-HE (Dressmaking) : Activity Sheet Quarter 0 - MELC 4Document15 pagesTLE-HE (Dressmaking) : Activity Sheet Quarter 0 - MELC 4Mari PagxNo ratings yet
- DOH's Response to President Duterte's Marching Orders on Drug Treatment and RehabilitationDocument52 pagesDOH's Response to President Duterte's Marching Orders on Drug Treatment and Rehabilitationpurple0920No ratings yet
- Basics of Immunity and InflammationDocument6 pagesBasics of Immunity and InflammationNegrus Stefan100% (1)
- IeltsDocument65 pagesIeltskitten_alina92% (13)
- Generador Marcapaso Osypka Pace101h IfuDocument35 pagesGenerador Marcapaso Osypka Pace101h IfuJordan BonnettNo ratings yet
- PTB Case-StudyDocument64 pagesPTB Case-StudyBeverly DatuNo ratings yet
- Abrar DMC Medicine OSPEDocument77 pagesAbrar DMC Medicine OSPEmfshihab3352No ratings yet
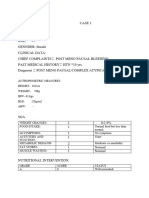
- Case 1Document7 pagesCase 1bsc.clinicalnutrition2018No ratings yet
- Meltdown: Nuclear disaster and the human cost of going criticalFrom EverandMeltdown: Nuclear disaster and the human cost of going criticalRating: 5 out of 5 stars5/5 (5)
- Is That a Fact?: Frauds, Quacks, and the Real Science of Everyday LifeFrom EverandIs That a Fact?: Frauds, Quacks, and the Real Science of Everyday LifeRating: 4.5 out of 5 stars4.5/5 (3)
- Periodic Tales: A Cultural History of the Elements, from Arsenic to ZincFrom EverandPeriodic Tales: A Cultural History of the Elements, from Arsenic to ZincRating: 3.5 out of 5 stars3.5/5 (137)
- Organic Chemistry for Schools: Advanced Level and Senior High SchoolFrom EverandOrganic Chemistry for Schools: Advanced Level and Senior High SchoolNo ratings yet
- Essential Oil Chemistry Formulating Essential Oil Blends that Heal - Aldehyde - Ketone - Lactone: Healing with Essential OilFrom EverandEssential Oil Chemistry Formulating Essential Oil Blends that Heal - Aldehyde - Ketone - Lactone: Healing with Essential OilRating: 5 out of 5 stars5/5 (1)
- An Introduction to the Periodic Table of Elements : Chemistry Textbook Grade 8 | Children's Chemistry BooksFrom EverandAn Introduction to the Periodic Table of Elements : Chemistry Textbook Grade 8 | Children's Chemistry BooksRating: 5 out of 5 stars5/5 (1)
- The Disappearing Spoon: And Other True Tales of Madness, Love, and the History of the World from the Periodic Table of the ElementsFrom EverandThe Disappearing Spoon: And Other True Tales of Madness, Love, and the History of the World from the Periodic Table of the ElementsRating: 4 out of 5 stars4/5 (146)
- Coating and Drying Defects: Troubleshooting Operating ProblemsFrom EverandCoating and Drying Defects: Troubleshooting Operating ProblemsRating: 5 out of 5 stars5/5 (1)
- Chemistry at Home - A Collection of Experiments and Formulas for the Chemistry EnthusiastFrom EverandChemistry at Home - A Collection of Experiments and Formulas for the Chemistry EnthusiastNo ratings yet
- The Periodic Table of Elements - Post-Transition Metals, Metalloids and Nonmetals | Children's Chemistry BookFrom EverandThe Periodic Table of Elements - Post-Transition Metals, Metalloids and Nonmetals | Children's Chemistry BookNo ratings yet
- Guidelines for Asset Integrity ManagementFrom EverandGuidelines for Asset Integrity ManagementRating: 5 out of 5 stars5/5 (1)
- Science Goes Viral: Captivating Accounts of Science in Everyday LifeFrom EverandScience Goes Viral: Captivating Accounts of Science in Everyday LifeRating: 5 out of 5 stars5/5 (1)
- Chemistry: a QuickStudy Laminated Reference GuideFrom EverandChemistry: a QuickStudy Laminated Reference GuideRating: 5 out of 5 stars5/5 (1)
- The Periodic Table: A Very Short IntroductionFrom EverandThe Periodic Table: A Very Short IntroductionRating: 4.5 out of 5 stars4.5/5 (3)
- The Regenerative Grower's Guide to Garden Amendments: Using Locally Sourced Materials to Make Mineral and Biological Extracts and FermentsFrom EverandThe Regenerative Grower's Guide to Garden Amendments: Using Locally Sourced Materials to Make Mineral and Biological Extracts and FermentsRating: 5 out of 5 stars5/5 (3)
- The Elements We Live By: How Iron Helps Us Breathe, Potassium Lets Us See, and Other Surprising Superpowers of the Periodic TableFrom EverandThe Elements We Live By: How Iron Helps Us Breathe, Potassium Lets Us See, and Other Surprising Superpowers of the Periodic TableRating: 3.5 out of 5 stars3.5/5 (22)
- Stuff Matters: Exploring the Marvelous Materials That Shape Our Man-Made WorldFrom EverandStuff Matters: Exploring the Marvelous Materials That Shape Our Man-Made WorldRating: 4 out of 5 stars4/5 (289)
- Chemistry for Breakfast: The Amazing Science of Everyday LifeFrom EverandChemistry for Breakfast: The Amazing Science of Everyday LifeRating: 4.5 out of 5 stars4.5/5 (14)
- Gas-Liquid And Liquid-Liquid SeparatorsFrom EverandGas-Liquid And Liquid-Liquid SeparatorsRating: 3.5 out of 5 stars3.5/5 (3)
- Monkeys, Myths, and Molecules: Separating Fact from Fiction in the Science of Everyday LifeFrom EverandMonkeys, Myths, and Molecules: Separating Fact from Fiction in the Science of Everyday LifeRating: 4 out of 5 stars4/5 (9)
- Monkeys, Myths, and Molecules: Separating Fact from Fiction, and the Science of Everyday LifeFrom EverandMonkeys, Myths, and Molecules: Separating Fact from Fiction, and the Science of Everyday LifeRating: 4 out of 5 stars4/5 (1)
- Chemical Elements Pocket Guide: Detailed Summary of the Periodic TableFrom EverandChemical Elements Pocket Guide: Detailed Summary of the Periodic TableNo ratings yet