You might also like
- B-12-02861 KMT Blast Nozzles Catalog enDocument84 pagesB-12-02861 KMT Blast Nozzles Catalog enSankar KrishnanNo ratings yet
- Nikon Photographers Handbook 2016 Uk1129Document224 pagesNikon Photographers Handbook 2016 Uk1129iljan100% (2)
- Countdown Timers For PowerPointDocument21 pagesCountdown Timers For PowerPointArgo VirgiawanNo ratings yet
- R Language PDFDocument619 pagesR Language PDFShivam TanejaNo ratings yet
- FILE 20201025 102828 Public.1594882803..steam-Turbine-Overview-2019 PDFDocument45 pagesFILE 20201025 102828 Public.1594882803..steam-Turbine-Overview-2019 PDFNGUYEN QUANGNo ratings yet
- Generator Relay Protection Setting Calculation REV 1.0Document18 pagesGenerator Relay Protection Setting Calculation REV 1.0SreekanthMylavarapu100% (1)
- English: Quarter 2 - Module 3: Comparing and Contrasting The Same Topics in Different Multimodal TextsDocument13 pagesEnglish: Quarter 2 - Module 3: Comparing and Contrasting The Same Topics in Different Multimodal TextsLUCINO JR VALMORES100% (1)
- Googel Calendar Test CaseDocument6 pagesGoogel Calendar Test CaseJyotidesai25% (4)
- Clinical Informatics Literacy: 5000 Concepts That Every Informatician Should KnowFrom EverandClinical Informatics Literacy: 5000 Concepts That Every Informatician Should KnowNo ratings yet
- Seminar ReportDocument19 pagesSeminar ReportrenjithjamesNo ratings yet
- Articulo JDocument15 pagesArticulo JPercy QuispeNo ratings yet
- A Secure Cloud-Based Patient Electronic Medical Records System Using Two-Factor AuthenticationDocument6 pagesA Secure Cloud-Based Patient Electronic Medical Records System Using Two-Factor AuthenticationInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Patient Health Management System Using E-Health Monitoring ArchitectureDocument7 pagesPatient Health Management System Using E-Health Monitoring Architecturejayesh tahasildarNo ratings yet
- 1 s2.0 S016740482030239X MainDocument20 pages1 s2.0 S016740482030239X MainHanNo ratings yet
- Health Information Privacy and SecurityDocument9 pagesHealth Information Privacy and SecurityHafsa AkhtarNo ratings yet
- Research Paper in ProcessDocument9 pagesResearch Paper in ProcessakanshaNo ratings yet
- Smart HealthcareDocument9 pagesSmart HealthcareRohit RajNo ratings yet
- Security and Privacy-Preserving Challenges of E-Health Solutions in Cloud ComputingDocument22 pagesSecurity and Privacy-Preserving Challenges of E-Health Solutions in Cloud ComputingfardzlyNo ratings yet
- Proposed System Using Iot and Gis To Generate Electronic Medical RecordsDocument11 pagesProposed System Using Iot and Gis To Generate Electronic Medical Recordsindex PubNo ratings yet
- Securing The E-Health CloudDocument11 pagesSecuring The E-Health CloudfardzlyNo ratings yet
- Serum (Major)Document10 pagesSerum (Major)habaga6016No ratings yet
- Implementing A Personal Health Record Cloud Platform Using Ciphertext-Policy Attribute-Based EncryptionDocument8 pagesImplementing A Personal Health Record Cloud Platform Using Ciphertext-Policy Attribute-Based EncryptionAyeni AyomideNo ratings yet
- Handling Privacy-Sensitive Medical Data With Federated Learning: Challenges and Future DirectionsDocument14 pagesHandling Privacy-Sensitive Medical Data With Federated Learning: Challenges and Future DirectionsAfrin IbrahimNo ratings yet
- Securing The Ehealth CloudDocument10 pagesSecuring The Ehealth CloudFirdausNo ratings yet
- Hgrid: An Economical Model For Mass-Health Care System Using Latest Technology (Grid Computing)Document5 pagesHgrid: An Economical Model For Mass-Health Care System Using Latest Technology (Grid Computing)IJMERNo ratings yet
- E-AMBULANCE: Real-Time Integration Platform For Heterogeneous Medical Telemetry SystemDocument8 pagesE-AMBULANCE: Real-Time Integration Platform For Heterogeneous Medical Telemetry SystemNourhene EllouzeNo ratings yet
- Ijet V3i6p2Document6 pagesIjet V3i6p2International Journal of Engineering and TechniquesNo ratings yet
- Name:: Mohammad Khamis BalochiDocument7 pagesName:: Mohammad Khamis BalochiNaveed Akhtar BalochNo ratings yet
- Report Task2 MohammadDocument7 pagesReport Task2 MohammadNaveed Akhtar BalochNo ratings yet
- Health Big Data Analytics: A Technology SurveyDocument18 pagesHealth Big Data Analytics: A Technology SurveyRitesh SharmaNo ratings yet
- Good For NextDocument13 pagesGood For NextKrishna Prasad SatamrajuNo ratings yet
- Poh 2014Document6 pagesPoh 2014karanNo ratings yet
- Individual AssignmentDocument13 pagesIndividual AssignmentLife of LokiniNo ratings yet
- L3 Overview of Health InformaticsDocument3 pagesL3 Overview of Health InformaticsVera June RañesesNo ratings yet
- Individual AssignmentDocument12 pagesIndividual AssignmentLife of LokiniNo ratings yet
- Patient Record TrackingDocument85 pagesPatient Record TrackingMajestyNo ratings yet
- AmirLatif2020 Article ARemixIDESmartContract-basedFrDocument24 pagesAmirLatif2020 Article ARemixIDESmartContract-basedFrDivya KandpalNo ratings yet
- A Survey On The Roles of Communication Technologies in IoT-Based Personalized Healthcare ApplicationsDocument21 pagesA Survey On The Roles of Communication Technologies in IoT-Based Personalized Healthcare ApplicationsAlfi NgrNo ratings yet
- A Healthcare Monitoring System Using Random Forest & IOT (MTAP)Document12 pagesA Healthcare Monitoring System Using Random Forest & IOT (MTAP)Ahmed IqbalNo ratings yet
- 1C1-4 EPRSwDEaFPIDocument6 pages1C1-4 EPRSwDEaFPIAlunar HartNo ratings yet
- Final IS AssignmentDocument8 pagesFinal IS AssignmentThunder BangNo ratings yet
- Blockchain Based Storing and Sharing of Medical RecordDocument9 pagesBlockchain Based Storing and Sharing of Medical RecordIJRASETPublicationsNo ratings yet
- Blockchain For Giving Patients Control ODocument14 pagesBlockchain For Giving Patients Control OGreg ChatsiosNo ratings yet
- Bio IotDocument60 pagesBio Iotns saravananNo ratings yet
- Healthcare and Therefore The Internet of ThingsDocument7 pagesHealthcare and Therefore The Internet of Thingsrishabh arora rishabhNo ratings yet
- Chiuchisan 2015Document5 pagesChiuchisan 2015manthan joshiNo ratings yet
- Report On Ehr SystemDocument24 pagesReport On Ehr SystemRajesh KumarNo ratings yet
- Combining Blockchain and Iot For Decentralized Healthcare Data ManagementDocument16 pagesCombining Blockchain and Iot For Decentralized Healthcare Data ManagementJames MorenoNo ratings yet
- Keynote Paper: From Eda To Iot Ehealth: Promises, Challenges, and SolutionsDocument14 pagesKeynote Paper: From Eda To Iot Ehealth: Promises, Challenges, and SolutionsngovantamcuteNo ratings yet
- CAM: Cloud-Assisted Privacy Preserving Mobile Health MonitoringDocument13 pagesCAM: Cloud-Assisted Privacy Preserving Mobile Health MonitoringakttripathiNo ratings yet
- Importance of Cybersecurity in Electronic Health RecordsDocument5 pagesImportance of Cybersecurity in Electronic Health RecordsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Privacy in Electronic Health Records: A Systematic Mapping StudyDocument20 pagesPrivacy in Electronic Health Records: A Systematic Mapping StudyputriNo ratings yet
- Machine-Learning Approach For Predicting Harmful Diseases Using Big Data and IoT A ReviewDocument6 pagesMachine-Learning Approach For Predicting Harmful Diseases Using Big Data and IoT A ReviewIJRASETPublicationsNo ratings yet
- An Adaptive Role-Based Access Control Approach For Cloud E-Health SystemsDocument12 pagesAn Adaptive Role-Based Access Control Approach For Cloud E-Health SystemsGlobal Research and Development ServicesNo ratings yet
- Bio Final Report BTDocument15 pagesBio Final Report BTK NandanNo ratings yet
- Computers in Human Behavior: Kashif Saleem, Abdelouahid Derhab, Jalal Al-Muhtadi, Basit ShahzadDocument9 pagesComputers in Human Behavior: Kashif Saleem, Abdelouahid Derhab, Jalal Al-Muhtadi, Basit ShahzadvinjamurisivaNo ratings yet
- Literature Review On Patient Monitoring SystemDocument6 pagesLiterature Review On Patient Monitoring Systemc5rc7ppr100% (1)
- Health Record Using Block ChainDocument9 pagesHealth Record Using Block Chainroshini venkatNo ratings yet
- Base PaerDocument14 pagesBase PaerRitesh sharmaNo ratings yet
- Privacy Security and Resilience in Mobile Healthcare ApplicationsDocument16 pagesPrivacy Security and Resilience in Mobile Healthcare ApplicationsMUH.ALFIKRI TRI ANGGORO PAMUNGKASNo ratings yet
- Importance of Interoperability in HealthcareDocument4 pagesImportance of Interoperability in HealthcareInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Unified Patient Information System For Iraqi HospiDocument4 pagesUnified Patient Information System For Iraqi HospiMohammed nabelNo ratings yet
- Nikhil EportDocument25 pagesNikhil Eportbablu mokshagnaNo ratings yet
- Thesis On Electronic Medical RecordsDocument5 pagesThesis On Electronic Medical RecordsPayingSomeoneToWriteAPaperJackson100% (2)
- Official Lecture#4 - Overview of Health InformaticsDocument3 pagesOfficial Lecture#4 - Overview of Health InformaticsLYKA ANTONETTE ABREGANANo ratings yet
- 10 1145@2818869 2818889 PDFDocument6 pages10 1145@2818869 2818889 PDFDjamel JamelNo ratings yet
- 1 s2.0 S2214212623002053 MainDocument15 pages1 s2.0 S2214212623002053 MainDr. V. Padmavathi Associate ProfessorNo ratings yet
- Towards A Remote Monitoring of Patient Vital SignsDocument26 pagesTowards A Remote Monitoring of Patient Vital SignsWahid Hassan FuadNo ratings yet
- Which of The Following Is Not One of The Pillars of "The Well-Architected Framework" From Amazon?Document18 pagesWhich of The Following Is Not One of The Pillars of "The Well-Architected Framework" From Amazon?Nael SinganNo ratings yet
- Student Behavior That Leads To Energy Abuse: Case Study at A Teaching Institution in MalaysiaDocument9 pagesStudent Behavior That Leads To Energy Abuse: Case Study at A Teaching Institution in MalaysiafairusNo ratings yet
- KX-T30810B ManualDocument8 pagesKX-T30810B ManualHesham ElsayedNo ratings yet
- Qdoc - Tips Chap 3Document11 pagesQdoc - Tips Chap 3Jovana LazicNo ratings yet
- Inomax ACS580 VFD User Manual V220Document112 pagesInomax ACS580 VFD User Manual V220luis castiblanco100% (1)
- Chapter: Shift Registers Paper: Digital Systems and Applications Lesson Developer: Ms. Chanchal Yadav College: Rajdhani College, University of DelhiDocument39 pagesChapter: Shift Registers Paper: Digital Systems and Applications Lesson Developer: Ms. Chanchal Yadav College: Rajdhani College, University of DelhiMaxbuub AxmedNo ratings yet
- Application of GPS in Vehicular Traffic Management AssignmentDocument12 pagesApplication of GPS in Vehicular Traffic Management AssignmentVijisha SahooNo ratings yet
- VPython Help17Document1 pageVPython Help17hammouNo ratings yet
- Chuyên Phú ThọDocument12 pagesChuyên Phú Thọluhang1979No ratings yet
- LogDocument24 pagesLogcintapuspita2003No ratings yet
- Lieferanten-Selbstauskunft - Entwurf Messring enDocument4 pagesLieferanten-Selbstauskunft - Entwurf Messring enIonel ValceaNo ratings yet
- TOEFL Sample Practice Test 1 Reading Passage 2 Smart EnergyDocument3 pagesTOEFL Sample Practice Test 1 Reading Passage 2 Smart EnergyAilen ChoNo ratings yet
- Unique AppSites Data MiningDocument159 pagesUnique AppSites Data Miningintkhab khanNo ratings yet
- A New Material-Balance Equation For Naturally Fractured ReservoirsDocument9 pagesA New Material-Balance Equation For Naturally Fractured ReservoirsIgnacio Martinez SanchezNo ratings yet
- X-Band Solid-State Surface Movement Radar "ALCOR": PJSC "Almaz R&P Corp." Almaz-Antey ConcernDocument2 pagesX-Band Solid-State Surface Movement Radar "ALCOR": PJSC "Almaz R&P Corp." Almaz-Antey ConcernNapssNo ratings yet
- Policing The Net SketchDocument3 pagesPolicing The Net SketchBen BroughtonNo ratings yet
- Arjay Repaso Quiz ScienceDocument4 pagesArjay Repaso Quiz ScienceArjay RepasoNo ratings yet
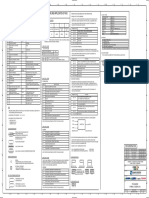
- CB2-M-ZEN-21-20003-P&ID - Symbol & Legend (33) - Rev.1Document1 pageCB2-M-ZEN-21-20003-P&ID - Symbol & Legend (33) - Rev.1ari wibowoNo ratings yet
- Final Students W SanctionsDocument39 pagesFinal Students W SanctionsJohn Gavin CarmenNo ratings yet
- Part-II-Substations Template - Q4Document19 pagesPart-II-Substations Template - Q4sadegaonkarNo ratings yet
- TAGWALK Menswear Fall - Winter 2021 Top Trends & DataDocument6 pagesTAGWALK Menswear Fall - Winter 2021 Top Trends & DataRafael PlataNo ratings yet
- Why Use A Distribution Block?: Power Distribution Terminal BlocksDocument2 pagesWhy Use A Distribution Block?: Power Distribution Terminal BlocksMark FernandezNo ratings yet