You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Hypovolemic Shock TEXTDocument5 pagesHypovolemic Shock TEXTrhen1991No ratings yet
- Dams Flash Cards PDFDocument315 pagesDams Flash Cards PDFKritika P SoroutNo ratings yet
- Grays Anatomy For Students 5th Edition 2023Document16 pagesGrays Anatomy For Students 5th Edition 2023AnandSreeNo ratings yet
- Pearls and Pitfalls in Emergency Radiology Variants and Other Difficult Diagnoses 2013Document389 pagesPearls and Pitfalls in Emergency Radiology Variants and Other Difficult Diagnoses 2013mmbire@gmail.comNo ratings yet
- Medical-Surgical NursingDocument16 pagesMedical-Surgical NursingMei Joy0% (1)
- Cardiogenic ShockDocument21 pagesCardiogenic ShockIslamOteshNo ratings yet
- Aiims - Pediatrics Q&ADocument207 pagesAiims - Pediatrics Q&AqqypprcyxyNo ratings yet
- Science - 9 - Learning MaterialsDocument438 pagesScience - 9 - Learning MaterialsEUGELYN G. PRESADO100% (1)
- NfiDocument41 pagesNfiKristine Singson0% (1)
- Jaffe Anesthesiologist Manual of Surgical ProcDocument50 pagesJaffe Anesthesiologist Manual of Surgical ProcHidayati IdaNo ratings yet
- Snakes (Ophidia) : Snakes Poisonous Non-PoisonousDocument7 pagesSnakes (Ophidia) : Snakes Poisonous Non-Poisonousssuhass243No ratings yet
- Second PrescriptionDocument6 pagesSecond Prescriptionssuhass243No ratings yet
- Lead (Shisha)Document7 pagesLead (Shisha)ssuhass243No ratings yet
- Periocarditis: A) Acute PericarditisDocument4 pagesPeriocarditis: A) Acute Pericarditisssuhass243No ratings yet
- Obstetrics Instruments: 1) Sims Speculum UsesDocument5 pagesObstetrics Instruments: 1) Sims Speculum Usesssuhass243No ratings yet
- Delta Wave - LITFL Medical Blog - ECG Library BasicsDocument9 pagesDelta Wave - LITFL Medical Blog - ECG Library BasicsLauraNo ratings yet
- Arterial Disorders: Arteriosclerosis & AtherosclerosisDocument28 pagesArterial Disorders: Arteriosclerosis & AtherosclerosisManuel Jacob YradNo ratings yet
- Firstaidbyessamsidqi 210313230642Document80 pagesFirstaidbyessamsidqi 210313230642Ni Cho LayyNo ratings yet
- Antiarrhythmic Drugs: Division of Cardiovascular Medicine Taipei Medical University-Wan-Fang HospitalDocument35 pagesAntiarrhythmic Drugs: Division of Cardiovascular Medicine Taipei Medical University-Wan-Fang HospitalHONGJYNo ratings yet
- Diet Heart MythDocument23 pagesDiet Heart MythΚυριακίδης ΚώσταςNo ratings yet
- Hypertension in PregnancyDocument34 pagesHypertension in PregnancyROY ALPHYNo ratings yet
- Ventricular Septal DefectDocument11 pagesVentricular Septal DefectFajar YuniftiadiNo ratings yet
- 11 - Cardiovascular Series of LecturesDocument161 pages11 - Cardiovascular Series of LecturesNickson OnchokaNo ratings yet
- Alternate Overlap Syndrome 2023Document64 pagesAlternate Overlap Syndrome 2023bonn maNo ratings yet
- WordRoot MedicalAbbreviationsDocument9 pagesWordRoot MedicalAbbreviationsJouriel Kristoffer GriarteNo ratings yet
- MedSurge HYPERCALCEMIADocument9 pagesMedSurge HYPERCALCEMIAArfela Joy Dela CruzNo ratings yet
- Nerves of The ForearmDocument60 pagesNerves of The ForearmHiruzaminNo ratings yet
- 05 Feb 100 MCQ Test NEETprep Test Series For NEET 2023 AspirantsDocument13 pages05 Feb 100 MCQ Test NEETprep Test Series For NEET 2023 Aspirantsnorah araujoNo ratings yet
- FinalDocument36 pagesFinalNirali GalaNo ratings yet
- B. Between Two Lobes: - Posses Fissure For Ligamentum Teres C. Right Lobe: Posses Which Is Related ToDocument50 pagesB. Between Two Lobes: - Posses Fissure For Ligamentum Teres C. Right Lobe: Posses Which Is Related ToJc GaldosNo ratings yet
- Chapter 4 ReviewerDocument5 pagesChapter 4 ReviewerOUR LADY OF FATIMA UNIVERSITY COLLEGENo ratings yet
- HCQ in COVIDDocument28 pagesHCQ in COVIDAppu EliasNo ratings yet
- Function Human HeartDocument13 pagesFunction Human Heartshyam_inkNo ratings yet
- MEDT 19 (Lec)Document17 pagesMEDT 19 (Lec)Erick PanganibanNo ratings yet
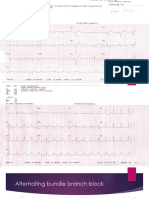
- Alternating Bundle Branch BlockDocument9 pagesAlternating Bundle Branch BlockSyifa Mahmud Syukran AkbarNo ratings yet