You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (843)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- N O I A N: AME Rigin Nsertion Ction ErveDocument16 pagesN O I A N: AME Rigin Nsertion Ction ErveJulie Brookelle Jacquinot100% (7)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Cupping Therapy NewDocument50 pagesCupping Therapy NewNikita Yadav100% (3)
- Bridgmans Complete Guide To Drawing From Life Over 1000 Illustrations-Sterling 2001 George B. BridgmanDocument346 pagesBridgmans Complete Guide To Drawing From Life Over 1000 Illustrations-Sterling 2001 George B. Bridgmankareem gunther100% (2)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Muscles of The Hand & WristDocument43 pagesMuscles of The Hand & WristWasemBhatNo ratings yet
- Rotator CuffDocument46 pagesRotator Cuffeuan00No ratings yet
- The Rotator Cuff PDFDocument201 pagesThe Rotator Cuff PDFjesussalvadorsuazaNo ratings yet
- Notes On Anatomy S N Kazi Final Shoretened CompressDocument206 pagesNotes On Anatomy S N Kazi Final Shoretened Compress147 -Ashfia Hashmi100% (1)
- AAOS Foot & Ankle 2015Document114 pagesAAOS Foot & Ankle 2015Fasa Roshada100% (3)
- Biomechanics of The ElbowDocument16 pagesBiomechanics of The ElbowAsmaa Ahmad SharawyNo ratings yet
- 12 Ways To Exercise Hands and FingersDocument6 pages12 Ways To Exercise Hands and FingersAri WidiyantoNo ratings yet
- I Ching Balance Method - Meridian & Point SelectionDocument1 pageI Ching Balance Method - Meridian & Point SelectionStuart LeNo ratings yet
- De Humani Corporis FabricaDocument13 pagesDe Humani Corporis FabricaMaykson CardosoNo ratings yet
- Deforming Force in Lower Limb Fracture FixDocument28 pagesDeforming Force in Lower Limb Fracture FixRizki Setiawan SultanNo ratings yet
- PDF The Muscular System Manual The Skeletal Muscles of The Human Body Joseph E Muscolino Ebook Full ChapterDocument53 pagesPDF The Muscular System Manual The Skeletal Muscles of The Human Body Joseph E Muscolino Ebook Full Chapterwarren.chesnut124No ratings yet
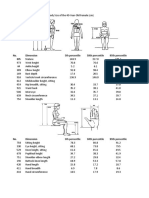
- Human Factors Data PDFDocument9 pagesHuman Factors Data PDFBalram JhaNo ratings yet
- Obaid Hip ExaminationDocument3 pagesObaid Hip ExaminationAlaa ElbulukNo ratings yet
- English Class 6T0 Sulannee AlejoDocument6 pagesEnglish Class 6T0 Sulannee AlejoSherlo DuranNo ratings yet
- Kelas 1 Sd-Mi Bab 5 Bahasa InggrisDocument3 pagesKelas 1 Sd-Mi Bab 5 Bahasa InggrisAnonymous AjkjNFees100% (1)
- Splints and Casts Indications and MethodsDocument9 pagesSplints and Casts Indications and MethodsJay GaneshNo ratings yet
- Common Errors in Xray Interpretation 2Document49 pagesCommon Errors in Xray Interpretation 2Shri RamaNo ratings yet
- (Mark D.miller) Review of Orthopaedics (5th Ed.)Document3 pages(Mark D.miller) Review of Orthopaedics (5th Ed.)Nauman ManzoorNo ratings yet
- Le Plexus BrachialDocument1 pageLe Plexus BrachialCarl-Eric TanoéNo ratings yet
- Upper Extremity Range of Motion: Erinda Rahma MuliaDocument25 pagesUpper Extremity Range of Motion: Erinda Rahma MuliaAdinda DianNo ratings yet
- 5 - ArthrologyDocument26 pages5 - Arthrologydrshubhamvyas.08No ratings yet
- Carpal Tunnel SyndromeDocument22 pagesCarpal Tunnel SyndromeNUR ZAMZAM AZIZAHNo ratings yet
- Teachings of Master Ott - WiktenauerDocument17 pagesTeachings of Master Ott - Wiktenauerdumpy56No ratings yet
- Chronic Lateral Elbow PainDocument62 pagesChronic Lateral Elbow Painloopy100No ratings yet
- Kin 3305 Knee PresentationDocument45 pagesKin 3305 Knee PresentationErrol TongcoNo ratings yet
- Badminton Injuries in Elite Athletes: A Review of Epidemiology and BiomechanicsDocument9 pagesBadminton Injuries in Elite Athletes: A Review of Epidemiology and BiomechanicsAmbusam SubramaniamNo ratings yet
- Aorta and Peripheral Arteries Anatomy VisualizationDocument71 pagesAorta and Peripheral Arteries Anatomy VisualizationSergiu HelciugNo ratings yet