You might also like
- Intestinal Ills Chronic Constipation, Indigestion, Autogenetic Poisons, Diarrhea, Piles, Etc. Also Auto-Infection, Auto-Intoxication, Anemia, Emaciation, Etc. Due to Proctitis and ColitisFrom EverandIntestinal Ills Chronic Constipation, Indigestion, Autogenetic Poisons, Diarrhea, Piles, Etc. Also Auto-Infection, Auto-Intoxication, Anemia, Emaciation, Etc. Due to Proctitis and ColitisNo ratings yet
- Calculation For Service Platform & Pump Shelter StructureDocument36 pagesCalculation For Service Platform & Pump Shelter Structuretrian33100% (1)
- Natural Antibiotics and Antivirals: Homemade Herbal Remedies that Kill Pathogens and Cure Bacterial Infections and Allergies. Prevent Illness, Cold and FluFrom EverandNatural Antibiotics and Antivirals: Homemade Herbal Remedies that Kill Pathogens and Cure Bacterial Infections and Allergies. Prevent Illness, Cold and FluNo ratings yet
- Fast Facts: Respiratory Allergies: Understand aeroallergens, improve treatment responseFrom EverandFast Facts: Respiratory Allergies: Understand aeroallergens, improve treatment responseNo ratings yet
- A Management and Leadership TheoriesDocument43 pagesA Management and Leadership TheoriesKrezielDulosEscobarNo ratings yet
- InfoVista Xeus Pro 5 TMR Quick GuideDocument76 pagesInfoVista Xeus Pro 5 TMR Quick GuideNguyen Dang KhanhNo ratings yet
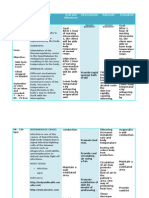
- VI. Nursing Care Plan Cues Nursing Diagnosis Analysis Goals and Objectives Intervention Rationale EvaluationDocument3 pagesVI. Nursing Care Plan Cues Nursing Diagnosis Analysis Goals and Objectives Intervention Rationale EvaluationJenny AjocNo ratings yet
- The Flu: A Guide for Prevention and TreatmentFrom EverandThe Flu: A Guide for Prevention and TreatmentRating: 5 out of 5 stars5/5 (1)
- NCM 112Document24 pagesNCM 112Amoroso, Marian Corneth D.No ratings yet
- Nursing Care Plan Typhoid FeverDocument2 pagesNursing Care Plan Typhoid Feverderic87% (68)
- NCP HyperthermiaDocument4 pagesNCP HyperthermiaKingJayson Pacman06No ratings yet
- Assessment Explanation of The Problem Objectives Nursing Interventions Rationale EvaluationDocument3 pagesAssessment Explanation of The Problem Objectives Nursing Interventions Rationale EvaluationAlyssa Moutrie Dulay Arabe100% (1)
- Com +Nursing+Care+Plan+Chicken+PoxDocument2 pagesCom +Nursing+Care+Plan+Chicken+PoxDahl Obañana Erojo100% (1)
- Nursing Care Plan: Subjective: Short Term IndependentDocument2 pagesNursing Care Plan: Subjective: Short Term IndependentKristine Young50% (2)
- Project Report On Amazon vs. FlipkartDocument86 pagesProject Report On Amazon vs. FlipkartDimple100% (3)
- NCP - HyperthermiaDocument2 pagesNCP - Hyperthermiagiadda91% (67)
- NURSING CARE PLAN Chicken PoxDocument2 pagesNURSING CARE PLAN Chicken Poxderic87% (62)
- B NCP On and Off Fever 2b ImproveddocxDocument6 pagesB NCP On and Off Fever 2b ImproveddocxKylie CatralNo ratings yet
- Assessment Nursing Diagnosis Planning Nursing Intervention Rationale Subjective Short Term IndependentDocument3 pagesAssessment Nursing Diagnosis Planning Nursing Intervention Rationale Subjective Short Term IndependentMoi Valdoz100% (1)
- TASk 2 DS NCPDocument3 pagesTASk 2 DS NCPCHRISTIAN CALAMBANo ratings yet
- Cues Nursing Diagnosis Scientific Rationale Objectives Intervention Rationale Evaluation IndependentDocument6 pagesCues Nursing Diagnosis Scientific Rationale Objectives Intervention Rationale Evaluation IndependentKasandra Dawn Moquia Beriso100% (1)
- Activity 1 - Case Agent RookieDocument2 pagesActivity 1 - Case Agent RookieChristian ConcepcionNo ratings yet
- Define Sepsis?: Ahmed Ba Elaian BSNDocument5 pagesDefine Sepsis?: Ahmed Ba Elaian BSNAhmad BaolayyanNo ratings yet
- NCP - Chicken PoxDocument4 pagesNCP - Chicken Poxhanna_lim0% (1)
- Assessment Nursing Diagnosis Nursing Analysis Planning Nursing Interventions Rationale EvaluationDocument2 pagesAssessment Nursing Diagnosis Nursing Analysis Planning Nursing Interventions Rationale EvaluationChristian ConcepcionNo ratings yet
- HW#4 PaharmacologyDocument5 pagesHW#4 PaharmacologyMICHAEL GABRIEL JIMENEZNo ratings yet
- NCM 101B - NCP - Miguel, Roenth Rhene D - BSN 1DDocument2 pagesNCM 101B - NCP - Miguel, Roenth Rhene D - BSN 1DRiri MiguelNo ratings yet
- Assessment Diagnosis Scientific Background Planning Intervention Rationale Evaluation Short Term: IndependentDocument2 pagesAssessment Diagnosis Scientific Background Planning Intervention Rationale Evaluation Short Term: IndependentNE TdrNo ratings yet
- Assessment Nursing Diagnosis Planning Implementation Rationale EvaluationDocument3 pagesAssessment Nursing Diagnosis Planning Implementation Rationale EvaluationChloie Marie RosalejosNo ratings yet
- Cues Nursing Diagnosis Background Knowledge Planning Intervention Rationale Evaluation Subjective DataDocument2 pagesCues Nursing Diagnosis Background Knowledge Planning Intervention Rationale Evaluation Subjective DataJordz PlaciNo ratings yet
- Hyperthermia Drug StudyDocument2 pagesHyperthermia Drug StudyTipey SegismundoNo ratings yet
- Assessment NCM 101Document1 pageAssessment NCM 101Lorainne Angel U. MolinaNo ratings yet
- NCPDocument2 pagesNCPJonna Mae TurquezaNo ratings yet
- Case Presentation (2023)Document17 pagesCase Presentation (2023)Infection QcghNo ratings yet
- Hypothermia: By: James Rod D. Marinduque and Jeanette T. DungcaDocument2 pagesHypothermia: By: James Rod D. Marinduque and Jeanette T. DungcaJAMES ROD MARINDUQUENo ratings yet
- Kawasaki Disease FinalDocument5 pagesKawasaki Disease FinalMarie Ashley Casia100% (1)
- Casia-Research Topic-Kawasaki SyndromeDocument10 pagesCasia-Research Topic-Kawasaki SyndromeMarie Ashley CasiaNo ratings yet
- Chicken Pox N C P BY BHERU LALDocument2 pagesChicken Pox N C P BY BHERU LALBheru Lal100% (1)
- Assessment Nursing Diagnosis Need Objective Interventions Evaluation Subjective Data: C O G N I T I V E - P E R C E P T U A L Goal MetDocument4 pagesAssessment Nursing Diagnosis Need Objective Interventions Evaluation Subjective Data: C O G N I T I V E - P E R C E P T U A L Goal MetAngel Mikaela CilladoNo ratings yet
- Assessment Diagnosis Inference Planning Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Inference Planning Intervention Rationale EvaluationMichelle Dona MirallesNo ratings yet
- SNU49Document2 pagesSNU49Nora BacolNo ratings yet
- HyperthermiaDocument6 pagesHyperthermiaBerlyn FelicianoNo ratings yet
- Subjective: "Sumikip Ang Dibdib Ko at Hindi Ako Makahinga NG Maayos" As IndependentDocument2 pagesSubjective: "Sumikip Ang Dibdib Ko at Hindi Ako Makahinga NG Maayos" As IndependentCorinneNo ratings yet
- Nursing Care Plan: Assessment Diagnosis Planning Implementation Rationale EvaluationDocument2 pagesNursing Care Plan: Assessment Diagnosis Planning Implementation Rationale EvaluationWinnie AriolaNo ratings yet
- Cor Jesu College, Inc., College of Health Sciences Sto. Rosario, Tres de Mayo, Digos CityDocument8 pagesCor Jesu College, Inc., College of Health Sciences Sto. Rosario, Tres de Mayo, Digos City2BGrp3Plaza, Anna MaeNo ratings yet
- Apalisok NCPDocument3 pagesApalisok NCPApalisok GerardNo ratings yet
- SNU49Document2 pagesSNU49Nora BacolNo ratings yet
- Nursing InterventionsDocument37 pagesNursing InterventionsRajalakshmi100% (1)
- Hyperthermia Related To Dengue Fever As Evidenced by Temperature Above The Normal RangeDocument2 pagesHyperthermia Related To Dengue Fever As Evidenced by Temperature Above The Normal RangeAlyssa marieNo ratings yet
- Cues and Evidences Nursing Diagnosis Objectives Interventions Rationale EvaluationDocument2 pagesCues and Evidences Nursing Diagnosis Objectives Interventions Rationale EvaluationJade GordoncilloNo ratings yet
- Nursing Care PlanDocument3 pagesNursing Care PlanAnnahNo ratings yet
- Assessment Diagnosis Planning Interventions Rationale Evaluation IndependentDocument2 pagesAssessment Diagnosis Planning Interventions Rationale Evaluation IndependentFau Fau DheoboNo ratings yet
- Assessment Diagnosis Planning Intervention Evauation IndependentDocument2 pagesAssessment Diagnosis Planning Intervention Evauation IndependentCHRISTIAN CALAMBANo ratings yet
- Nursingcrib Com NURSING CARE PLAN Chicken Pox PDFDocument2 pagesNursingcrib Com NURSING CARE PLAN Chicken Pox PDFAkeroNo ratings yet
- Cues Nursing Diagnos IS Analysis Planning Intervention Rationale EvaluationDocument7 pagesCues Nursing Diagnos IS Analysis Planning Intervention Rationale EvaluationLoriejae Marie DesulocNo ratings yet
- NCP 3rd YearDocument6 pagesNCP 3rd YearTotoro AblogNo ratings yet
- Family Nursing Care Plan For FeverDocument2 pagesFamily Nursing Care Plan For Feverbharat singhNo ratings yet
- Brain Tumor ManuscriptDocument7 pagesBrain Tumor Manuscripteliza luisNo ratings yet
- Q-fever, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandQ-fever, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Legionellosis, (Legionnaire Disease) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandLegionellosis, (Legionnaire Disease) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- NonmodifiableDocument4 pagesNonmodifiableAmoroso, Marian Corneth D.No ratings yet
- Iv Sheets, NN, VSDocument4 pagesIv Sheets, NN, VSAmoroso, Marian Corneth D.No ratings yet
- Renal FailureDocument5 pagesRenal FailureAmoroso, Marian Corneth D.No ratings yet
- Bulimia NervosaDocument19 pagesBulimia NervosaAmoroso, Marian Corneth D.No ratings yet
- Acute PancreatitisDocument31 pagesAcute PancreatitisAmoroso, Marian Corneth D.No ratings yet
- Logic of JudgementDocument11 pagesLogic of JudgementAmoroso, Marian Corneth D.No ratings yet
- Case Presentation: March 11, 2023Document14 pagesCase Presentation: March 11, 2023Amoroso, Marian Corneth D.No ratings yet
- Gerd and Hiatal HerniaDocument4 pagesGerd and Hiatal HerniaAmoroso, Marian Corneth D.No ratings yet
- Pneumonia Apollo SimulationDocument2 pagesPneumonia Apollo SimulationAmoroso, Marian Corneth D.No ratings yet
- Gigantism and AcromegalyDocument5 pagesGigantism and AcromegalyAmoroso, Marian Corneth D.No ratings yet
- Cushing SyndromeDocument12 pagesCushing SyndromeAmoroso, Marian Corneth D.No ratings yet
- ANATOMY AND PHYSIOLOGY of ADRENAL GLANDS AND SIADH & DIDocument9 pagesANATOMY AND PHYSIOLOGY of ADRENAL GLANDS AND SIADH & DIAmoroso, Marian Corneth D.No ratings yet
- Anatomy & Physiology: CRH ActhDocument6 pagesAnatomy & Physiology: CRH ActhAmoroso, Marian Corneth D.No ratings yet
- Pregnancy ComplicationsDocument2 pagesPregnancy ComplicationsAmoroso, Marian Corneth D.No ratings yet
- Stages of LaborDocument3 pagesStages of LaborAmoroso, Marian Corneth D.No ratings yet
- CATARACTS and GLAUCOMADocument11 pagesCATARACTS and GLAUCOMAAmoroso, Marian Corneth D.No ratings yet
- A. Discuss The Four Stages of LaborDocument3 pagesA. Discuss The Four Stages of LaborAmoroso, Marian Corneth D.No ratings yet
- Customer AnalysisDocument6 pagesCustomer AnalysisLina LambotNo ratings yet
- SKI Report2008 - 50 2Document46 pagesSKI Report2008 - 50 2nada safitriNo ratings yet
- Appendix H Sample of Coded Transcript PDFDocument21 pagesAppendix H Sample of Coded Transcript PDFWahib LahnitiNo ratings yet
- 3658 - Implement Load BalancingDocument6 pages3658 - Implement Load BalancingDavid Hung NguyenNo ratings yet
- Gallery IsKCON Desire Tree PDF MudrasDocument2 pagesGallery IsKCON Desire Tree PDF MudrassanatanNo ratings yet
- Hydrozirconation - Final 0Document11 pagesHydrozirconation - Final 0David Tritono Di BallastrossNo ratings yet
- Biology Chapter 23.1Document2 pagesBiology Chapter 23.1Carlos Enrique Altamar BorjaNo ratings yet
- Financial Vs Health and Safety Vs Reputation Vs Opportunity CostsDocument11 pagesFinancial Vs Health and Safety Vs Reputation Vs Opportunity Costschanlego123No ratings yet
- Stephen Law Morality Without GodDocument9 pagesStephen Law Morality Without GodJiReH MeCuaNo ratings yet
- AC2104 - Seminar 5Document3 pagesAC2104 - Seminar 5Rachel LiuNo ratings yet
- Berms For Stablizing Earth Retaining Structures: Youssef Gomaa Youssef Morsi B.SC., Civil EngineeringDocument212 pagesBerms For Stablizing Earth Retaining Structures: Youssef Gomaa Youssef Morsi B.SC., Civil EngineeringChan KNo ratings yet
- Chem31.1 Experiment 2Document28 pagesChem31.1 Experiment 2Mia FernandezNo ratings yet
- Consolidated PCU Labor Law Review 1st Batch Atty Jeff SantosDocument36 pagesConsolidated PCU Labor Law Review 1st Batch Atty Jeff SantosJannah Mae de OcampoNo ratings yet
- Dwnload Full Conceptual Physics 12th Edition Hewitt Test Bank PDFDocument36 pagesDwnload Full Conceptual Physics 12th Edition Hewitt Test Bank PDFscreamsoaring.pm7hcv100% (13)
- Pemphigus Subtypes Clinical Features Diagnosis andDocument23 pagesPemphigus Subtypes Clinical Features Diagnosis andAnonymous bdFllrgorzNo ratings yet
- National ScientistDocument2 pagesNational ScientistHu T. BunuanNo ratings yet
- Final BasantDocument22 pagesFinal BasantMuqaddas IsrarNo ratings yet
- History of AIDocument27 pagesHistory of AImuzammalNo ratings yet
- Ch3 Review QuestionsDocument15 pagesCh3 Review Questionsave estillerNo ratings yet
- Mohd Ali 17: By:-Roll NoDocument12 pagesMohd Ali 17: By:-Roll NoMd AliNo ratings yet
- Microsoft Official Course: Installing and Configuring Windows Server 2012Document18 pagesMicrosoft Official Course: Installing and Configuring Windows Server 2012jttodorovNo ratings yet
- The Palatability, and Potential Toxicity of Australian Weeds To GoatsDocument163 pagesThe Palatability, and Potential Toxicity of Australian Weeds To Goatsalshokairsaad513No ratings yet
- Effect of Employee Loyalty On Customer S PDFDocument37 pagesEffect of Employee Loyalty On Customer S PDFShailendra DasariNo ratings yet
- Item Bank - Science 5 - 2ND QuarterDocument11 pagesItem Bank - Science 5 - 2ND QuarterJasmine AguilaNo ratings yet
- Consumer Trend Canvas (CTC) Template 2022Document1 pageConsumer Trend Canvas (CTC) Template 2022Patricia DominguezNo ratings yet