You might also like
- Mental Health, Intellectual and Developmental Disabilities and the Ageing ProcessFrom EverandMental Health, Intellectual and Developmental Disabilities and the Ageing ProcessNo ratings yet
- Factors That Promote Remission in Individuals With SchizophreniaDocument16 pagesFactors That Promote Remission in Individuals With SchizophreniaFernando Yoga AlonsoNo ratings yet
- The F-Words' in Childhood Disability - I Swear This IsDocument7 pagesThe F-Words' in Childhood Disability - I Swear This IsPavel Antonovich Cuevas ZhbankovNo ratings yet
- Children 09 00091 v4Document17 pagesChildren 09 00091 v4Random PersonNo ratings yet
- Autoestima Pacientes Con OrtodonciaDocument6 pagesAutoestima Pacientes Con OrtodonciaAndres CoboNo ratings yet
- Physical Health of Adults with Intellectual and Developmental DisabilitiesFrom EverandPhysical Health of Adults with Intellectual and Developmental DisabilitiesNo ratings yet
- Hal 6 TranslatedDocument2 pagesHal 6 TranslatedsarahsaNo ratings yet
- 10 1016@j PMR 2019 07 012Document11 pages10 1016@j PMR 2019 07 012Sukandriani UtamiNo ratings yet
- Develop Med Child Neuro - 2009 - WATERS - Quality of life instruments for children and adolescents with neurodisabilitiesDocument10 pagesDevelop Med Child Neuro - 2009 - WATERS - Quality of life instruments for children and adolescents with neurodisabilitiesCalin PirvaNo ratings yet
- LX20221217-403 - Meta Analysis HealthcareDocument8 pagesLX20221217-403 - Meta Analysis HealthcareHumaira NasirNo ratings yet
- Helping Children and Adolescents with Chronic and Serious Medical Conditions: A Strengths-Based ApproachFrom EverandHelping Children and Adolescents with Chronic and Serious Medical Conditions: A Strengths-Based ApproachNo ratings yet
- Self-Concept and Self-Esteem Among Children and Young Adults With Visual Impairment A Systematic ReviewDocument13 pagesSelf-Concept and Self-Esteem Among Children and Young Adults With Visual Impairment A Systematic ReviewMădălina MarincaşNo ratings yet
- Inquiries, Investigation and ImmersionDocument7 pagesInquiries, Investigation and ImmersionAngel Erica TabigueNo ratings yet
- ICF: A Hands-on Approach for Clinicians and FamiliesFrom EverandICF: A Hands-on Approach for Clinicians and FamiliesOlaf Kraus de CamargoNo ratings yet
- Diagnosis To Function: Classification For Children and YouthsDocument8 pagesDiagnosis To Function: Classification For Children and YouthsVe SaNo ratings yet
- Mental Institution Research PaperDocument4 pagesMental Institution Research Paperixevojrif100% (1)
- Children's Perceptions of Health and Illness in PreadolescenceDocument11 pagesChildren's Perceptions of Health and Illness in PreadolescenceMarisol Rojas JaramilloNo ratings yet
- Labanza, Rain Raven B-2-1Document7 pagesLabanza, Rain Raven B-2-1RAIN RAVEN LABANZANo ratings yet
- Journal - Pone.0290653 1Document26 pagesJournal - Pone.0290653 1U of T MedicineNo ratings yet
- Free Research Papers On Mental IllnessDocument5 pagesFree Research Papers On Mental Illnesssvfziasif100% (1)
- RRLDocument4 pagesRRLMark CornejoNo ratings yet
- An Evaluation of The Overall Utility of Measures of Functioning Suitable For School-Aged Children On The Autism Spectrum: A Scoping ReviewDocument29 pagesAn Evaluation of The Overall Utility of Measures of Functioning Suitable For School-Aged Children On The Autism Spectrum: A Scoping ReviewHaytham Mumtaze NabulsyNo ratings yet
- The stress can be unbearable, but the good times are like finding gold”: A phase one modelling survey to inform the development of a self-help positive reappraisal coping intervention for caregivers of those with autism spectrum disorderDocument18 pagesThe stress can be unbearable, but the good times are like finding gold”: A phase one modelling survey to inform the development of a self-help positive reappraisal coping intervention for caregivers of those with autism spectrum disorderSham ObaidatNo ratings yet
- 1 s2.0 S193665741830253X MainDocument10 pages1 s2.0 S193665741830253X MainnadaNo ratings yet
- Ijerph 18 04091Document13 pagesIjerph 18 04091Ricardo Martín MoyaNo ratings yet
- 1978 Vol 1Document41 pages1978 Vol 1najwa faeizahNo ratings yet
- Perception and Psychosocial Burden of People With Epilepsy (PWE) : Experience From IndonesiaDocument4 pagesPerception and Psychosocial Burden of People With Epilepsy (PWE) : Experience From IndonesiaElna NurjannahNo ratings yet
- Foreign LiteratureDocument3 pagesForeign LiteraturemhonyitaNo ratings yet
- Best Ch1 Understanding Individuals With Physical Health and Multiple DisabilitiesDocument25 pagesBest Ch1 Understanding Individuals With Physical Health and Multiple DisabilitiesMarkoNo ratings yet
- Mental Health Problems Among Young People-A Scoping Review of Help SeekingDocument15 pagesMental Health Problems Among Young People-A Scoping Review of Help SeekingKarylle Yesha DomingoNo ratings yet
- Lundvall 2018Document8 pagesLundvall 2018Gummo bfsNo ratings yet
- Psychol Psychother - 2023 - Kitchen - Barriers and Enablers For Young People Parents and Therapists Undertaking 1Document21 pagesPsychol Psychother - 2023 - Kitchen - Barriers and Enablers For Young People Parents and Therapists Undertaking 1U of T MedicineNo ratings yet
- Care for Seniors by Family Health ProfessionalsDocument7 pagesCare for Seniors by Family Health Professionalsmarcelo3No ratings yet
- The GP Curriculum and Cerebral PalsyDocument9 pagesThe GP Curriculum and Cerebral PalsyFiaNo ratings yet
- Multidisciplinary Teamwork in Autism: Can One Size Fit All?: Karola DillenburgerDocument17 pagesMultidisciplinary Teamwork in Autism: Can One Size Fit All?: Karola DillenburgerMoustafa AbdouNo ratings yet
- Pittsburgh Ku Ferolie Aff Texas Round1Document15 pagesPittsburgh Ku Ferolie Aff Texas Round1jim tannerNo ratings yet
- Foundations of Professional Psychology: The End of Theoretical Orientations and the Emergence of the Biopsychosocial ApproachFrom EverandFoundations of Professional Psychology: The End of Theoretical Orientations and the Emergence of the Biopsychosocial ApproachNo ratings yet
- A Review of Mental Health Literacy Strategy For AdolescenceDocument7 pagesA Review of Mental Health Literacy Strategy For AdolescenceIJPHSNo ratings yet
- Journal Article ReviewDocument3 pagesJournal Article ReviewElyssa LeonardoNo ratings yet
- Empathy: The Legacy of Altruism in Health Care: The Promotion of Empathy, Prosociality and HumanismDocument9 pagesEmpathy: The Legacy of Altruism in Health Care: The Promotion of Empathy, Prosociality and HumanismWilmer Del Castillo MorilloNo ratings yet
- Quality of Life in Persons With Intellectual Disabilities and Mental Health Problems: An Explorative StudyDocument9 pagesQuality of Life in Persons With Intellectual Disabilities and Mental Health Problems: An Explorative StudyRaquelMaiaNo ratings yet
- Establishing Priorities For Psychological Interventions in Pediatric Settings: A Decision - Tree Approach Using The DISABKIDS-10 Index As A Screening InstrumentDocument15 pagesEstablishing Priorities For Psychological Interventions in Pediatric Settings: A Decision - Tree Approach Using The DISABKIDS-10 Index As A Screening InstrumentAndrade GuiNo ratings yet
- Child and Parent Perspectives of Life Quality of Children With Physical Impairments Compared With Non Disabled PeersDocument10 pagesChild and Parent Perspectives of Life Quality of Children With Physical Impairments Compared With Non Disabled Peerssocmed gistiNo ratings yet
- Chapter 1 second -WPS OfficeDocument2 pagesChapter 1 second -WPS Officejovelyntaming2No ratings yet
- Globalna Perspektiva AutizmaDocument7 pagesGlobalna Perspektiva AutizmaJohn SmithNo ratings yet
- Dentist training virtues of alterity and empathyDocument10 pagesDentist training virtues of alterity and empathyMeilisa RachmawatiNo ratings yet
- Labelling ReadingDocument22 pagesLabelling ReadingJack UptonNo ratings yet
- Disability Law Project.Document14 pagesDisability Law Project.mohitNo ratings yet
- Adolescent Health Interventions: Conclusions, Evidence Gaps, and Research PrioritiesDocument5 pagesAdolescent Health Interventions: Conclusions, Evidence Gaps, and Research PrioritiesMutya FebrianiNo ratings yet
- Self-Care As A Health Resource of Elders: An Integrative Review of The ConceptDocument11 pagesSelf-Care As A Health Resource of Elders: An Integrative Review of The ConceptJoaoNo ratings yet
- Loneliness in Older Adults: Effects, Prevention, and TreatmentFrom EverandLoneliness in Older Adults: Effects, Prevention, and TreatmentNo ratings yet
- A Study On Mental Health Literacy Among College StudentsDocument5 pagesA Study On Mental Health Literacy Among College StudentsEditor IJTSRDNo ratings yet
- Μαδιανός Attitudes Mental IllnessDocument13 pagesΜαδιανός Attitudes Mental IllnessGiorgos GritzelasNo ratings yet
- Professional Identity TransFormation in Medical EducationDocument6 pagesProfessional Identity TransFormation in Medical EducationDaniel QuirogaNo ratings yet
- Brady - Mental Health Resilience and Existential LiteratureDocument10 pagesBrady - Mental Health Resilience and Existential LiteratureNenad VujosevicNo ratings yet
- Cerebral Palsy: From Diagnosis to Adult LifeFrom EverandCerebral Palsy: From Diagnosis to Adult LifeRating: 5 out of 5 stars5/5 (3)
- Case Study AdolescentDocument27 pagesCase Study AdolescentAnna Larita100% (2)
- Resilience and Protective Factors Among Refugee Children Post-Migration To High-Income CountriesDocument8 pagesResilience and Protective Factors Among Refugee Children Post-Migration To High-Income Countriesjuniki.mariaNo ratings yet
- Mapping The Evidence of ExperiencesDocument7 pagesMapping The Evidence of ExperiencesWeronika GranthamNo ratings yet
- Mapping The Evidence of ExperiencesDocument7 pagesMapping The Evidence of ExperiencesWeronika GranthamNo ratings yet
- The Effectiveness of Regular Exercise Programs in The Prevention of Gestational Diabetes Mellitus-A Systematic ReviewDocument11 pagesThe Effectiveness of Regular Exercise Programs in The Prevention of Gestational Diabetes Mellitus-A Systematic ReviewWeronika GranthamNo ratings yet
- Dancing My Scoliosis An Autoethnography of Healing From Bodily Doubt Through Somatic PracticesDocument18 pagesDancing My Scoliosis An Autoethnography of Healing From Bodily Doubt Through Somatic PracticesWeronika GranthamNo ratings yet
- Dancing My Scoliosis An Autoethnography of Healing From Bodily Doubt Through Somatic PracticesDocument18 pagesDancing My Scoliosis An Autoethnography of Healing From Bodily Doubt Through Somatic PracticesWeronika GranthamNo ratings yet
- l3 Immunization & Cold ChainDocument53 pagesl3 Immunization & Cold ChainNur AinaaNo ratings yet
- Joyce2016 PDFDocument13 pagesJoyce2016 PDFAffan ArrizqiNo ratings yet
- Lead and Manage Team Effectiveness for BSBWOR502Document38 pagesLead and Manage Team Effectiveness for BSBWOR502roopaNo ratings yet
- Royal Scythians and the Slave Trade in HerodotusDocument19 pagesRoyal Scythians and the Slave Trade in HerodotusSinan SakicNo ratings yet
- Review of Esu Yoruba God Power and The IDocument7 pagesReview of Esu Yoruba God Power and The IBoris MilovicNo ratings yet
- Emotion-WPS OfficeDocument2 pagesEmotion-WPS OfficemikaNo ratings yet
- Labor Law 1 Class NotesDocument20 pagesLabor Law 1 Class Notescmv mendozaNo ratings yet
- MSDS Hygisoft Surface Disinfectant, Concentrate - PagesDocument5 pagesMSDS Hygisoft Surface Disinfectant, Concentrate - PagesDr. Omar Al-AbbasiNo ratings yet
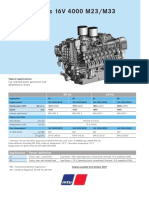
- Diesel Engines 16V 4000 M23/M33: 50 HZ 60 HZDocument2 pagesDiesel Engines 16V 4000 M23/M33: 50 HZ 60 HZAlberto100% (1)
- USD - DPF Cleaning Machine - POSEYDON1000 - PolDocument8 pagesUSD - DPF Cleaning Machine - POSEYDON1000 - PolAbaidi RabieNo ratings yet
- Se Lab Da-2Document12 pagesSe Lab Da-2Anvesh PenkeNo ratings yet
- How The Voice Works HandoutDocument7 pagesHow The Voice Works HandoutMatthew ColleyNo ratings yet
- STPDocument32 pagesSTPvishakha_rm2000No ratings yet
- Our Lady of Consolation Orchestra InstrumentsDocument2 pagesOur Lady of Consolation Orchestra InstrumentsCelestian Valensario PaderangaNo ratings yet
- The Merchant of Venice QuestionsDocument9 pagesThe Merchant of Venice QuestionsHaranath Babu50% (4)
- Down Syndrome Research PaperDocument11 pagesDown Syndrome Research Paperapi-299871292100% (1)
- PT JayatamaDocument67 pagesPT JayatamaAminadap. SIL.TNo ratings yet
- Communication Strategy Target AudienceDocument47 pagesCommunication Strategy Target Audienceguille simariNo ratings yet
- Elitox PPT ENG CompressedDocument18 pagesElitox PPT ENG CompressedTom ArdiNo ratings yet
- ACCT250-Auditing Course OutlineDocument7 pagesACCT250-Auditing Course OutlineammadNo ratings yet
- Unit 2 - LISDocument24 pagesUnit 2 - LISThục Anh NguyễnNo ratings yet
- Not Qualified (Spoken Word Poem) by JonJorgensonDocument3 pagesNot Qualified (Spoken Word Poem) by JonJorgensonKent Bryan Anderson100% (1)
- Ky203817 PSRPT 2022-05-17 14.39.33Document8 pagesKy203817 PSRPT 2022-05-17 14.39.33Thuy AnhNo ratings yet
- IN SUNNY SPAIN, 1882-85: "My Country, My Love, My People, I Leave You Now, You Disappear, I Lose Sight of You"Document4 pagesIN SUNNY SPAIN, 1882-85: "My Country, My Love, My People, I Leave You Now, You Disappear, I Lose Sight of You"Mary Claire ComalaNo ratings yet
- MgstreamDocument2 pagesMgstreamSaiful ManalaoNo ratings yet
- PassportDocument4 pagesPassportVijai Abraham100% (1)
- MSc Thesis on VAW in PhilippinesDocument100 pagesMSc Thesis on VAW in Philippineselma cutamoraNo ratings yet
- Kepler's ProblemDocument21 pagesKepler's ProblemGustavo MiasatoNo ratings yet
- National Geographic USA - 01 2019Document145 pagesNational Geographic USA - 01 2019Minh ThuNo ratings yet
- Are The Risk Management Tools at Your Law Firm Working?Document17 pagesAre The Risk Management Tools at Your Law Firm Working?vantoffNo ratings yet