You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- English For NursesDocument166 pagesEnglish For NursesAlexandrutza IuliaNo ratings yet
- Preanesthetic Assessment of Cardiac Patients UndDocument42 pagesPreanesthetic Assessment of Cardiac Patients UndParvathy R NairNo ratings yet
- Suicidio ArenasDocument26 pagesSuicidio ArenasJuan InsignaresNo ratings yet
- Genetic Engineering and The SocietyDocument25 pagesGenetic Engineering and The SocietyKrischanSayloGelasan100% (1)
- A6. Nutrition and Elimination - LT 2Document39 pagesA6. Nutrition and Elimination - LT 2Vincent JadolNo ratings yet
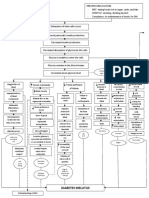
- Diabetes Mellitus: Hyperglycemia (304 MG/DL, 13.2 MG/DL)Document3 pagesDiabetes Mellitus: Hyperglycemia (304 MG/DL, 13.2 MG/DL)John Henry ValenciaNo ratings yet
- Veterinary Dermatology - 2021 - MuellerDocument20 pagesVeterinary Dermatology - 2021 - MuellerMandycat75No ratings yet
- Agc332 Exam June 2019Document3 pagesAgc332 Exam June 2019Solomon MbeweNo ratings yet
- Jurnal Case Control UTS (Idrus) 5Document8 pagesJurnal Case Control UTS (Idrus) 5Reny NapitupuluNo ratings yet
- RLE-level-2-packet-week-12-requirement (SANAANI, NUR-FATIMA, M.)Document26 pagesRLE-level-2-packet-week-12-requirement (SANAANI, NUR-FATIMA, M.)Nur SanaaniNo ratings yet
- History of Abnormal Psychology Chap 2Document20 pagesHistory of Abnormal Psychology Chap 2ahmadNo ratings yet
- Respi HemaDocument57 pagesRespi Hemaniczdelosreyes8No ratings yet
- Mythos World Resources Vol 1Document20 pagesMythos World Resources Vol 1Dániel Sebestyén100% (1)
- Heat Illnes Ped Rev 2019Document13 pagesHeat Illnes Ped Rev 2019Sandra A. Sánchez GarcíaNo ratings yet
- Komplikasi Ginjal Dan HipertensiDocument8 pagesKomplikasi Ginjal Dan HipertensiEna ElisaNo ratings yet
- Has Kahlbaum Syndrome Disappeared or Is It Underdiagnosed? Reexamining The Nosology of CatatoniaDocument3 pagesHas Kahlbaum Syndrome Disappeared or Is It Underdiagnosed? Reexamining The Nosology of CatatoniaMariano OutesNo ratings yet
- ANNEX 2m Guidelines On Home Monitoring and Clinical Protocol at Primary Care For Cat 1 and 2 Mild Confirmed COVID-19 Cases 02122021Document57 pagesANNEX 2m Guidelines On Home Monitoring and Clinical Protocol at Primary Care For Cat 1 and 2 Mild Confirmed COVID-19 Cases 02122021hoe hao keatNo ratings yet
- Gambaran Dan Lesi Rahang Pada Radiograf: Border Periosteal ReactionDocument6 pagesGambaran Dan Lesi Rahang Pada Radiograf: Border Periosteal ReactionI Dewa Ayu SavitriNo ratings yet
- Assessment - of - SKIN HAIR AND NAILS CHECKLISTDocument8 pagesAssessment - of - SKIN HAIR AND NAILS CHECKLISTJonah R. MeranoNo ratings yet
- Malaysian Orthopaedic JournalDocument21 pagesMalaysian Orthopaedic JournalnithinvenkatNo ratings yet
- Peritonea L DialysisDocument46 pagesPeritonea L DialysisRen SiavingcoNo ratings yet
- Early Complications in Prepectoral Tissue Expander Based Breast ReconstructionDocument11 pagesEarly Complications in Prepectoral Tissue Expander Based Breast ReconstructionBruno Mañon0% (1)
- Broward Teachers Union Lawsuit Against School DistrictDocument18 pagesBroward Teachers Union Lawsuit Against School DistrictMichelle SolomonNo ratings yet
- 4a's LESSON PLAN FOR GRADE 8 - HealthDocument2 pages4a's LESSON PLAN FOR GRADE 8 - HealthDremie Works100% (1)
- AdrenalineDocument13 pagesAdrenalineMobahil AhmadNo ratings yet
- 5 Medicinal PlantsDocument7 pages5 Medicinal PlantsJc ZelleNo ratings yet
- Hs Sexlinked InheritanceDocument14 pagesHs Sexlinked InheritanceMarcelo Pessoa NetoNo ratings yet
- Chronic PancreatitisDocument42 pagesChronic PancreatitismmurugeshrajNo ratings yet
- Hypertension - A Companion To Braunwald - S Heart Disease 3rd Edition (2017)Document503 pagesHypertension - A Companion To Braunwald - S Heart Disease 3rd Edition (2017)JOLANDA ANGELIN100% (1)
- HLTENN004 Assignment - NursingDocument4 pagesHLTENN004 Assignment - NursingJulianneTintNo ratings yet