You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- All Bleeding Stops - Stephen M CohnDocument199 pagesAll Bleeding Stops - Stephen M CohnmiladkohistaniofficialNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- New Trend IV FluidsDocument9 pagesNew Trend IV FluidsMarfu'ah Mar'ahNo ratings yet
- Ringer's Lactate - StatPearls - NCBI BookshelfDocument4 pagesRinger's Lactate - StatPearls - NCBI BookshelfMarfu'ah Mar'ahNo ratings yet
- Albumin (Human) 20%, USPPlasbumin®-20Document8 pagesAlbumin (Human) 20%, USPPlasbumin®-20Marfu'ah Mar'ahNo ratings yet
- Pharmacogenetics Drug Drug Interactions1Document16 pagesPharmacogenetics Drug Drug Interactions1Marfu'ah Mar'ahNo ratings yet
- Taking The Wrong Medication of Digoxin TabletsDocument3 pagesTaking The Wrong Medication of Digoxin TabletsMarfu'ah Mar'ahNo ratings yet
- Ddgi and Ddgdi RevDocument26 pagesDdgi and Ddgdi RevMarfu'ah Mar'ahNo ratings yet
- Pharmacogenomics DDI and DDGIDocument39 pagesPharmacogenomics DDI and DDGIMarfu'ah Mar'ahNo ratings yet
- Pharmaco GenomicsDocument14 pagesPharmaco GenomicsMarfu'ah Mar'ahNo ratings yet
- Tobacco and KretekDocument22 pagesTobacco and KretekMarfu'ah Mar'ahNo ratings yet
- Pain Management Us PharmacistDocument78 pagesPain Management Us PharmacistMarfu'ah Mar'ah100% (1)
- Complex DrugDrugGeneDisease Interactions Involving Cytochromes P450Document27 pagesComplex DrugDrugGeneDisease Interactions Involving Cytochromes P450Marfu'ah Mar'ahNo ratings yet
- Tieraona Low Dog, MD, With and Marc S. Micozzi, MD, PHD (Auth.) - Women's Health in Complementary and Integrative Medicine. A Clinical Guide (2005)Document353 pagesTieraona Low Dog, MD, With and Marc S. Micozzi, MD, PHD (Auth.) - Women's Health in Complementary and Integrative Medicine. A Clinical Guide (2005)Marfu'ah Mar'ahNo ratings yet
- Guidlane TB 2020Document42 pagesGuidlane TB 2020Marfu'ah Mar'ahNo ratings yet
- Choice Between Gastrostomy and JejunostomyDocument22 pagesChoice Between Gastrostomy and JejunostomyJonel BuenaventuraNo ratings yet
- Prepared By: Sarah A. Ligaya, PTRP Arisa Takagi, PTRP, PTDocument44 pagesPrepared By: Sarah A. Ligaya, PTRP Arisa Takagi, PTRP, PTShan EstanislaoNo ratings yet
- Raksha PDFDocument86 pagesRaksha PDFPrints BindingsNo ratings yet
- Clinical Rotation PlanDocument2 pagesClinical Rotation PlanManisha ThakurNo ratings yet
- Fever in IcuDocument17 pagesFever in Iculakshminivas PingaliNo ratings yet
- Prediction of Poor Outcomes For Septic Children According To FerritinDocument8 pagesPrediction of Poor Outcomes For Septic Children According To FerritinShofa 'fanni' NisrinaNo ratings yet
- Airway AdjunctsDocument17 pagesAirway AdjunctsChannelGNo ratings yet
- Physiotherapy For Cardio Respiratory Conditions: Q.P.CODE:1119-NSDocument22 pagesPhysiotherapy For Cardio Respiratory Conditions: Q.P.CODE:1119-NSSHAIK SHABEENANo ratings yet
- Pain Assessment in The Patient Unable To Self ReportDocument21 pagesPain Assessment in The Patient Unable To Self ReportNurul AenNo ratings yet
- The Variability of Critical Care Bed Numbers in Europe: OriginalDocument7 pagesThe Variability of Critical Care Bed Numbers in Europe: OriginalkotiniNo ratings yet
- ID Pengaruh Tindakan Penghisapan Lendir EndDocument8 pagesID Pengaruh Tindakan Penghisapan Lendir EndipurplaNo ratings yet
- Administration in Clinical ServicesDocument29 pagesAdministration in Clinical ServicesDr Ashish ManochaNo ratings yet
- The Third International Consensus Definition For Sepsis and Septic ShockDocument13 pagesThe Third International Consensus Definition For Sepsis and Septic ShockdrhendyjuniorNo ratings yet
- Annalsats 201404-164otDocument1 pageAnnalsats 201404-164otPhương UyênNo ratings yet
- The Textbook of Critical Care Including Trauma andDocument2 pagesThe Textbook of Critical Care Including Trauma andRahul KirkNo ratings yet
- Role Development Module 6 Assignment APRN Interview and Analysis Written by Carly BerlonDocument3 pagesRole Development Module 6 Assignment APRN Interview and Analysis Written by Carly Berlonapi-451008354No ratings yet
- Project Proposal: Code of 1991 Mandates The Local Government Units To Provide Basic FacilitiesDocument4 pagesProject Proposal: Code of 1991 Mandates The Local Government Units To Provide Basic Facilitiescasagantm-1No ratings yet
- Nightingale Institute of Nursing: AssignmentDocument18 pagesNightingale Institute of Nursing: AssignmentDhAiRyA ArOrANo ratings yet
- Admission Discharge Criteria To A Critical Care UnitDocument6 pagesAdmission Discharge Criteria To A Critical Care UnitsafaaNo ratings yet
- Business Plan of HospitalDocument34 pagesBusiness Plan of HospitalArslan100% (26)
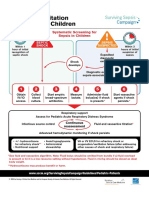
- Initial Resuscitation Algorithm For Children - Pdf.aspxDocument2 pagesInitial Resuscitation Algorithm For Children - Pdf.aspxasniatkoNo ratings yet
- TMC Practice TestDocument17 pagesTMC Practice TestRisen ManlosaNo ratings yet
- The Research Proposal TemplateDocument17 pagesThe Research Proposal TemplatePractice Medi-nursingNo ratings yet
- Evaluation and Management Billing and CodingDocument7 pagesEvaluation and Management Billing and Codingchurchil owinoNo ratings yet
- Deniz 2022Document10 pagesDeniz 2022syakurNo ratings yet
- Health TeamDocument5 pagesHealth TeamFahim AhmedNo ratings yet
- PFCCS Instructor Director Consultant CriteriaDocument3 pagesPFCCS Instructor Director Consultant CriteriaImam RahmadiNo ratings yet
- ABG Practice QuizDocument4 pagesABG Practice QuizRiz Austria RN0% (1)
- General & Multi Speciality HospitalsDocument17 pagesGeneral & Multi Speciality HospitalsHarsha INo ratings yet