You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- UntitledDocument663 pagesUntitledAna Beatriz MedeirosNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Solution Manual For Abnormal Psychology 18th Edition Jill M Hooley Matthew Nock James ButcherDocument25 pagesSolution Manual For Abnormal Psychology 18th Edition Jill M Hooley Matthew Nock James ButcherRichardGranttbaie100% (81)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Medical Symptoms A Visual Guide 2nd Edition The Easy Way To Identify Medical Problems DORLING KINDERSLEY LTDDocument258 pagesMedical Symptoms A Visual Guide 2nd Edition The Easy Way To Identify Medical Problems DORLING KINDERSLEY LTDShekinah WilcoxNo ratings yet
- Neurology Important McqsDocument12 pagesNeurology Important McqsFarhan Khosa100% (1)
- Minutes of Management Review Meeting OkDocument3 pagesMinutes of Management Review Meeting Okdidar100% (4)
- Healthcare Virtual AssistantsDocument14 pagesHealthcare Virtual AssistantsJessica TayagNo ratings yet
- Notice of Management Review MeetingDocument1 pageNotice of Management Review MeetingdidarNo ratings yet
- WIP Production Report 2009Document6 pagesWIP Production Report 2009didarNo ratings yet
- Costing Prazover 20 MGDocument1 pageCosting Prazover 20 MGdidarNo ratings yet
- Soil Digger Rent PriceDocument2 pagesSoil Digger Rent PricedidarNo ratings yet
- Meeting Minutes 05.02.2022Document4 pagesMeeting Minutes 05.02.2022didarNo ratings yet
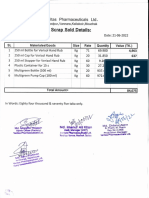
- Scrub & Broken Trees SoldDocument5 pagesScrub & Broken Trees SolddidarNo ratings yet
- Stability Chamber - QuotationDocument4 pagesStability Chamber - QuotationdidarNo ratings yet
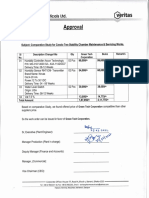
- Change Approval FormDocument2 pagesChange Approval FormdidarNo ratings yet
- Scan2022 07 20 - 163719Document1 pageScan2022 07 20 - 163719didarNo ratings yet
- HomeopathicDocument3 pagesHomeopathicdidarNo ratings yet
- Appraisal (2022 - 02 - 10 02 - 59 - 27 UTC)Document2 pagesAppraisal (2022 - 02 - 10 02 - 59 - 27 UTC)didarNo ratings yet
- Scan2022 08 03 - 132224Document1 pageScan2022 08 03 - 132224didarNo ratings yet
- Daily MeetingDocument1 pageDaily MeetingdidarNo ratings yet
- NoticeDocument1 pageNoticedidarNo ratings yet
- Motor Cycle Price Offer 21.07.2022Document2 pagesMotor Cycle Price Offer 21.07.2022didarNo ratings yet
- " (Veritas Pharmaceuticals: PlantDocument1 page" (Veritas Pharmaceuticals: PlantdidarNo ratings yet
- Motor Cycle HandoverDocument1 pageMotor Cycle HandoverdidarNo ratings yet
- Veritas Pharmaceuticals LTDDocument4 pagesVeritas Pharmaceuticals LTDdidarNo ratings yet
- Damage Air Compressor - Sales Price OfferDocument3 pagesDamage Air Compressor - Sales Price OfferdidarNo ratings yet
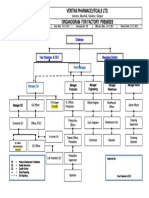
- Veritas Pharmaceuticals Ltd. Organogram For Factory PremisesDocument1 pageVeritas Pharmaceuticals Ltd. Organogram For Factory PremisesdidarNo ratings yet
- Ffifixas: Veritas PharmaceuticalsDocument1 pageFfifixas: Veritas PharmaceuticalsdidarNo ratings yet
- Tadalafil INN 10 MG TabletDocument7 pagesTadalafil INN 10 MG TabletdidarNo ratings yet
- Veritas Pharmaceuticals LTD: TO: Management Associates CC To: Honorable Chairman & Honorable VC &CEODocument19 pagesVeritas Pharmaceuticals LTD: TO: Management Associates CC To: Honorable Chairman & Honorable VC &CEOdidarNo ratings yet
- Existing Machinery StatusDocument3 pagesExisting Machinery StatusdidarNo ratings yet
- RM PM Stock VerisolDocument1 pageRM PM Stock VerisoldidarNo ratings yet
- Vitamin C 250 MG TabletDocument5 pagesVitamin C 250 MG TabletdidarNo ratings yet
- MD Muminur Rahman 2021-1-91-041Document22 pagesMD Muminur Rahman 2021-1-91-041Md MuminurNo ratings yet
- N078 DMaterialsDocument84 pagesN078 DMaterialsFeriel FerielNo ratings yet
- Sample Id: Sample Id: 34046605 Icmr Specimen Referral Form Icmr Specimen Referral Form For For Covid-19 (Sars-Cov2) Covid-19 (Sars-Cov2)Document2 pagesSample Id: Sample Id: 34046605 Icmr Specimen Referral Form Icmr Specimen Referral Form For For Covid-19 (Sars-Cov2) Covid-19 (Sars-Cov2)S4 HanaNo ratings yet
- Corona Virus SpeechDocument1 pageCorona Virus SpeechJean Gabriela CaparrosNo ratings yet
- FIRST RESPONDER Care Summary MatrixDocument3 pagesFIRST RESPONDER Care Summary MatrixAleksandar PetrovicNo ratings yet
- ESI ER CompleteDocument45 pagesESI ER Completetammy2121No ratings yet
- Evolve Resources For Goulds Pathophysiology For The Health Professions 6th Edition Hubert Test BankDocument8 pagesEvolve Resources For Goulds Pathophysiology For The Health Professions 6th Edition Hubert Test Bankjosephgillmtjirpxngk100% (15)
- Ie Format OlfuDocument8 pagesIe Format OlfuJonathan ZapantaNo ratings yet
- Points To Note For Persons Tested Preliminarily Positive / Positive Pending Admission To Hospitals or Isolation Facilities LeafletDocument2 pagesPoints To Note For Persons Tested Preliminarily Positive / Positive Pending Admission To Hospitals or Isolation Facilities LeafletHKFPNo ratings yet
- Mythos World - PlaybooksDocument30 pagesMythos World - PlaybooksPlural FutureNo ratings yet
- Health Certificate: Personal Details: Section ADocument3 pagesHealth Certificate: Personal Details: Section APrashob SugathanNo ratings yet
- What Is Covid19Document7 pagesWhat Is Covid19Prity KumariNo ratings yet
- Cefadroxil Mylan Capsule Hard, Film-Coated Tablet, Oral Suspension ENG PL - 09001be680190988Document5 pagesCefadroxil Mylan Capsule Hard, Film-Coated Tablet, Oral Suspension ENG PL - 09001be680190988Ajeng VinaNo ratings yet
- Case Study Analysis - The Case of MeredithDocument4 pagesCase Study Analysis - The Case of MeredithMichelle GaleosNo ratings yet
- Q1 M1 Gr.7Document39 pagesQ1 M1 Gr.7Rowena PaguiaNo ratings yet
- 01章(1 29)物理治疗转诊筛查Document29 pages01章(1 29)物理治疗转诊筛查zhangpengNo ratings yet
- Educ 7 ReviewerDocument37 pagesEduc 7 ReviewerRalph Raymond CervantesNo ratings yet
- Assessment Report Mentha X Piperita L Folium Aetheroleum Revision 1 - enDocument101 pagesAssessment Report Mentha X Piperita L Folium Aetheroleum Revision 1 - enANAHI AUQUI AROTOMANo ratings yet
- Health FinalDocument11 pagesHealth Finalbernadeth magtibayNo ratings yet
- LKPD News ItemDocument9 pagesLKPD News Itemsugi antiNo ratings yet
- MeggyDocument7 pagesMeggyAubrey Meg Y. GajeteNo ratings yet
- APA Guidelines For Treating Adults With SchizophreniaDocument8 pagesAPA Guidelines For Treating Adults With SchizophreniaKaren C. ManoodNo ratings yet
- Unit 9 Taking About Symtoms + Unit 13 Family MedicineDocument2 pagesUnit 9 Taking About Symtoms + Unit 13 Family MedicineThuy AnhNo ratings yet
- Juvenile Osteochondrosis of The Cuneiform BonesDocument4 pagesJuvenile Osteochondrosis of The Cuneiform BonesasclepiuspdfsNo ratings yet
- 2023 - ACRM - Diagnositc - CriteriaDocument13 pages2023 - ACRM - Diagnositc - CriteriaRobinNo ratings yet