You might also like
- Mckinsey Healthcare AnalyticsDocument36 pagesMckinsey Healthcare AnalyticsAndrey PritulyukNo ratings yet
- Forensic Approaches To Death Disaster and AbuseDocument332 pagesForensic Approaches To Death Disaster and Abusetupac446100% (4)
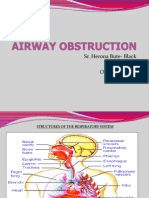
- Airway ObstructionDocument35 pagesAirway ObstructionJemicia AdamsNo ratings yet
- Accident Investigation 1Document63 pagesAccident Investigation 1Biscuit_WarriorNo ratings yet
- Egan's Skilled Helper Model - Developments and Applications in Counselling (PDFDrive)Document217 pagesEgan's Skilled Helper Model - Developments and Applications in Counselling (PDFDrive)Erfana Thasnem100% (2)
- Enclosed/ Confined Space Entry Permit: As Per ISGOTT - Chapter 10Document4 pagesEnclosed/ Confined Space Entry Permit: As Per ISGOTT - Chapter 10irakli100% (2)
- Module 1.the Domain of Production and Operations Management (Operations Management) - Opem 311Document8 pagesModule 1.the Domain of Production and Operations Management (Operations Management) - Opem 311Maritoni MedallaNo ratings yet
- Transfer of The Critically Ill Adult PatientDocument5 pagesTransfer of The Critically Ill Adult PatientJoao Pedro QuevedoNo ratings yet
- Big Picture: AddictionDocument16 pagesBig Picture: AddictionWellcome Trust100% (1)
- Bsbcmm401 Task 1 & 2 (Tal)Document16 pagesBsbcmm401 Task 1 & 2 (Tal)Shar KhanNo ratings yet
- Transportation of Patients - Ambulances - Maintaining Patient SafetyDocument4 pagesTransportation of Patients - Ambulances - Maintaining Patient SafetyNicolo Martin BelloNo ratings yet
- Jal NetiDocument3 pagesJal Netisun1986No ratings yet
- Immunology Syllabus-2015 PDFDocument307 pagesImmunology Syllabus-2015 PDFLorena BravoNo ratings yet
- Hospital Support Service - IIDocument17 pagesHospital Support Service - IIbharadwajNo ratings yet
- A High Proportion of Prehospital Emergency Patients Are Not Transported by Ambulance 2017Document9 pagesA High Proportion of Prehospital Emergency Patients Are Not Transported by Ambulance 2017Angel ArreolaNo ratings yet
- Nelson Essentials of Pediatrics 7th Edition 2015Document4 pagesNelson Essentials of Pediatrics 7th Edition 2015Rida Zaheer Tariq SheikhNo ratings yet
- Clinical Assessment and Treatment in Paediatric Wards in The North-East of The United Republic of TanzaniaDocument8 pagesClinical Assessment and Treatment in Paediatric Wards in The North-East of The United Republic of TanzaniaOheneba Kwadjo Afari DebraNo ratings yet
- Implementation of The Modified Canadian C Spine Rule by ParamedicsDocument10 pagesImplementation of The Modified Canadian C Spine Rule by Paramedicscarper454No ratings yet
- Transport and Communication Systems in Health Services: Tropical Doctor August 1977Document5 pagesTransport and Communication Systems in Health Services: Tropical Doctor August 1977mohit7898No ratings yet
- 10217-Article Text-56357-1-10-20211220Document6 pages10217-Article Text-56357-1-10-20211220Joy B. DaladagNo ratings yet
- Emergency TrolleysDocument5 pagesEmergency Trolleysabrahem igbariaNo ratings yet
- Articles: BackgroundDocument9 pagesArticles: BackgroundBassim BirklandNo ratings yet
- Kings Well 2017Document8 pagesKings Well 2017Migumi YoshugaraNo ratings yet
- Who Oms 16-175885 PDFDocument8 pagesWho Oms 16-175885 PDFsofiabloemNo ratings yet
- Telehealth-Enabled Emergency Medical Services Program Reduces Ambulance Transport To Urban Emergency DepartmentsDocument20 pagesTelehealth-Enabled Emergency Medical Services Program Reduces Ambulance Transport To Urban Emergency DepartmentsYohanaNo ratings yet
- Equipment For Ground AmbulancesDocument7 pagesEquipment For Ground AmbulancesNteziryayo EzechielNo ratings yet
- The Maternal Health Compact: Rural Health C AreDocument2 pagesThe Maternal Health Compact: Rural Health C AreanggiNo ratings yet
- 4 5-Appendicectomy PDFDocument12 pages4 5-Appendicectomy PDFtamiNo ratings yet
- Comparative Analysis of Using 112 Emergency Ambulance Services in Turkey and The Province of KonyaDocument7 pagesComparative Analysis of Using 112 Emergency Ambulance Services in Turkey and The Province of KonyaPutra MentaokNo ratings yet
- Pembe 2010Document9 pagesPembe 2010Berry BancinNo ratings yet
- Civilian Aeromedical Retrievals (The Australian Experience)Document5 pagesCivilian Aeromedical Retrievals (The Australian Experience)ramzi MohamedNo ratings yet
- Intl J Gynecology Obste - 2021 - Burke - A Ketamine Package For Use in Emergency Cesarean Delivery When No Anesthetist IsDocument8 pagesIntl J Gynecology Obste - 2021 - Burke - A Ketamine Package For Use in Emergency Cesarean Delivery When No Anesthetist IsHerman FiraNo ratings yet
- Close, But Still Too Far. The Experience of Australian People With Cancer Commuting From A Regional To A Capital City For Radiotherapy TreatmentDocument8 pagesClose, But Still Too Far. The Experience of Australian People With Cancer Commuting From A Regional To A Capital City For Radiotherapy TreatmentyouldenaNo ratings yet
- A Statewide Analysis of EMS' Pediatric Transport Destination DecisionsDocument25 pagesA Statewide Analysis of EMS' Pediatric Transport Destination Decisionssouhail gnaneNo ratings yet
- Kozhimannil (2016) AJOGDocument10 pagesKozhimannil (2016) AJOGNatalia DalenceNo ratings yet
- Bmjopen 2014 005828Document9 pagesBmjopen 2014 005828antidius johnNo ratings yet
- Review of Acute Cancer Beds 1Document2 pagesReview of Acute Cancer Beds 1Cepi Ridwan FerdiansyahNo ratings yet
- Burden of Emergency Medical Services Usage by Dialysis PatientsDocument8 pagesBurden of Emergency Medical Services Usage by Dialysis PatientsBarry TraceyNo ratings yet
- Caesarean in Rural Environment of Eastern Kasai (R.D. Congo) Cover of The Needs and Quality of The Services With Kasansa and TshilengeDocument8 pagesCaesarean in Rural Environment of Eastern Kasai (R.D. Congo) Cover of The Needs and Quality of The Services With Kasansa and TshilengeAnonymous SMEU6r2No ratings yet
- Chest X-Ray As An Essential Part of Routine Medical Examination: Is It Necessary?Document4 pagesChest X-Ray As An Essential Part of Routine Medical Examination: Is It Necessary?rajpot potNo ratings yet
- The Global Burden of Women's Cancers - A Grand Challenge in Global HealthDocument14 pagesThe Global Burden of Women's Cancers - A Grand Challenge in Global HealthroyNo ratings yet
- Sahloul Et Al 2016 Cancer Care at Times of Crisis and War The Syrian ExampleDocument8 pagesSahloul Et Al 2016 Cancer Care at Times of Crisis and War The Syrian ExampleAntony HenningsNo ratings yet
- Critical Care: Queuing Theory Accurately Models The Need For Critical Care ResourcesDocument6 pagesCritical Care: Queuing Theory Accurately Models The Need For Critical Care ResourcesAngela SaoNo ratings yet
- Newborn Aides: An Innovative Approach in Sick Newborn Care at A District-Level Special Care UnitDocument7 pagesNewborn Aides: An Innovative Approach in Sick Newborn Care at A District-Level Special Care Unitmuhar randiNo ratings yet
- Obstetric Referrals at Saint Paul'S Hospital Millennium Medical College (SPHMMC) : Pre-Referral Care and AppropriatenessDocument7 pagesObstetric Referrals at Saint Paul'S Hospital Millennium Medical College (SPHMMC) : Pre-Referral Care and AppropriatenessTaklu Marama M. BaatiiNo ratings yet
- PakurDocument17 pagesPakurAnik SinghNo ratings yet
- Use of Health Services by Prison Inmates ComparisoDocument3 pagesUse of Health Services by Prison Inmates ComparisoJOSE LUCERONo ratings yet
- Jurnal Inter 1Document10 pagesJurnal Inter 1Adhe YuniarNo ratings yet
- Transforming Community Services 2011: Challenges and WinnersDocument11 pagesTransforming Community Services 2011: Challenges and WinnersDepartmentofHealthNo ratings yet
- Paediatric Index of Mortality 3Document9 pagesPaediatric Index of Mortality 3Hendra MahardikaNo ratings yet
- Guidelines For The Management of Pediatric Head Injury in AlaskaDocument19 pagesGuidelines For The Management of Pediatric Head Injury in AlaskaKenNo ratings yet
- Epidemiology of Critically Ill Patients in Intensive Care Units: A Population-Based Observational StudyDocument8 pagesEpidemiology of Critically Ill Patients in Intensive Care Units: A Population-Based Observational StudyMohamat MutajirNo ratings yet
- Mobile Health Clinics in The Era of Reform: © Managed Care & Healthcare Communications, LLCDocument4 pagesMobile Health Clinics in The Era of Reform: © Managed Care & Healthcare Communications, LLCdrestadyumna ChilspiderNo ratings yet
- Emergency Medical Services inDocument5 pagesEmergency Medical Services inWawan JokoNo ratings yet
- Guideline. Rectal Cancer Version 2-2018.NCCN Clinical PracticeDocument29 pagesGuideline. Rectal Cancer Version 2-2018.NCCN Clinical PracticeTrí Cương NguyễnNo ratings yet
- 1 SMDocument5 pages1 SMali syahbanaNo ratings yet
- NIH Public Access: The Human and Economic Burden of Cervical Cancer in TexasDocument12 pagesNIH Public Access: The Human and Economic Burden of Cervical Cancer in TexassihqinarsrNo ratings yet
- Journal Pone 0265262Document12 pagesJournal Pone 0265262golden abidemNo ratings yet
- Analisis Situasi IGDDocument6 pagesAnalisis Situasi IGDNur HolizaNo ratings yet
- Journal Emergency Patient Transportation in South Asiacall For A Proper Prehospital Care SystemDocument3 pagesJournal Emergency Patient Transportation in South Asiacall For A Proper Prehospital Care SystemMohammad SutamiNo ratings yet
- Antiedema Effects of Hypertonic Saline After SCI - Editorial (2009) PDFDocument19 pagesAntiedema Effects of Hypertonic Saline After SCI - Editorial (2009) PDFCoal CoalyNo ratings yet
- Mackenzie 2013Document10 pagesMackenzie 2013scribd.glowing960No ratings yet
- Farmers and Chest Pain ArticleDocument9 pagesFarmers and Chest Pain ArticleAlexander DarlingNo ratings yet
- An Intervention Involving Traditional Birth Attendants and Perinatal and Maternal Mortality in PakistanDocument9 pagesAn Intervention Involving Traditional Birth Attendants and Perinatal and Maternal Mortality in PakistanAndaru Kusuma PrajaNo ratings yet
- 1540 1413 Article p181Document29 pages1540 1413 Article p181NeliNo ratings yet
- Content ServerDocument13 pagesContent ServerIngca ClaudiaNo ratings yet
- Research ArticleDocument12 pagesResearch ArticleFhasya Aditya PutraNo ratings yet
- Broderick 2015Document4 pagesBroderick 2015Jimmy SilverhandNo ratings yet
- State of TelehealthDocument8 pagesState of TelehealthLiz HackettNo ratings yet
- 989 FullDocument6 pages989 FullIndermeet Singh AnandNo ratings yet
- Atypical Breast Proliferative Lesions and Benign Breast DiseaseFrom EverandAtypical Breast Proliferative Lesions and Benign Breast DiseaseFarin AmersiNo ratings yet
- Ananthanarayan and Paniker's Textbook of Microbiology TestDocument672 pagesAnanthanarayan and Paniker's Textbook of Microbiology TestRexArtem100% (1)
- Pediatric Pharyngotonsillitis Sore ThroatDocument5 pagesPediatric Pharyngotonsillitis Sore Throatdef_10No ratings yet
- Transcultural Nursing Nur324Document18 pagesTranscultural Nursing Nur324lidyaNo ratings yet
- Role of QEEG in Spiritual Science ResearchDocument10 pagesRole of QEEG in Spiritual Science ResearchMeha FatimaNo ratings yet
- Book ReviewDocument10 pagesBook ReviewCezanne CruzNo ratings yet
- AlzheimerDocument7 pagesAlzheimerInas100% (1)
- Assembly & User Manual: Artemis Ii Air RowerDocument28 pagesAssembly & User Manual: Artemis Ii Air Roweragn003No ratings yet
- 6 Laboratory SafetyDocument17 pages6 Laboratory SafetyNipun ShamikaNo ratings yet
- Describe An Unforgettable Interview You Have HadDocument4 pagesDescribe An Unforgettable Interview You Have HadTruc LeNo ratings yet
- Research Group Member RatingDocument1 pageResearch Group Member RatingMrJay OisotrasNo ratings yet
- Complaint Walgreen Murphy 03 8 11Document22 pagesComplaint Walgreen Murphy 03 8 11s_klineNo ratings yet
- Dairy Best Ad - Focus Group DiscussionDocument5 pagesDairy Best Ad - Focus Group DiscussionUpasana SilNo ratings yet
- REVISED HVAC Layout For DC3 Annex - 4F Roof - 08.10.2022.dwg-Roof HVACDocument1 pageREVISED HVAC Layout For DC3 Annex - 4F Roof - 08.10.2022.dwg-Roof HVACaamnagroup officeNo ratings yet
- Minimum Required Skills of Physical Therapist GraduatesDocument16 pagesMinimum Required Skills of Physical Therapist GraduatesIndra IndfisNo ratings yet
- CO57963Document18 pagesCO57963Patrick PiscitelloNo ratings yet
- Herbal Cigarette: Group No 9Document11 pagesHerbal Cigarette: Group No 9Riddhi GuptaNo ratings yet
- Sika Top-Seal 107Document5 pagesSika Top-Seal 107Gibbs PerNo ratings yet
- Intermittent FastingDocument7 pagesIntermittent FastingJohnny KeeverNo ratings yet
- PICC ProcedureDocument35 pagesPICC ProcedureTemiloluwa AdeyemiNo ratings yet