You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Drill String Design 4.11Document23 pagesDrill String Design 4.11Ryan Tan Ping Yi100% (1)
- CL 604-Power Plant PDFDocument38 pagesCL 604-Power Plant PDFBhaskerNegiNo ratings yet
- Advances in Parasit OlogyDocument321 pagesAdvances in Parasit Ologyintanhardianti7No ratings yet
- NCD Proof PDFDocument2 pagesNCD Proof PDFAnonymous TDzUwCg67% (3)
- Eddy Current Testing in NDTDocument43 pagesEddy Current Testing in NDTMeby Selvaraj RNo ratings yet
- 24 Basic Tai Chi Chuan (Yang Style) : Relaxation and HarmonyDocument2 pages24 Basic Tai Chi Chuan (Yang Style) : Relaxation and HarmonyDharma LingamNo ratings yet
- AstmDocument5 pagesAstmandresNo ratings yet
- PX 95 Service ManualDocument167 pagesPX 95 Service Manualidigiti100% (1)
- CIVREV!!!!Document5 pagesCIVREV!!!!aypod100% (1)
- RA 9231 (Special Protection For Children)Document5 pagesRA 9231 (Special Protection For Children)Lutchel Albis TanjayNo ratings yet
- Apex Beat..how To LocateDocument20 pagesApex Beat..how To LocateMaha MukhtarNo ratings yet
- Carvera Manual EngDocument30 pagesCarvera Manual EngBilly DipperNo ratings yet
- HematologyDocument100 pagesHematologyerzaraptorNo ratings yet
- Jurnal Terapi Komprehensif HipertensiDocument4 pagesJurnal Terapi Komprehensif HipertensiismiNo ratings yet
- CDEP-Structural ReviewerDocument42 pagesCDEP-Structural ReviewerSalted EggNo ratings yet
- MaterialsofMachines 10011526 PDFDocument224 pagesMaterialsofMachines 10011526 PDFmaese_obsesivoNo ratings yet
- Schuetziana 5 2014 1Document41 pagesSchuetziana 5 2014 1Vladimir RadenkovicNo ratings yet
- Taxi ReceiptDocument17 pagesTaxi ReceiptPraveen KumarNo ratings yet
- Xyr 5000 Wt530Document9 pagesXyr 5000 Wt530murali52100% (1)
- Ben and Jerry Situation Analysis 1Document30 pagesBen and Jerry Situation Analysis 1api-238369021100% (1)
- DDC SVC Bro 0002Document35 pagesDDC SVC Bro 0002SonthiMNo ratings yet
- Sogang KLEC - Confirmation For Self-Quarantine Location - ENGDocument1 pageSogang KLEC - Confirmation For Self-Quarantine Location - ENGAlive StillNo ratings yet
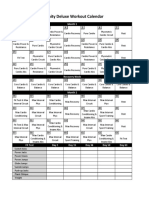
- Insanity Workout Deluxe Calendar SimpleDocument1 pageInsanity Workout Deluxe Calendar SimpleCristian Manuel GonzálezNo ratings yet
- V. Kulish Human Respiration Anatomy and Physiology - Mathematical Modeling - Numerical Simulation and Applications Advances in Bioengineering 2006Document243 pagesV. Kulish Human Respiration Anatomy and Physiology - Mathematical Modeling - Numerical Simulation and Applications Advances in Bioengineering 2006Sofiah QotrunadaNo ratings yet
- Zimwnt-Ufc01 - WNTP236 - 4097 - 001 (00000002) PDFDocument71 pagesZimwnt-Ufc01 - WNTP236 - 4097 - 001 (00000002) PDFNatasa RalicNo ratings yet
- United States Court of Appeals, Tenth CircuitDocument6 pagesUnited States Court of Appeals, Tenth CircuitScribd Government DocsNo ratings yet
- Repair manualTRAKKER ATH-ADH.0003Document1 pageRepair manualTRAKKER ATH-ADH.0003MihajloNo ratings yet
- Service: ManualDocument103 pagesService: ManualSaulvcr64 PorleyNo ratings yet
- The Nervous System Answer KeyDocument1 pageThe Nervous System Answer KeymichelleNo ratings yet
- Caalogo Allen BradleyDocument27 pagesCaalogo Allen BradleyricardoqqNo ratings yet