Professional Documents
Culture Documents
2018 Cluster Headache
2018 Cluster Headache
Uploaded by
Tony NgCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
2018 Cluster Headache
2018 Cluster Headache
Uploaded by
Tony NgCopyright:
Available Formats
PRIMER
Cluster headache
Arne May1, Todd J. Schwedt2, Delphine Magis3, Patricia Pozo-Rosich4,5, Stefan Evers6
and Shuu-Jiun Wang7
Abstract | Cluster headache is an excruciating, strictly one-sided pain syndrome with attacks that
last between 15 minutes and 180 minutes and that are accompanied by marked ipsilateral cranial
autonomic symptoms, such as lacrimation and conjunctival injection. The pain is so severe that
female patients describe each attack as worse than childbirth. The past decade has seen
remarkable progress in the understanding of the pathophysiological background of cluster
headache and has implicated the brain, particularly the hypothalamus, as the generator of both
the pain and the autonomic symptoms. Anatomical connections between the hypothalamus
and the trigeminovascular system, as well as the parasympathetic nervous system, have also been
implicated in cluster headache pathophysiology. The diagnosis of cluster headache involves
excluding other primary headaches and secondary headaches and is based primarily on the
patient’s symptoms. Remarkable progress has been achieved in developing effective treatment
options for single cluster attacks and in developing preventive measures, which include
pharmacological therapies and neuromodulation.
Headache is one of the most common pain symptoms in two cluster periods (also known as cluster bouts), each
humans. It is extremely rare to have never had a head‑ lasting from 7 days to 1 year 1. These cluster periods are
ache, even when experiencing influenza infection or a separated by pain-free periods (also known as out-of-
mild head trauma. Headache is a normal physiological bout periods or remission periods) that last ≥3 months.
reaction; however, when headaches occur regularly and Diagnosis of chronic cluster headache requires cluster
without adequate triggers, they are regarded not as a attacks that occur for >1 year without remission p eriods
symptom but as a disease, examples of which include or with remission periods of <3 months in duration.
migraine and cluster headache. The International Cluster headache attacks usually also occur with clock‑
Classification of Headache Disorders (ICHD‑3), which like r egularity during the day and are common during
was updated in 2018, uses explicit diagnostic criteria the night.
based on symptoms and medical history for all head‑ The pathophysiology of cluster headache is not fully
ache disorders1. No single examination is able to define, understood but includes alterations in both the central
ensure or differentiate idiopathic headache syndromes2. and peripheral nervous systems, including activation
The ICHD‑3 summarizes one group of headache syn‑ of the trigeminovascular system (that is, divisions of
dromes as the trigeminal-autonomic cephalalgias (TACs; the trigeminal nerve that innervate the cranial blood
BOX 1)1, of which cluster headache is the most prominent vessels) and the parasympathetic nervous system, which
and common subtype. are speculated to underlie the pain and autonomic
Cluster headache is probably the most severe pain features of cluster headache, respectively. In addition,
known and is characterized by ipsilateral headache, with the hypothalamus — which interacts with several com‑
pain localized to the orbit, supraorbital and/or temporal ponents of the trigeminovascular system — is believed
regions and associated autonomic features. Autonomic to have an important role in the pathophysiology of
Correspondence to A.M.
Department of Systems
symptoms, such as lacrimation (tearing), conjunctival cluster headache.
Neuroscience, University injection (redness of the sclera), rhinorrhoea, nasal This Primer focuses on the current evidence of
Medical Center Hamburg- congestion, hyperhidrosis (excessive sweating) and eye‑ pathophysiology and diagnosis of cluster headache and
Eppendorf, Martinistrasse lid oedema, usually occur on the ipsilateral side to the how to manage patients, including those who are diffi‑
52, D-20246 Hamburg,
pain3 and are absent in only 3% of cases. Cluster head‑ cult to treat. This Primer also gives an up-to-date over‑
Germany.
a.may@uke.de ache can be subclassified as either episodic or chronic, view of the clinical features of cluster headache and a
of which the episodic form is more common and affects topical summary of the current state of research for this
Article number: 18006
doi:10.1038/nrdp.2018.6 80–90% of patients3. Based on the ICHD‑3 criteria, debilitating disease that is, in principle, easily treatable
Published online 1 Mar 2018 diagnosis of episodic cluster headache requires at least if certain principles are followed.
NATURE REVIEWS | DISEASE PRIMERS VOLUME 4 | ARTICLE NUMBER 18006 | 1
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
PRIMER
Author addresses Cluster bout periods seem to be more frequent in
spring and autumn; although there are some reports in this
1
Department of Systems Neuroscience, University Medical Center Hamburg-Eppendorf, regard, data are not available from all countries. However,
Martinistrasse 52, D-20246 Hamburg, Germany. one study in Taiwan stated that the cluster periods were
2
Department of Neurology, Mayo Clinic, Phoenix, AZ, USA. more likely to occur in autumn and winter and are
3
University Department of Neurology CHR, CHU de Liege, Belgium.
determined by the temperature of the preceding periods16.
4
Headache and Craniofacial Pain Unit, Neurology Department, Hospital Universitari Vall
d’Hebron, Barcelona, Spain. In regard to life habits and possible risk factors, cigar
5
Headache Research Group, VHIR, Universitat Autònoma Barcelona, Barcelona, Spain. ette smoking, head trauma and family history of head‑
6
Department of Neurology, Krankenhaus Lindenbrunn, Coppenbrügge, Germany. ache were associated with cluster headache in an Italian
7
Taipei Veterans General Hospital, National Yang-Ming University School of Medicine, epidemiological case–control study 17.
Taipei, Taiwan.
Genetic factors
Epidemiology Previous twin and family studies have highlighted the
Sociodemographic factors importance of genetic factors in cluster headache4,18.
Cluster headache is a rare headache disorder that occurs Individuals with first-degree and second-degree relatives
globally in 0.1% of the general population but accounts for with cluster headache have an increased risk compared
<3% of all patients with headache in Asia4–6. Cluster head‑ with the general population19,20. Some studies suggest
ache has a male preponderance; the Cluster Headache that cluster headache is an autosomal recessive inherited
Survey completed by 1,134 individuals in the United States disorder, although others have suggested an autosomal
confirmed earlier reports that ~72% of patients are male7. dominant or multifactorial inheritance pattern21.
A decreasing male to female ratio has been reported in the Genetic association studies focusing on the identifi
past 30 years8. This difference is probably attributable to cation of candidate genes for cluster headache have
better epidemiological tools, improved adherence to the suggested a modulatory role for HCRTR2 (encoding
diagnostic criteria and increased knowledge of the dis‑ hypocretin (orexin) receptor type 2) in posterior hypo‑
ease9; a lack of awareness of the disorder probably led to thalamic neurons that are involved in the trigeminal pain
frequent misdiagnosis as migraine10. Indeed, a large pro‑ pathway 22–24; however, this hypothesis was contradicted
portion of patients with cluster headache have migraine- in a recent meta-analysis25. Other studies have associated
like f eatures, such as photophobia (sensitivity to light) homozygosity for the 1246G>A allele of HCRTR2 with
or osmophobia (hypersensitivity to odours), in addition an increased risk of cluster headache26,27, but this finding
to the typical trigeminal-autonomic symptoms, such as was not confirmed in a large multinational study22. Given
ptosis (drooping of the upper eyelid), sweating and miosis the association between polymorphisms in HCRTR2 and
(constriction of the pupils). These patients (up to 46% in cluster headache as well as the role of the orexin system in
a large Italian study) also show a relatively younger age of the pathophysiology (see Mechanisms/pathophysiology,
onset and attacks that are longer in duration than cluster below), sleep disorders such as narcolepsy have been
headache attacks without migraineous features11. suggested to be associated with cluster headache28. Other
The age at onset of cluster headache ranged from genetic association studies have revealed negative or con‑
10 years to 68 years of age in one study in Sweden, with flicting results for the association of several genetic alter‑
a peak between 20 years and 29 years of age for both ations with cluster headache, including mitochondrial
sexes12. In the United States, cluster headache onset has DNA mutation29, genes encoding nitric oxide synthase
been shown to occur before 20 years of age in 35% of (NOS1, NOS2A and NOS3)30, CACNA1A (encoding
patients and between 21 years and 30 years of age in 36%
of patients7. Onset is less likely to occur between 31 years
and 40 years of age (observed in 16% of patients) and Box 1 | Trigeminal-autonomic cephalalgias
between 41 years and 50 years of age (observed in 10% The trigeminal-autonomic cephalalgias (TACs) are a
of patients)7. Only 3% of patients were >51 years of age group of headache disorders characterized by unilateral
at onset in the United States7. Other studies conducted in headaches with autonomic symptoms ipsilateral to the
the United States and Italy have shown an onset of cluster pain, such as miosis (constriction of the pupil), ptosis
headache before 50 years of age in 83.3% of women and (drooping of the upper eyelid), lacrimation (tearing) and
91.3% of men13,14. In a large Italian study, the mean age conjunctival injection (redness of the sclera). Individual
TACs have distinct patterns of duration, frequency,
at onset was 30.2 years. In this study, women with pri‑
periodicity and intensity of attacks. In the most current
mary chronic cluster headache (cluster headache that was International Classification of Headache Disorders
chronic from onset) had a mean age at onset of 42.8 years; (ICHD‑3), the following syndromes are classified as TACs:
the age at onset in women with secondary chronic cluster
• Episodic and chronic cluster headaches
headache (cluster headache that was episodic at onset and
• Episodic and chronic paroxysmal hemicrania
later became chronic) did not differ much from those
with episodic cluster headache. In patients with chronic • Hemicrania continua
cluster headache who had onset prior to 16 years of age • Short-lasting unilateral neuralgiform headache attacks
or after 49 years of age, the traditional male to female with cranial autonomic symptoms (SUNA-syndrome)
ratio was inverted15. Thus, the clear male predominance • Short-lasting unilateral neuralgiform headache
in cases with onset in the central age groups became attacks with conjunctival injection and tearing
(SUNCT-syndrome)
attenuated in the extreme age groups.
2 | ARTICLE NUMBER 18006 | VOLUME 4 www.nature.com/nrdp
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
PRIMER
calcium voltage-gated, P/Q‑type, α-1A subunit) for Pathogenesis of peripheral origin
paroxysmal characteristics31 and a number of clock genes Proposed model of cavernous sinus involvement. Several
for rhythmicity, such as PER3, and the T3111C and characteristics of cluster headache attacks are consistent
3092 T>C polymorphisms in CLOCK32–34. with pathology in the region of the cavernous sinus,
ADH4 (encoding alcohol dehydrogenase 4) has mainly the triad of a predominantly trigeminal pain
been studied in patients with cluster headache in light distribution, parasympathetic hyperactivity and sympa
of the identification of alcohol as a trigger for attacks35. thetic deficits. Indeed, the cavernous sinus is the only
One study identified a positive association between the peripheral site where trigeminal C‑fibres (which have
ADH4 rs1126671 single nucleotide polymorphism (SNP) a role in the transmission of nociceptive information
and the risk of cluster headache in an Italian cohort 35; to the central nervous system) and sympathetic fibres
another study reported an association between the ADH4 can be affected by a single cause41. However, clinical
rs1800759 SNP and cluster headache36. However, these evidence for the involvement of the cavernous sinus in
findings were not confirmed in a recent large c ase–control cluster headache is lacking. For example, the frequency
cohort study in Sweden37. of abnormal findings observed at orbital venography
A recent genome-wide association study in a cohort in cluster headache was not higher than those in other
of 99 Italian patients with cluster headache and 360 age- forms of headache42,43, suggesting that the cavernous
matched, cigarette-smoking, healthy controls demon‑ sinus is unlikely to be the sole origin of pain in cluster
strated that ADCYAP1R1 (encoding pituitary adenylyl headache. Furthermore, no clinical or biochemical
cyclase-activating polypeptide type I receptor, also known evidence suggests a role of s ystemic inflammation in
as PACAP) and MME (encoding membrane metallo patients with cluster headache44.
endopeptidase, also known as neprilysin) variants were
associated with cluster headache susceptibility, suggesting Proposed vascular model. Another, albeit obsolete,
roles for genes implicated in pain processing 38. However, hypothesis is that cluster headache is a variant of
a case–control study in Sweden did not find an association migraine such that the vascular headaches in cluster
between cluster headache and ADCYAP1R1, MME or an headache are related to changes in intracranial and extra
intergenic variant on chromosome 14q21 (REF. 39). Thus, cranial blood vessels. Indeed, vasoconstricting ergot
additional exploration of specific gene abnormalities in alkaloid derivatives are effective for the treatment of
cluster headache is warranted, and additional studies with cluster headache45. However, neuroimaging studies
larger sample sizes are needed; hitherto, no gene has been using single-photon emission computed tomography
clearly associated with cluster headache. (SPECT) have yielded contradictory results, with stud‑
ies showing increased, decreased or unchanged cere‑
Mechanisms/pathophysiology bral blood flow in patients with cluster headache44,46–49.
Our understanding of the pathophysiology of cluster Furthermore, intracranial vasodilation has been pro‑
headache has advanced greatly owing to findings from posed to occur in cluster headache, although this is not
preclinical and clinical studies, clinical observations, specific as it also occurs in forehead pain50. Notably,
genetics and neuroimaging studies, but still remains exogenous histamine and other vasodilators (for exam‑
incompletely understood. Previously, cluster headache ple, alcohol, nitroglycerine and 5‑hydroxytryptamine 2B
was considered to be a type of vascular headache, but (5‑HT2B) agonists) can trigger cluster headache attacks
more recent evidence suggests that the pathophysio during cluster‑bout periods in patients51,52. This finding
logy of cluster headache involves the brain, trigemino‑ does not prove that vasodilatation is the initial event
vascular system and cranial parasympathetic system9,40. of c luster headache but suggests that vascular or other
Whether cluster headache pain originates peripherally changes generate a permissive state in the cluster head‑
or centrally remains controversial; both are hypotheses ache brain. Thus, vasodilation may be a trigger for the
of cluster headache pathophysiology. Collectively, the onset of cluster headache attacks, but it does not seem to
pathophysiology of cluster headache seems to involve be the primary cause.
the hypothalamus and pain-processing areas of the central
nervous system, as well as peripheral structures, such as Proposed trigeminal nerve model. According to the
the trigeminal nerve, parasympathetic nerves and c ranial trigeminal nerve model of cluster headache, activation
vasculature. However, changes in peripheral structures of the first division of the trigeminal nerve (that is,
(such as peripheral blood vessels) have a secondary role the ophthalmic nerve) by headache triggers — such as
in cluster headache pathophysiology. Structural and changes in weather, alcohol consumption, histamine
functional changes in the hypothalamus and other brain release and strong odours — produces severe uni
networks that transmit nociceptive information have also lateral headache. This activation of the trigeminal nerve
been implicated in cluster headache, and the functional leads to the reflex activation of parasympathetic effer‑
changes dynamically change between cluster-bout periods ents (through the trigeminal-autonomic reflex), which
and out-of-bout periods. Moreover, anatomical and func‑ produce autonomic symptoms, such as lacrimation,
tional links between the hypothalamus and brain areas rhinorrhoea and nasal congestion53.
that are traditionally not considered as pain processing In support of this model, triptans (particularly, suma
(for example, the occipital cortex and cerebellum) are triptan), which activate postsynaptic 5‑HT1B (causing
altered in cluster headache and may also contribute to intracranial vasoconstriction) and 5‑HT1D receptors
the pathophysiology. (inhibiting brainstem trigeminal neuron neurotransmitter
NATURE REVIEWS | DISEASE PRIMERS VOLUME 4 | ARTICLE NUMBER 18006 | 3
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
PRIMER
release), have been successfully used to treat acute cluster prophylaxis with corticosteroids63. Pretreatment with
headache attacks54. However, to date, no evidence sup‑ methylprednisolone could suppress IL‑1β, but not
ports that sumatriptan crosses the blood–brain b arrier prostaglandin E 2-induced CGRP release from cul‑
during acute attacks55, and whether triptans act through tured trigeminal ganglia neurons64, and a blockade of
an effect on peripheral trigeminovascular neurons or cytokine-mediated trigeminal activation may medi‑
predominantly through a central nervous system effect ate the preventive effect of methylprednisolone on
in the brainstem is debated56. Surgical lesioning of the cluster headache pathophysiology 64. However, despite
trigeminal nerve is not effective in patients with clus‑ increased levels of CGRP in cluster headache, similar
ter headache57, suggesting that the potentially central changes have been reported during migraine attacks
effects of sumatriptan on the trigeminal nucleus caudalis and during therapeutic lesioning of the trigeminal
(TNC; that is, the caudal region of the spinal trigeminal ganglion65,66. Thus, although the trigeminal nerve may
nucleus)58 are partly responsible for the success of this be involved in cluster headache, its activation alone
treatment in cluster headache, in addition to a possible cannot account for the disorder, and other factors are
peripheral trigeminovascular effect59. probably involved.
Other lines of evidence supporting the trigeminal The neuropeptide PACAP is pharmacologically
nerve model of cluster headache include increased levels similar to VIP, is involved in pain processing in animal
of markers of both trigeminal nerve and parasympa models and has been implicated in migraine patho‑
thetic activation. For example, increased expression genesis67. Indeed, the intravenous administration of
of calcitonin gene-related peptide (CGRP; a marker of PACAP in healthy individuals can induce migraine-like
trigeminal activation) and vasoactive intestinal peptide headaches68. Interestingly, one study demonstrated the
(VIP; a marker of parasympathetic neuronal activation) presence of PACAP in plasma during acute attacks in
have been found in jugular vein blood samples, ipsi‑ patients with cluster headache69. In addition, PACAP can
lateral to cluster headache attacks compared with out- induce activation of neurons in regions that are thought
of-bout periods and in healthy individuals60. Moreover, to be involved in cluster headache pathophysiology, such
CGRP is increased in the plasma of patients during as the superior salivatory nucleus, the sphenopalatine
acute cluster headache attacks compared with out- ganglion (SPG; a parasympathetic ganglion) and the
of-bout periods61, and increased plasma CGRP levels trigeminal ganglion70.
during nitroglycerine-induced attacks can be attenu‑ Studies using animal models have shown that stimu
ated by sumatriptan injection in patients62. In addition, lation of the pontine superior salivatory nucleus (SSN;
increased CGRP levels have been reported between which is the origin of cells in the parasympathetic vaso
headaches (interictally) in patients during a cluster- dilator pathway and contains cell bodies of neurons
bout period, which were reduced after short-term that innervate the salivary glands and a host of other
tissues) independently produces short-term neuronal
activation in the trigeminocervical complex (TCC),
Mechanical and nociceptive Higher brain which is associated with autonomic cranial symptoms,
input from face and neck Trigeminal centres
ganglion such as lacrimation and rhinorrhoea, and is inhibited
by oxygen treatment in cluster headache71,72. The TCC
consists of the dorsal horn of cervical spinal cord level 1
Vasodilation and level 2 and the TNC and acts as a relay centre that
conveys nociceptive information from the head and
TCC neck to higher brain regions, such as the thalamus.
In addition, the SSN receives direct projections from
TNC the paraventricular hypothalamic nucleus, which might
Lacrimation
modulate trigeminovascular nociceptive processing 73.
C1 Neurons from the SSN project to the SPG, which is
associated with cranial pain and autonomic symptoms,
C2 SSN such as lacrimation and rhinorrhoea, and mediate the
Rhinorrohea trigeminal-autonomic reflex 40 (FIG. 1). Indeed, studies
have suggested that the activation of postganglionic
SPG SPG neurons mediates the dilation of local meningeal
vessels and the activation of trigeminal nociceptive
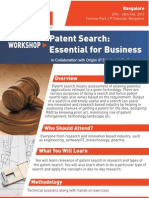
Figure 1 | Schematic pathway representation summarizing the trigeminal-
Nature Reviews | Disease Primers fibres40. The activation of trigeminal nociceptive fibres
parasympathetic reflex. In patients with cluster headache, autonomic symptoms are can also trigger a reflex connection in the SSN, which
thought to be mediated through the trigeminal-autonomic reflex. The trigeminal nucleus contributes to increased cranial parasympathetic activ‑
caudalis (TNC) is connected to the superior salivatory nucleus (SSN), from which
ity mediated by the SPG74,75. Consequently, SPG stimu‑
parasympathetic efferent fibres of the facial nerve arise. During the trigeminal-
lation is minimally invasive and a potentially effective
autonomic reflex, activation of the trigeminal nerve is thought to lead to activation of
parasympathetic efferents, producing autonomic symptoms such as lacrimation, treatment option for patients with intractable chronic
rhinorrhoea and nasal congestion. These parasympathetic efferents originate in the SSN cluster headache (see Neuromodulation, below)76–79.
synapse with postganglionic fibres that innervate the dural vessels in the sphenopalatine Of note, purely peripheral activation of the cranial
ganglion (SPG), resulting in vasodilation. C1, C1 cervical nerve; C2, C2 cervical nerve; parasympathetic system is not sufficient to cause cluster
TCC, trigeminocervical complex. headache attacks80–82.
4 | ARTICLE NUMBER 18006 | VOLUME 4 www.nature.com/nrdp
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
PRIMER
Although the above data suggest peripheral involve‑ In addition, white matter microstructural differences
ment in the pathogenesis of cluster headache, such have been reported in frontal pain modulation areas
theories cannot explain the cyclical recurrence of this during the cluster-bout period in patients with cluster
disorder. Indeed, cluster headache‑specific features, headache compared with healthy controls, and these
such as circadian and circannual rhythmicity, and changes mostly persisted during out-of-bout periods97.
behavioural features, such as agitation and restlessness, Probabilistic tractography showed consistent anatom‑
during acute attacks might be attributable to central ical connections between the altered areas (between
rather than p
eripheral mechanisms. the cluster-bout periods and out-of-bout periods) and the
hypothalamus, suggesting that these connections explain
Pathogenesis of central origin the shift between the two periods. Further research is
The pain network. Pain is a complex, multifactorial and required to determine the association. The discrepancies
subjective experience that involves a large distributed in the DTI studies may be attributable to differences in
brain network including both sensory–discriminatory study populations at the time of scanning (for example,
and affective–cognitive evaluative neuroanatomical during cluster bouts or between c luster-bout periods).
components83. Several neurophysiological studies have
shown altered pain perception and decreased pain Hypothalamus. The regularity and seasonal pattern of
thresholds in patients with cluster headache, suggesting cluster headache (with a peak in occurrence of attacks in
dysfunction of the pain control system84–87. Furthermore, the autumn and spring), in conjunction with a relapsing–
neurophysiological studies have implicated deficits in remitting presentation and ipsilateral cranial autonomic
supraspinal pain control, such as the diffuse noxious features, suggest that cluster headache may be related
inhibitory controls (neuronal pathways that underlie to alterations in the biological clock, such as that found
the physiological inhibition of pain by another pain‑ in the hypothalamus98,99. In addition, several other lines
ful stimulus) in cluster headache88,89. Dysfunction of of evidence, including data from anatomical, neuro
the descending pain control system may facilitate pri‑ imaging, hormonal and genetic studies implicate the
mary headache disorders, including cluster headache, hypothalamus in the pathophysiology of cluster head‑
by disinhibiting or facilitating n ociceptive signalling 90. ache. For example, patients with cluster headache often
Functional imaging studies have demonstrated dys‑ have neuro-endocrinological changes such as a blunted
function of the pain modulatory system in cluster head‑ circadian testosterone rhythmicity and abnormal levels
ache91,92. Indeed, studies using 18F-fluorodeoxyglucose of other hormones regulated by the hypothalamus,
PET showed increased glucose metabolism in frontal including cortisol, growth hormone, thyroid-stimulat‑
brain areas (such as the perigenual anterior cingulate ing hormone, prolactin, melatonin, follicle-stimulating
and prefrontal cortices) in addition to the thalamus, hormone and luteinizing hormone99,100.
posterior cingulate, insular cortex and temporal c ortex Several neuronal connections exist between the hypo‑
during cluster-bout periods compared with out-of- thalamus and regions of the trigeminovascular system
bout periods in patients with episodic cluster headache, (FIG. 2). Studies in rodents have shown that the hypothala
suggesting that dynamic functional differences in c entral mus receives sensory input, including nociceptive infor‑
descending pain modulation between cluster‑bout mation, from areas of the face and cranium innervated
(interictally between headaches) and out‑of‑bout by the trigeminal nerve via the trigeminohypothalamic
periods may facilitate attacks91. tract 101,102. Additionally, the posterior hypothalamus is
In addition, studies using T1 voxel-based morpho‑ a physiological modulator of TNC neuronal activity 103.
metry (VBM) have demonstrated grey matter volume Interestingly, disturbances in the hypothalamic–orexin
reductions in the middle frontal gyrus, left superior system have been associated with cluster headache patho
gyrus and medial frontal gyrus during cluster-bout physiology 104. For example, injection of orexin A into
periods in patients compared with healthy controls93. the posterior hypothalamus of rats activates neurons in the
Furtherm ore, grey matter volume increases were TNC, whereas the injection of orexin B inhibits activity
observed in the left anterior cingulate, insular cortex and in the TNC24. In addition, one study showed decreased
fusiform gyrus during cluster-bout periods compared levels of orexin A in the cerebrospinal fluid of patients
with out-of-bout periods. Thus, these dynamic changes with cluster headache during cluster-bout periods105,
in grey matter volume may reflect insufficient capacity which may be due to decreased function of the hypo‑
for pain modulation in frontal areas in episodic clus‑ thalamic descending antinociceptive pathway or may
ter headache that are p otentially associated with cluster represent an epiphenomenon of pain affecting hypotha‑
headache pathophysiology. lamic activity 105. The evidence for potential involvement
Studies using diffusion-tensor imaging (DTI) to of the orexin system in cluster headache pathophysiology
investigate white matter microstructural changes in is supported by human genetic association studies, which
patients with cluster headache have offered contradic‑ have revealed an association between a polymorphism of
tory findings94–96. One study revealed the absence of HCRT2 and risk of cluster headache26.
white matter diffusivity abnormalities compared with Increased ipsilateral posterior hypothalamic activ
healthy controls94, although two other studies reported ation has been observed in patients with cluster head‑
widespread white matter microstructural changes in the ache during nitroglycerine-triggered attacks compared
brain, particularly in the pain network, such as the fron‑ with both out-of-bout periods and with healthy individ‑
tal lobe, parietal lobe, temporal lobe and thalamus95,96. uals106,107. In addition, similar hypothalamic activation
NATURE REVIEWS | DISEASE PRIMERS VOLUME 4 | ARTICLE NUMBER 18006 | 5
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
PRIMER
Regions that are altered during acute attacks
Regions that are altered interictally
(between headaches) S1
Regions that are altered between cluster-bout
periods and out-of-bout periods
ACC
OCC
PFC INS
THA
AMYG
HYP
PAG CERE
Sensory and TG LC
nociceptive SSN
input from the
dural vessels, Trigeminal nerve NRM
face and head
TNC
Lacrimation,
rhinorrhoea and SPG
nasal congestion Parasympathetic division
of the facial nerve
Figure 2 | Schematic peripheral and central pathway representation summarizing the pathogenesis of cluster
headache. Pain and autonomic features in cluster headache probably arise from activation Nature Reviews structures,
of peripheral | Disease Primers
such as the trigeminovascular system. The pathophysiology initially involves structural and functional changes in the
hypothalamus and specific brain networks that transmit nociceptive input, and these functional changes can differ
between cluster‑bout and out-of-bout periods. In addition, anatomical and functional links between the hypothalamus
and brain areas that are traditionally not considered to be involved in pain processing (such as the occipital cortex
(OCC) and cerebellum (CERE)) are altered in cluster headache and may have contributory roles in its pathophysiology.
ACC, anterior cingulate cortex; AMYG, amygdala; HYP, hypothalamus; INS, insular cortex; LC, locus coeruleus; NRM,
nucleus raphe magnus; PAG, periaqueductal grey; PFC, prefrontal cortex; S1, primary sensory cortex; SPG, sphenopalatine
ganglion; SSN, superior salivatory nucleus; TG, trigeminal ganglion; THA, thalamus; TNC, trigeminal nucleus caudalis.
Adapted from REF. 111, Sage.
was observed in a patient with a spontaneous attack108,109. Other brain structures. Brainstem nuclei, including the
In addition, bout-independent bilateral grey matter vol‑ locus coeruleus and dorsal raphe nucleus (which modu‑
ume increases have been reported in the hypothalamus late vascular activity and pain input from the trigeminal
of patients with cluster headache106,110. These findings nucleus), have been implicated in cluster headache patho‑
are under debate as some groups could not repro‑ genesis119,120. The dysfunction of related monoaminergic
duce them111, whereas another study recently did110. The pathways, which is related to brainstem descending pain
use of different MRI sequences and procedures for image modulation (noradrenaline and 5‑HT as neurotrans
processing may partly explain this discrepancy. Proton mitters), may link the hypothalamus and brainstem in
magnetic resonance spectroscopy studies have prov cluster headache121 (FIG. 2).
ided additional evidence in support of hypothalamic Altered intrinsic fluctuations in sensorimotor and pri‑
dysfunction in c luster headache: low N‑acetylaspartate mary visual networks have been reported in patients dur‑
to creatine ratios in the hypothalamus of patients with ing out‑of‑bout periods, suggesting that these functional
cluster headache were found, which again supports changes extend beyond the antinociceptive system of the
hypothalamic dysfunction in the pathophysiology 112,113. brain122. In addition, abnormal functional connectivity
Further evidence supporting the role of the hypothal‑ between the hypothalamus and areas associated with pain
amus in cluster headache pathophysiology stems from processing and visual networks, such as the sensorimotor
neuromodulation. Deep brain stimulation (DBS) of the and the primary visual networks, has been reported dur‑
posterior hypothalamus has been evaluated for the treat‑ ing and between attacks122. Bout-dependent changes in
ment of intractable chronic cluster headache114–117 and hypothalamic dynamic functional connectivity with
leads to improvement in ~60% of patients115, although regions of the frontal and occipital lobes and the cere‑
ongoing attacks are unaffected (see Neuromodulation, bellum and cerebellar areas have also been reported in
below)118. patients with cluster headache123. Additionally, a decrease
6 | ARTICLE NUMBER 18006 | VOLUME 4 www.nature.com/nrdp
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
PRIMER
in functional co‑activation of the hypothalamus and sali‑ spring and autumn7. The circadian and circannual rhyth‑
ence network areas in patients with cluster headache has micity is preserved in chronic cluster headache136. The
been observed, suggesting the association with the defec‑ average number of daily attacks ranges from two to four,
tive central pain control pathway and autonomic nervous with a mean duration of ~100 minutes for untreated
system dysregulation124. Dynamic functional connectiv‑ attacks. In individuals with episodic cluster headache,
ity in the frontal and dorsal attention networks between the average duration of a cluster period is 8–9 weeks,
cluster‑bout periods and out-of-bout periods in patients and patients experience an average of one to two cluster
with cluster headache has also been reported, implicating periods per year.
these changes in discrete cortical areas within networks Commonly reported trigger factors for cluster attacks
outside traditional pain-processing areas125. include sleep, alcohol consumption, relaxation, warmth,
As previously mentioned, behavioural disturbances, stress, high altitude and changes in weather. Indeed,
including agitation and restlessness, are frequently in a questionnaire-based study of 275 individuals with
observed in patients during attacks9; these symptoms are cluster headache, 80% reported sleep as a trigger for their
thought to be associated with the autonomic fight‑or‑ attacks28. Alcohol can trigger cluster attacks in 50–80% of
flight response rather than a reaction to pain126,127. Pre patients and, accordingly, some individuals with c luster
vious studies have suggested the association between the headache avoid alcohol completely 137.
cerebellum and the motor agitation128,129. Furthermore,
trigeminal nociceptive processing has been reported in Diagnostic evaluation
the cerebellar lobules V and VI, ipsilateral to the stimulus, Diagnostic criteria for cluster headache are available
suggesting that the cerebellum might have a functional from the ICHD‑3 (REF. 138) (BOX 2). Cluster headache is
influence on nociceptive and trigeminal processing 130. subcategorized into episodic and chronic forms based on
Cluster headache‑related functional changes in the cere‑ whether cluster-bout periods are separated by pain-free
bellum have been demonstrated in recent imaging studies intervals (out-of-bout periods) that last at least 3 months.
and implicated in acute attacks131. Thus, we hypothesize The official classification, including several translations,
that alterations in the activity or connectivity of the cere‑ can also be found online139.
bellum may be associated with agitation or restlessness in The diagnosis of cluster headache is based on the
cluster headache. Further research is required to confirm patient’s symptoms and the exclusion of a secondary
this hypothesis and may reveal neuromodulatory targets headache. As secondary headaches that have a clus‑
for specific symptoms. ter headache phenotype and primary cluster headache are
difficult to differentiate according to symptoms alone140,
Diagnosis, screening and prevention all patients with suspected cluster headache should
Cluster headache features undergo brain imaging to determine whether condi‑
The typical features of cluster headache have been tions are present that could cause a secondary headache
described in studies from Denmark, the United Kingdom, with a cluster phenotype. The recommended technique is
Germany and the United States, collectively including MRI with or without contrast enhancement and with fine
1,924 individuals7,132–134. These studies provide fairly con‑ slices through the region of the pituitary gland (as pitu‑
sistent results regarding the age of onset of cluster head‑ itary tumours can manifest with secondary headaches
ache, the number and duration of attacks, the number of with a cluster phenotype)141. If a pituitary gland lesion is
cluster periods per year, headache location and associated suspected or confirmed by imaging, laboratory testing
symptoms. Cluster attacks might begin with premonitory for levels of pituitary hormones is indicated. In addition,
features that occur 10–20 minutes before the attack and as many patients with cluster headache have attacks that
include pain symptoms in the same regions as the cluster wake them from sleep, some patients have sleep dis‑
headache pain, cranial autonomic symptoms and general turbances before the attacks142 and sleep disorders are
symptoms, such as difficulty concentrating and restless‑ common comorbid conditions, investigations for sleep
ness135. Pain intensity is consistently described as severe, disorders are often indicated (see Comorbidities, below).
and the most common headache locations are peri
orbital and retro-orbital, followed by temporal. The most Differential diagnosis. Cluster headache must be
common symptom associated with cluster headache is differentiated from other headache types that have
lacrimation (reported by >90% of patients), but other overlapping features, including other TACs (BOX 1), side-
common symptoms include conjunctival injection, nasal locked migraine (in which every migraine attack occurs
congestion and rhinorrhoea, irritability, motor a gitation, on the same side of the head) and secondary headaches
ptosis, eyelid swelling, forehead sweating and light sen‑ manifesting with a cluster phenotype. Although the
sitivity. Of note, in Asian individuals, lower frequencies symptoms of cluster headache are similar to those of
of restlessness (50%) have been reported c ompared to other TACs, they can be differentiated by the duration
western populations (>80%)5,6. and frequency of attacks and therapeutic response to
Circadian rhythmicity is reported by ~80% of indomethacin (TABLE 1). Hemicrania continua consists of
patients, and circannual rhythmicity is noted by >50%. continuous unilateral headache, although exacerbations
In the Danish study, the worsening of attacks or the onset of headache severity that are often associated with ipsi‑
of cluster-bout periods was most common at the end of lateral cranial autonomic features can occur episodi‑
autumn and the beginning of winter, but in the US study, cally; the continuous pain and the complete therapeutic
onset or worsening of attacks was most common in the response to indomethacin in patients with hemicrania
NATURE REVIEWS | DISEASE PRIMERS VOLUME 4 | ARTICLE NUMBER 18006 | 7
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
PRIMER
continua differentiate this disorder from cluster head‑ is variable between countries; the average time to diagno‑
ache138. Attacks of paroxysmal hemicrania, short-lasting sis was 2.6 years in the United Kingdom144, 4.6 years in
unilateral neuralgiform headache attacks with conjunc‑ Spain147, 5 years in the United States7, 5.3 years in Italy 148,
tival injection and tearing (SUNCT) and short-lasting 8 years in Taiwan5 and 11 years in Norway 4. In the US
unilateral neuralgiform headache attacks with cranial Cluster Headache Survey, 25% of patients were diagnosed
autonomic symptoms (SUNA) have key differences in within 1 year of symptom onset and 58% of patients were
their duration, frequency and response to indomethacin diagnosed within 5 years, but 22% were not diagnosed for
compared with cluster headache (TABLE 1). ≥10 years7. In that study, 79% of patients initially received
Occasionally, phenotypic overlap is apparent between an incorrect diagnosis, including migraine, sinusitis,
migraine attacks and cluster headache, such as in side- allergies or tooth-related issues7. Overlapping features
locked migraine, when migraine is associated with between cluster headache and migraine, such as the pres‑
ipsilateral cranial autonomic features and when cluster ence of aura, photosensitivity, phonosensitivity and side-
headache is associated with photophobia, phonophobia, shifting of headache (that is, from one side of the head to
nausea or vomiting 7,143. Characteristics that are consistent the other), probably c ontribute to misdiagnosis133,134,149.
with side-locked migraine rather than cluster headache
are the longer duration of untreated attacks with migraine Comorbidities
and the differences in patient activity during the attack Individuals with cluster headache should be screened for
(TABLE 1). As previously mentioned, secondary headaches possible comorbidities or other lifestyle factors, includ‑
with a cluster phenotype cannot be differentiated from ing smoking, alcohol abuse, illicit drug use, depression
primary cluster headache based on clinical features alone, and sleep disorders9.
and a diagnostic e valuation is required.
Smoking, alcohol and illicit drug use. As many as
Diagnostic challenges. In patients with typical cluster 70–90% of individuals with cluster headache smoke7,150.
headache symptoms, the phenotype should be easily Smoking is associated with more severe manifestations
recognized and the diagnosis of primary cluster head‑ of cluster headache (for example, longer cluster-bout
ache should be made after the exclusion of a secondary periods and more frequent attacks), although only 18%
headache. However, patients with cluster headache often of patients stopped smoking after cluster headache onset
experience delayed diagnosis or misdiagnosis, leading based on results from a US survey 7. Smoking cessation
to suboptimal and inappropriate treatments144,145. In one does not affect the course of the disorder 150,151. Different
study of 85 patients seen at the Danish Headache Center, studies have provided conflicting results regarding
the average delay between onset and diagnosis was whether the rates of alcohol use and abuse are higher
9 years, whereas in another survey of 351 patients within in individuals with cluster headache than the general
the Danish Headache Survey, the average time to diagno‑ population151,152. However, alcohol can trigger cluster
sis was 6.2 years and half of the patients initially received attacks in 50–80% of patients, making its use problem‑
the wrong diagnosis132,146. In general, the time to diagnosis atic within this population and leading some individuals
with cluster headache to avoid alcohol137. Illicit drug use
is more common in individuals with cluster headache
Box 2 | ICHD‑3 diagnostic criteria for cluster headache than in the general population153, although this observa‑
tion might be true only in men154. In an Italian study of
Cluster headache 210 patients (including 162 men) with cluster headache,
At least five attacks that fulfil the following criteria:
the rates of cannabis, opioids, cocaine, amphetamine and
• Severe or very severe unilateral orbital, supraorbital and/or temporal pain lasting ecstasy use were higher in those with cluster headache
15–180 minutes (when untreated)
than in the general population155. The use of illicit drugs,
• Either or both of the following: such as psilocybin and forms of lysergic acid, as self-
-- At least one of the following, ipsilateral to the headache: conjunctival injection
treatments is not uncommon for patients with cluster
and/or lacrimation; nasal congestion and/or rhinorrhoea; eyelid oedema;
headache156. However, some studies suggest that most
forehead and facial sweating; or miosis and/or ptosis
-- A sense of restlessness or agitation illicit drug users first used the drugs before the onset of
cluster headache155.
• Attacks have a frequency between one every other day and eight per day for more
than half of the time when the disorder is active (during cluster bouts)
Depression and other psychological comorbidities.
• Not better accounted for by another ICHD‑3 diagnosis
Depression is frequent in patients with cluster headache.
Episodic cluster headache Indeed, data from a population-based, cross-sectional
• Attacks fulfilling criteria for cluster headache and occurring in cluster bout periods study of 462 patients showed the lifetime prevalence
• At least two cluster-bout periods lasting from 7 days to 1 year (when untreated) of depression was 2.8‑fold higher in those with cluster
and separated by pain-free remission (out-of-bout) periods of at least 3 months headache compared with healthy individuals157. In addi‑
Chronic cluster headache tion, the 2.5‑year incidence of depression was 5.6‑fold
• Attacks fulfilling criteria for cluster headache higher in patients with cluster headache than healthy
• Occurring without a remission period, or with remissions lasting <3 months, individuals in a population-based follow‑up study
for at least 1 year using the Taiwan National Health Insurance database,
and more cluster-bout periods per year was a risk factor
ICHD‑3, International Classification of Headache Disorders138.
for depression158. In the US Cluster Headache Survey,
8 | ARTICLE NUMBER 18006 | VOLUME 4 www.nature.com/nrdp
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
PRIMER
Table 1 | Characteristics of cluster headache and other headache types that can have overlapping features
Headache Attack duration Attack frequency Behaviour Sex ratio Complete response
(if untreated) during an attack (female:male) to indomethacin
Cluster headache 15–180 minutes Once every other day, up to 8 times per Agitated 1:4 No
(typically 100 minutes) day (typically 3–4 per day)
Hemicrania continua Continuous Continuous Nonspecific 2:1 Yes
Paroxysmal 2–30 minutes ≥5 per day (typically 10 per day) Agitated 2:1 Yes
hemicrania (typically 15 minutes)
SUNCT and SUNA 1–600 seconds ≥1 per day or more (typically 60 per day) Agitated 1:1.5 No
(typically 1 minute)
Side-locked At least 4 hours Variable Avoid physical 3:1 No
migraine (typically 24 hours) movement
SUNA, short-lasting unilateral neuralgiform headache attacks with cranial autonomic symptoms; SUNCT, short-lasting unilateral neuralgiform headache attacks
with conjunctival injection and tearing.
55% of patients reported suicidal thoughts, and 2% had Although the existence and nature of the relation‑
attempted suicide7. Chronic cluster headache is associ‑ ship between cluster headache and sleep disorders are
ated with a higher prevalence of lifetime depression than not clearly understood, screening patients with cluster
episodic cluster headache157. Despite the high frequency, headache for sleep disorders is reasonable as sleep is a
the rates of diagnosis and treatment of depression are trigger for attacks. Several studies suggest sleep disorders
low in patients with cluster headache, e mphasizing the in patients, and some evidence suggests treating sleep dis‑
importance of screening for this condition157. orders can reduce cluster attack frequency for a subset
Whether anxiety and certain personality profiles are of patients.
more common in individuals with cluster headache is a
matter of debate. Although some studies have suggested Management
high rates of anxiety and obsessive-compulsive and The treatment of cluster headache is based on empiri‑
anti-social traits, other studies have found no differences cal data and only a few clinical trials. Pharmacological
between those with cluster headache and comparator treatment can be divided into acute attack abortion and
groups, including healthy controls159–162. Further stud‑ prophylaxis, and most patients receive both types of treat‑
ies are needed to define the psychological comorbidi ment. Several nonpharmacological treatments (excluding
ties of cluster headache and to assess how personality neurostimulation) have been trialled but are ineffective
traits might affect pain coping, quality of life and optimal in nearly all patients. Pharmacological treatment has a
treatment recommendations. placebo rate that is similar to that for migraine treatment
(~25%)166. International treatment guidelines are available
Sleep disorders. As cluster headache attacks are fre‑ for cluster headache167,168, and the superiority of guide‑
quently initiated during sleep, several studies have line-adherent treatment compared with non-guideline
evaluated patients with cluster headache for sleep dis treatment in cluster headache has been reported169.
orders28,133,163,164. Indeed, patients with cluster headache
had higher scores on the Pittsburgh Sleep Quality Index During an attack
than healthy individuals, which indicates a poorer self- Oxygen. The inhalation of pure oxygen is effective at
assessment of sleep quality 28. Patients who reported sleep aborting attacks170. Inhalation should start as soon as
as a trigger for their cluster attacks had higher scores possible but can commence at any point during the
than patients who did not report sleep as a trigger 28. One attack and should last for 15 minutes while the patient
polysomnography study showed a reduced percentage of is in a sitting, upright position. The oxygen should be
rapid eye movement (REM) sleep, longer REM latency delivered through a non-rebreather mask with reservoir
and fewer arousals in patients with cluster headache com‑ or, preferably, with a demand valve oxygen mask171. Apart
pared with healthy individuals164. No relationship was from chronic obstructive pulmonary disease, there are
observed between the occurrence of nocturnal attacks no common contraindications to oxygen therapy, as this
and a specific sleep stage164. therapy is safe and without relevant adverse effects170.
Whether sleep-disordered breathing is more common More than 70% of all patients with cluster headache
in patients with cluster headache is debated. In one study, respond to oxygen therapy with a substantial pain reduc‑
the rate of obstructive sleep apnoea was not higher in tion within 30 minutes170. Thus, oxygen is the first-choice
patients with cluster headache compared with healthy treatment for the abortion of cluster attacks, although
controls; however, sleep-disordered breathing was little is known about its mechanism of action71.
present in 80% of patients (using an apnoea-hypopnea
index cut-off of ≥5)163,164 and in 44% of patients (using Triptans. Subcutaneous injection of sumatriptan, a 5‑HT1B
an apnoea-hypopnea index cut-off of ≥10)163. A higher and 5‑HT1D agonist, can render 75% of patients pain-free
rate of obstructive sleep apnoea has been reported dur‑ within 20 minutes of injection and can be administered at
ing cluster-bout periods in patients with cluster headache any point during the attack172,173. Sumatriptan injections
than in healthy controls (29% versus 7%, P = 0.018)165. are safe and without adverse effects in most patients,
NATURE REVIEWS | DISEASE PRIMERS VOLUME 4 | ARTICLE NUMBER 18006 | 9
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
PRIMER
even with frequent use (including daily use for several period. The full effectiveness of verapamil can be expected
years), and their effectiveness is not reduced over time174. within 2–3 weeks after drug onset187. Slow-release formu‑
Contraindications are cardiovascular and cerebrovascular lations are available that enable fewer administrations per
disorders and risk factors including untreated arterial day. When patients initially start verapamil, corticoster‑
hypertension, hyperlipidaemia, diabetes mellitus, smok‑ oids are also administered by some clinicians for ~2 weeks
ing and old age. The most specific and unpleasant adverse to bridge the time period of dose escalation of verapamil.
effects are chest pains and distal paraesthesia, which can
occur in up to 10% of patients174. A zolmitriptan nasal Corticosteroids. There are no sufficiently powered ran‑
spray has been shown to reduce pain and accompany‑ domized, placebo-controlled trials for the use of oral
ing symptoms during attacks in two placebo-controlled corticosteroids in cluster headache, although they are
trials and has been approved by the European Medicines regarded as highly effective and several open-label stud‑
Agency (EMA) for the acute treatment of cluster head‑ ies and case series have been published and reviewed190.
ache175,176. A sumatriptan nasal spray 177,178 and oral zol‑ All studies showed the efficacy of the different regimens.
mitriptan therapy 179 have also shown efficacy within Corticosteroids are recommended for short-term use,
30 minutes in single, open-label and double-blind, such as for 2–3 weeks after onset of the cluster bout when
placebo-controlled trials. the rapid control of attacks is desired. Some patients are
attack-free only with steroid treatment, and continu‑
Ergotamine. Oral ergotamine has been used for the ous administration of steroids is rarely required by the
treatment of cluster headache attacks for >50 years and patient. Chronic use of corticosteroids is associated with
is probably effective within 15 minutes if administered high morbidity and, accordingly, caution and short-
early in the attack; however, placebo-controlled trials are course therapy should be used; corticosteroids should
lacking. Short-term prophylaxis using ergotamine is not be avoided for chronic cluster headache. In particular,
recommended because of severe adverse effects, such as the risk of opportunistic infections with corticosteroid
vasoconstriction, soft tissue necrosis, distal paraesthe‑ use should be carefully considered in medium to long-
sia and ulcers. Intranasal dihydroergotamine was not term use. At high doses, ~70–80% of patients respond
superior to placebo in a single trial at aborting attacks180, to steroids. The injection of corticosteroids at the greater
although intravenous administration was shown to abort occipital nerve has shown efficacy in placebo-controlled
severe attacks in an o pen-label retrospective181 and an trials for prevention191–193; this procedure is easy to per‑
open-label prospective182 trial. form, has a very low rate of adverse effects compared with
other treatments, and the effect can last for days.
Others. The nasal installation of lidocaine — a local
anaesthetic that blocks neuronal voltage-gated sodium Lithium. More than 20 open-label trials have evaluated
channels — is probably effective in at least one-third of the use of lithium carbonate for prophylaxis starting at
patients when administered within 15 minutes of attack the beginning of a cluster-bout period194. An attack fre‑
onset, although this has only been reported in open-label quency reduction of >50% has been reported in up to
trials183–185. Intranasal lidocaine is safe but might cause 78% of patients with chronic cluster headache and 63%
nasal discomfort; other adverse effects are unknown. of patients with episodic cluster headache194. However,
Subcutaneous octreotide is effective in the treatment one placebo-controlled trial did not show any efficacy of
of acute attacks in a double-blind, placebo-controlled lithium in the prevention of episodic cluster headache195,
trial when given within 15 minutes of attack onset 186. and one study showed a more rapid improvement in
No adverse effects were reported in this trial. Further t rials headache frequency and better tolerability for verapamil
are not ongoing. than lithium187. Liver, renal and thyroid function, in addi‑
tion to electrolyte levels, should be monitored regularly
Preventive treatments in patients using lithium as the major adverse effects are
Verapamil. Verapamil — a voltage-dependent calcium hypothyroidism, tremor and renal dysfunction194.
channel blocker — is the first drug of choice for the
prophylaxis of episodic and chronic cluster headache in Anticonvulsants. Two open-label trials have suggested
most countries. Although only a few sufficiently powered a moderate efficacy of valproic acid for prevention196,197,
double-blind, controlled trials have been conducted, they although one controlled study did not show a difference
demonstrate that ~70% of patients are responders9. In one compared with placebo198. The scientific evidence is that
controlled trial, verapamil was shown to have a more rapid valproic acid has no proven efficacy in either episodic or
action of onset than lithium, although both drugs showed chronic cluster headache because the controlled trial was
efficacy in attack prophylaxis compared with placebo187. negative but can be tried as a third-line drug in patients
In another trial, verapamil was superior to placebo188. who do not respond to verapamil or lithium. On the basis
Adverse effects of verapamil are bradycardia, oedema of of results from open-label studies, other anticonvulsants,
the legs, constipation, gastrointestinal discomfort, gingi such as topiramate199,200 and gabapentin201,202, have a
val hyperplasia and dull headache. As verapamil can probable efficacy in the prophylaxis of episodic and
increase cardiac conduction time, regular electrocardio chronic cluster headache. The main adverse effects of
graphy (ECG) testing is necessary 189. Verapamil should topiramate are cognitive disturbances, paraesthesia and
be administered for ~1.5 times of the assumed duration weight loss, and this drug is contraindicated in patients
of the cluster-bout period, starting at the beginning of the with nephrolithiasis.
10 | ARTICLE NUMBER 18006 | VOLUME 4 www.nature.com/nrdp
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
PRIMER
Other therapies. The pre-emptive or prophylactic use of noninvasive vagus nerve stimulation (VNS) (FIG. 3)),
triptans in patients with cluster headache remains contro‑ which have given new hope to patients with refractory
versial. In one study, sumatriptan administered orally was cluster headache. However, large sham-controlled trials
not effective in preventing attacks in a placebo-controlled are scarce, and data from some open-label studies have
trial203, although in open-label trials, eletriptan204 or nara to be confirmed.
triptan205 reduced the number of attacks in patients with
episodic cluster headache. SPG stimulation. Invasive techniques are g enerally con‑
The ipsilateral intranasal application of capsaicin sidered when patients fail to respond to usual pharmaco
has been studied in two open-label trials206,207 and one logical therapies (and/or have intolerance to these
double-blind, placebo-controlled208 trial, and showed treatments)221,222. The rationale for the use of SPG stimu‑
an efficacy in approximately two-thirds of patients with lation in cluster headache was based on the strong cranial
episodic cluster headache after repeated application in ipsilateral autonomic features that are frequently observed
all trials. Also, the intranasal application of civamide (cis-during attacks (see Mechanisms/pathophysiology, above)
capsaicin) showed moderate efficacy in a double-blind, and from data from pilot studies77. In the seminal ran‑
placebo-controlled study in patients with episodic cluster domized controlled trial (Pathway CH‑1)78, 28 patients
headache209. However, although these studies are categor with refractory chronic cluster headache received surgi‑
ized as blinded, the nasally applied treatments irritate the cal implantation of a stimulation device into the pterygo
mucosa. No evidence suggests that a combination of palatine fossa (in which the SPG is located). The devices
prophylactic drugs is superior to single use; however, this could be remotely controlled by the patient and could ran‑
question has not yet been systematically studied. domly deliver one of three different stimulation patterns
when activated (no stimulation or sham, subthreshold
Third-line treatments. Several treatments can be con‑ stimulation, or full stimulation). Pain relief was reported
sidered for refractory cluster headache. Methysergide — in 67.1% of attacks treated with full-dose stimulation
a 5‑HT receptor antagonist — has been successfully used and in 7.4% of attacks with sham stimulation; pain free‑
as a prophylactic drug for episodic cluster headache but is dom within 15 minutes of stimulation was achieved in
no longer manufactured. However, this issue may change 34.1% of attacks with full-dose stimulation and in 1.5% of
as the licence for drug production is still valid. Oral mela attacks with sham stimulation. The acute responder rate
tonin was effective in reducing attack frequency in a was 32%, and 43% of patients reported a ≥50% reduction
single double-blind, placebo-controlled study in patients in attack frequency compared with baseline78. Adverse
with episodic cluster headache210 but did not provide any events related to maxillofacial surgery were frequent
additional efficacy when used as an adjunctive therapy to (such as pain, swelling and haematoma), but most of the
standard treatment in patients with refractory disease211. events were fully reversible. Furthermore, 81% of patients
Warfarin was reported to effectively reduce attack fre‑ had sensory disturbances in the region of the face inner‑
quency in a small controlled trial and in case reports of vated by the maxillary nerve (likely because this nerve is
patients with episodic cluster headache212,213 but should located near the SPG), but these were mostly reversible.
not be used as a treatment given its adverse effect pro‑ Six patients had to be re‑intervened.
file (including bleeding). Weak evidence from a small The Pathway CH‑1 study was followed by an open-label
open-label study showed the efficacy of baclofen214 trial involving 33 patients with chronic cluster headache
in prophylaxis, and another open-label study showed no who had 5,956 cluster attacks over 24 months79. In this
evidence for transdermal clonidine215 in prophylaxis of trial, 30% of patients had ≥1 out-of-bout period(s) lasting
episodic cluster headache. ≥1 month (that is, they evolved to an episodic cluster head‑
ache form)223, 65% of attacks were successfully relieved by
Unsuccessful treatments. Candesartan is effective in SPG stimulation and pain freedom was obtained in 50% of
migraine treatment but was not effective in a placebo- attacks. The 50% acute responder rate was 45%, and 35%
controlled trial in cluster headache prophylaxis216. Patients of evaluable patients had an attack frequency reduction of
with episodic cluster headache did not benefit from ≥50% compared with baseline after 24 months. Headache
botulinum toxin type A injections for prophylactic treat‑ frequency increased in 35% of patients and remained
ment217,218, but there might be some prophylactic benefit stable in 29%. Because the study was designed to assess
following onabotulinumtoxinA administered to the SPG the efficacy of SPG stimulation in acute therapy in those
in patients with chronic cluster headache219. Hyperbaric with chronic cluster headache, a continuous monitor‑
oxygen inhalation is not effective in preventing attacks ing of attack frequency was not available in the Pathway
in episodic or chronic cluster headache220. Cannabis, CH‑1 study or the follow-up. Patients were asked to
other cannabinoids and similar psychotropic drugs are record their average attack frequency (in the past 4 weeks)
frequently used by patients with cluster headache153, every 3 months. Accordingly, further studies are needed
but self-reported effectiveness is very low 154. to determine the long-term effect of SPG stimulation
on attack frequency in chronic cluster headache.
Neuromodulation
Substantial progress has been achieved in the manage‑ Invasive ONS. Invasive ONS is being used for refrac‑
ment of cluster headache using invasive and noninvasive tory headache management and has been assessed for
neuromodulation techniques (such as SPG stimulation, cluster headache prevention in several open-label stud‑
invasive occipital nerve stimulation (ONS), DBS and ies224–229. Although most trials reported encouraging
NATURE REVIEWS | DISEASE PRIMERS VOLUME 4 | ARTICLE NUMBER 18006 | 11
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
PRIMER
Hypothalamic DBS SPG stimulation
Hypothalamus
Greater occipital nerve SPG
Facial
Invasive ONS nerve Noninvasive VNS
Vagus
nerve
Figure 3 | Neuromodulation therapies for cluster headache. Neuromodulation methods that have been investigated
Nature Reviews
for the treatment of cluster headache. For example, postganglionic neurons of the sphenopalatine | Disease
ganglion (SPG) Primers
have
been implicated in cluster headache-associated pain and autonomic features, and SPG stimulation has been shown to
effectively abort cluster headache attacks and to reduce the frequency of attacks in some patients78,79. Invasive occipital
nerve stimulation (ONS) has been evaluated for the prevention of cluster headache owing to the anatomical overlap
between the trigeminal and cervical afferents, which is consequently termed the trigeminocervical complex, and
accordingly, ONS could modulate antinociceptive activity in the trigeminocervical complex and the pain network257.
The vagus nerve is a mixed motor and sensory nerve with projections to brain areas involved in pain modulation, including
the trigeminal nucleus caudalis. Accordingly, noninvasive vagus nerve stimulation (VNS) has been suggested to inhibit
nociceptive processing258 and has proved effective mainly in episodic cluster headache acute therapy. Hypothalamic deep
brain stimulation (DBS) has been investigated for the prevention of cluster attacks owing to clinical and neuroimaging
data, which proved the implications of hypothalamic function in the pathophysiology and the circadian and circannual
manifestations of this condition. Figure adapted from REF. 259, Macmillan Publishers Limited.
results with follow‑up periods of several years, sham- Hypothalamic DBS. DBS targeting the hypothalamus is
controlled trials of invasive ONS in cluster headache pre‑ a neuromodulation technique that has been used to treat
vention have not been carried out. Overall, the open-label drug-refractory patients with cluster headache116 and is
trials have included 172 patients with chronic cluster based on the activation of the posterior hypothalamus
headache, usually those with drug-refractory forms224–229. during attacks107. Several case series have been published
The attack frequency improved in ~58.1% of patients, but over the past 20 years with encouraging results, includ‑
most patients also required concomitant pharmacological ing a reduction in attack frequency and intensity 234, but
prophylaxis. Similar to SPG stimulation, evolution from a significant risk of serious adverse events, including a
chronic to episodic cluster headache has been described fatal haemorrhage, has been reported235. Only one hypo‑
with invasive ONS in 10–40% of patients. Despite a reduc‑ thalamic DBS trial included a sham group117, and no
tion in the attack frequency, invasive ONS had little or no differences were observed between the active and sham
effect on the intensity of attacks or the duration of pain230. procedures in patients with chronic cluster headache,
Stimulator-related adverse events are quite common although the duration of the sham period might have been
with this treatment, mainly lead migration or device too short to detect a change. In the subsequent open-label
infection, and battery depletion may require replace‑ phase of this trial, the mean attack frequency improved in
ment surgeries in up to 100% of patients. Other adverse 6 out of 11 patients.
events include paraesthesia induced by the stimulation, Some controversies regarding the accuracy of the
which cannot be tolerated by some patients. In addition, hypothalamic DBS stereotactic coordinates and the struc‑
at least two long-term trials of up to 10 years in duration tures that are modulated have led to new trials based on
have described a tolerance phenomenon with invasive different techniques236–238. The aim of these trials was also
ONS228,231, which required the adjustment of the stimu‑ to reduce the risk of serious adverse events. One study
lation parameters and could be related to neuroplasticity used a modified target in five patients239, and another
in the opioid system232. A large multicentre randomized study evaluated DBS of the ventral tegmental area (VTA)
controlled trial is currently underway to evaluate invasive in 21 patients with chronic cluster headache114. The ration‑
ONS for prevention of cluster headache (ICON study 233). ale of using the VTA for DBS was based on imaging studies
12 | ARTICLE NUMBER 18006 | VOLUME 4 www.nature.com/nrdp
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
PRIMER
in patients previously treated with hypothalamic DBS that the standard of care group. An estimation of adherence
showed a maximal activation that was centred over the to therapy was 64% in the controlled phase (that is, 64%
VTA114. The median daily attack frequency decreased by of patients performed ≥80% of the recommended treat‑
60%, and 52% of patients had a 50% reduction in median ment sessions). Further evidence is needed to confirm the
frequency of attacks114. The feasibility and efficacy of endo usefulness of n
oninvasive VNS in attack prevention.
ventricular hypothalamic DBS using a floating electrode
that stimulates the floor of the third ventricle was reported Quality of life
in seven patients with chronic c luster headache240. Given the intense pain of cluster headaches, surprisingly
few studies have investigated the effect of the disorder on
Noninvasive VNS. Noninvasive VNS is the only non quality of life. Some studies suggest that patients have a
invasive neuromodulation technique that has been poorer quality of life during active cluster bouts than the
evaluated in cluster headache. In the ACT‑1 randomized general population and that the impairment is greater
controlled trial, 133 patients (of whom two-thirds had epi‑ in patients with an older age of onset 244. No difference
sodic cluster headache), were asked to use noninvasive was reported in the quality of life of patients during
VNS to treat five attacks each241. A trend to pain relief or cluster-bout periods in those with episodic compared
pain freedom was reported in patients who received the with chronic cluster headache244. During the out-of-
active treatment compared with the sham, and a signifi bout period in patients with episodic cluster headache,
cant difference was observed in patients with episodic clus‑ quality-of-life scores tended to improve and were similar
ter headache. In addition, exploratory efficacy end points to scores in those who are headache-free245,246, although
(such as pain freedom at 15 minutes and changes in attack other studies have reported high levels of disability in
duration) were significantly improved in the episodic clus‑ patients with episodic chronic headache during out-of-
ter headache subpopulation. The ACT‑2 study provided bout periods146,247. The degree of impairment that contin‑
similar results: noninvasive VNS was superior to sham ues beyond the cluster-bout period might be attributed to
in the episodic cluster headache subgroup only 242. The the unpredictability of the next cluster bout.
open-label controlled PREVA study evaluated the use of The consequences of cluster headache have been
noninvasive VNS add‑on therapy twice daily (to a total underlined by a recent US survey, which revealed that
of 12 minutes) for 1 month in 97 patients with chronic ~20% of patients had lost their job secondary to clus‑
cluster headache compared with patients who continued ter headache and 8% were unemployed7. One study in
their usual pharmacological prophylaxis (standard of Denmark reported that 16% of patients had lost their
care group)243. In the intention-to‑treat analysis, a mean job, and 8% needed early retirement; this occurred in
change in weekly attack frequency of −5.9 was reported episodic and chronic cluster headache146. Given that
in the noninvasive VNS group compared with −2.1 in most attacks occur during the night, a major problem in
patients is sleep deprivation. Generally, up to one-third of
patients found that the disorder limited their career 146,247.
Table 2 | Selected planned or ongoing trials in patients with cluster headache Compared with migraine, in which several question‑
Treatment Stage ClinicalTrials.gov naires that measure the impact or disability of headache
identifier have been validated, only one scale has been developed
Pharmacological for cluster headache248. This scale assesses the restriction
on activities of daily living, the impact on mood and
Psilocybin Phase 1 NCT02981173 interpersonal relationships, pain and anxiety, and lack of
Botulinum toxin type A Phase 1–2 NCT03066635 vitality 248. However, using the Headache Impact Test‑6
R‑Verapamil Phase 2 NCT02209155 (HIT‑6) scale, 74% of patients with cluster headache were
SOM230 Phase 2 NCT02619617
classified as severely affected (HIT‑6 grade IV disabil‑
ity)249, with 78% of patients reporting restrictions in daily
Sodium oxybate Phase 3 NCT02637648 living and 96% needing to make a lifestyle change146. Social
Fremanezumab Phase 3 NCT03107052 and leisure activities, family life and housework were dis‑
Civamide nasal solution Phase 3 NCT01341548 rupted. Agoraphobic symptoms have been reported in
33% of patients, depressive symptoms in 56% of patients
LY2951742 Phase 3 NCT02397473
and suicidal tendencies in 22% of patients247,249. In general,
LY2951742 (galcanezumab) Phase 3 NCT02797951 patients live in fear and uncertainty because of their con‑
TEV‑48125 Phase 3 NCT02945046 dition250, and patients have high levels of self-aggression
TEV‑48125 (fremanezumab) Phase 3 NCT02964338 and depression, which correlates with greater emotional
and functional impairment251. Self-aggression and depres‑
Acetium Not provided NCT02310828
sion substantially impair the patient’s life and, accordingly,
Neuromodulation should be c onsidered as important therapeutic targets.
Occipital nerve stimulation Phase 3 NCT01151631
SPG stimulation Not provided NCT02510729 Outlook
In the past 20 years, great advances in our understanding
Deep brain stimulation V3 Not provided NCT02782533
of the pathophysiology of cluster headache have come
US‑guided greater occipital nerve injection Not provided NCT02031822 from findings in the central and peripheral nervous sys‑
SPG, sphenopalatine ganglion; US, ultrasound. tems. The vascular model, involving an inflammation of
NATURE REVIEWS | DISEASE PRIMERS VOLUME 4 | ARTICLE NUMBER 18006 | 13
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
PRIMER
the walls of the cavernous sinus, has been rendered out‑ therapies are under study, including neuromodulation
dated by the recognition that the neurovascular phenom and pharmacological therapies (TABLE 2).
ena and a hypothalamic impulse generator, or ‘oscillator,’ As previously mentioned, circulating levels of CGRP
seem to be more important. However, at present, the are increased during attacks62, suggesting a key role for
molecular and genetic background of cluster headache this system in cluster headache. Several selective CGRP
remains largely unknown, possibly due to the low receptor antagonists are under development and seem to
prevalence compared with migraine. be effective in inhibiting nociceptive trigeminal process‑
Hypothalamic DBS has been used for the treatment ing in both animal models and patients252,253. However,
of drug-refractory chronic cluster headache and can the development of some older CGRP receptor antago
decrease attack frequency in 60% of patients. However, nists has been halted because of severe adverse effects,
DBS is an invasive technique that is associated with seri‑ such as hepatotoxicity 254. The more recent and prom‑
ous complications in some patients116; accordingly, other ising development of monoclonal antibodies targeting
minimally invasive or noninvasive neurostimulation tech‑ free CGRP and CGRP receptors has enabled clinicians to
niques, such as SPG stimulation and noninvasive VNS, circumvent these adverse effects. These antibodies have
have been evaluated in patients with cluster headache230. promising efficacy in patients with migraine255,256 and are
Although these techniques have demonstrated efficacy in likely to be effective in cluster headache, although these
several trials, most trials have been open-label studies or trials are still ongoing. Future development of monoclonal
have included only a limited number of patients in the antibodies and pharmacological agents targeting CGRP
placebo (sham) group. Accordingly, double-blind, ran and possibly PACAP might improve the clinical manage‑
domized controlled studies with long-term outcomes are ment of cluster headache. Further studies to identify new
needed to expand the repertoire of therapeutic options for biomarkers other than CGRP, accompanied by supportive
treating drug-refractory disease. To this end, several new brain imaging data, are warranted.
1. Headache Classification Committee of the International 17. Italian Cooperative Study Group on the Epidemiology 33. Cevoli, S. et al. Investigation of the T3111C CLOCK
Headache Society (IHS). The International Classification of Cluster Headache (ICECH). Case-control study on the gene polymorphism in cluster headache. J. Neurol.
of Headache Disorders, 3rd edition. Cephalalgia 38, epidemiology of cluster headache. I: Etiological factors 255, 299–300 (2008).
1–211 (2018). and associated conditions. Neuroepidemiology 14, 34. Rainero, I. et al. Lack of association between the 3092
This is the brand new edition of the International 123–127 (1995). T-->C Clock gene polymorphism and cluster headache.
Classification of Headache Disorders. Next to 18. Sjaastad, O., Shen, J. M., Stovner, L. J. & Elsas, T. Cephalalgia 25, 1078–1081 (2005).
describing >200 headache disorders, it contains Cluster headache in identical twins. Headache 33, 35. Rainero, I. et al. Cluster headache is associated with
up‑to-date references and commentaries on all 214–217 (1993). the alcohol dehydrogenase 4 (ADH4) gene. Headache
headache types, including cluster headache. 19. Leone, M. et al. Increased familial risk of cluster 50, 92–98 (2010).
2. Sandrini, G. et al. Neurophysiological tests and headache. Neurology 56, 1233–1236 (2001). 36. Zarrilli, F. et al. Molecular analysis of cluster headache.
neuroimaging procedures in non-acute headache 20. Russell, M. B., Andersson, P. G. & Thomsen, L. L. Clin. J. Pain 31, 52–57 (2015).
(2nd edition). Eur. J. Neurol. 18, 373–381 (2011). Familial occurrence of cluster headache. J. Neurol. 37. Fourier, C. et al. Screening of two ADH4 variations
3. Sjaastad, O. Cluster Headache Syndrome Neurosurg. Psychiatry 58, 341–343 (1995). in a Swedish cluster headache case-control material.
(W B Saunders Company Ltd, 1992). 21. Russell, M. B., Andersson, P. G., Thomsen, L. L. Headache 56, 835–840 (2016).
4. Russell, M. B. Epidemiology and genetics of cluster & Iselius, L. Cluster headache is an autosomal 38. Bacchelli, E. et al. A genome-wide analysis in cluster
headache. Lancet Neurol. 3, 279–283 (2004). dominantly inherited disorder in some families: headache points to neprilysin and PACAP receptor
5. Lin, K.‑H. et al. Cluster headache in the Taiwanese a complex segregation analysis. J. Med. Genet. 32, gene variants. J. Headache Pain 17, 114 (2016).
— a clinic-based study. Cephalalgia 24, 631–638 954–956 (1995). 39. Ran, C. et al. Screening of genetic variants in
(2004). 22. Baumber, L. et al. A genome-wide scan and HCRTR2 ADCYAP1R1, MME and 14q21 in a Swedish cluster
6. Imai, N. et al. Clinical profile of cluster headaches in candidate gene analysis in a European cluster headache cohort. J. Headache Pain 18, 88 (2017).
Japan: low prevalence of chronic cluster headache, headache cohort. Neurology 66, 1888–1893 (2006). 40. Goadsby, P. J. Pathophysiology of cluster headache:
and uncoupling of sense and behaviour of restlessness. 23. Rainero, I. et al. Association between the G1246A a trigeminal autonomic cephalgia. Lancet Neurol. 1,
Cephalalgia 31, 628–633 (2011). polymorphism of the hypocretin receptor 2 gene and 251–257 (2002).
7. Rozen, T. D. & Fishman, R. S. Cluster headache in cluster headache: a meta-analysis. J. Headache Pain 8, 41. Moskowitz, M. A. Cluster headache: evidence for
the United States of America: demographics, clinical 152–156 (2007). a pathophysiologic focus in the superior pericarotid
characteristics, triggers, suicidality, and personal 24. Bartsch, T., Levy, M. J., Knight, Y. E. & Goadsby, P. J. cavernous sinus plexus. Headache 28, 584–586
burden. Headache 52, 99–113 (2012). Differential modulation of nociceptive dural input to (1988).
8. Manzoni, G. C. Gender ratio of cluster headache over [hypocretin] orexin A and B receptor activation in the 42. Remahl, I. N., Waldenlind, E., Bratt, J. & Ekbom, K.
the years: a possible role of changes in lifestyle. posterior hypothalamic area. Pain 109, 367–378 Cluster headache is not associated with signs of a
Cephalalgia 18, 138–142 (1998). (2004). systemic inflammation. Headache 40, 276–281
9. May, A. Cluster headache: pathogenesis, diagnosis, 25. Weller, C. M. et al. Cluster headache and the (2000).
and management. Lancet 366, 843–855 (2005). hypocretin receptor 2 reconsidered: a genetic 43. Bovim, G., Jenssen, G. & Ericson, K. Orbital
10. Ekbom, K. & Hardebo, J. E. Cluster headache: association study and meta-analysis. Cephalalgia 35, phlebography: a comparison between cluster headache
aetiology, diagnosis and management. Drugs 62, 741–747 (2015). and other headaches. Headache 32, 408–412 (1992).
61–69 (2002). 26. Rainero, I. et al. A polymorphism of the hypocretin 44. Nelson, R. F. et al. Cerebral blood flow studies
11. Taga, A., Russo, M., Manzoni, G. C. & Torelli, P. Cluster receptor 2 gene is associated with cluster headache. in patients with cluster headache. Headache 20,
headache with accompanying migraine-like features: Neurology 63, 1286–1288 (2004). 184–189 (1980).
a possible clinical phenotype. Headache 57, 290–297 27. Schürks, M. et al. Cluster headache is associated 45. Markowitz, S., Saito, K. & Moskowitz, M. A.
(2017). with the G1246A polymorphism in the hypocretin Neurogenically mediated plasma extravasation in dura
12. Ekbom, K., Svensson, D. A., Traff, H. & Waldenlind, E. receptor 2 gene. Neurology 66, 1917–1919 (2006). mater: effect of ergot alkaloids. A possible mechanism
Age at onset and sex ratio in cluster headache: 28. Barloese, M. et al. Sleep and chronobiology in cluster of action in vascular headache. Cephalalgia 8, 83–91
observations over three decades. Cephalalgia 22, headache. Cephalalgia 35, 969–978 (2015). (1988).
94–100 (2002). 29. Cortelli, P. et al. Lack of association between 46. Sakai, F., Meyer, J. S., Ishihara, N., Naritomi, H.
13. Kudrow, L. Cluster Headache: Mechanism mitochondrial tRNALeu(UUR) point mutation and & Deshmukh, V. D. Noninvasive 133XE inhalation
& Management (Oxford Univ. Press, 1980). cluster headache. Lancet 345, 1120–1121 (1995). measurements of regional cerebral blood flow in
14. Manzoni, G. C. et al. Cluster headache — clinical 30. Sjöstrand, C. et al. Analysis of nitric oxide synthase migraine and related headaches. Acta Neurol. Scand.
findings in 180 patients. Cephalalgia 3, 21–30 genes in cluster headache. Cephalalgia 22, 758–764 Suppl. 64, 196–197 (1977).
(1983). (2002). 47. Henry, P. Y., Vernhiet, J., Orgogozo, J. M. & Caille, J. M.
15. Manzoni, G. C., Taga, A., Russo, M. & Torelli, P. 31. Sjöstrand, C., Giedratis, V., Ekbom, K., Waldenlind, E. Cerebral blood flow in migraine and cluster headache.
Age of onset of episodic and chronic cluster headache & Hillert, J. CACNA1A gene polymorphisms in cluster Compartmental analysis and reactivity to anaesthetic
— a review of a large case series from a single headache. Cephalalgia 21, 953–958 (2001). depression. Res. Clin. Studies Headache 6, 81–88
headache centre. J. Headache Pain 17, 44 (2016). 32. Ofte, H. K., Tronvik, E. & Alstadhaug, K. B. Lack (1978).
16. Lee, Y.‑J. et al. Temperature variation and the incidence of association between cluster headache and PER3 48. Norris, J. W., Hachinski, V. C. & Cooper, P. W.
of cluster headache periods: a nationwide population clock gene polymorphism. J. Headache Pain 17, 18 Cerebral blood flow changes in cluster headache.
study. Cephalalgia 34, 656–663 (2014). (2016). Acta Neurol. Scand. 54, 371–374 (1976).
14 | ARTICLE NUMBER 18006 | VOLUME 4 www.nature.com/nrdp
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
PRIMER
49. Krabbe, A.A., Henriksen, L. & Olesen, J. Tomographic activation of trigeminal afferents. Headache 49, 96. Szabó, N. et al. White matter disintegration in cluster
determination of cerebral blood flow during attacks 1131–1143 (2009). headache. J. Headache Pain 14, 64 (2013).
of cluster headache. Cephalalgia 4, 17–23 (1984). This is the best model hitherto that describes 97. Chou, K.‑H. et al. Altered white matter microstructural
50. May, A., Büchel, C., Turner, R. & Goadsby, P. J. how oxygen inhalation may be effective in connectivity in cluster headaches: A longitudinal
Magnetic resonance angiography in facial and other cluster headache. diffusion tensor imaging study. Cephalalgia 34,
pain: neurovascular mechanisms of trigeminal 72. Akerman, S., Holland, P. R., Summ, O., 1040–1052 (2014).
sensation. J. Cereb. Blood Flow Metab. 21, 1171–1176 Lasalandra, M. P. & Goadsby, P. J. A translational in vivo 98. Pringsheim, T. Cluster headache: evidence for a
(2001). model of trigeminal autonomic cephalalgias: therapeutic disorder of circadian rhythm and hypothalamic
51. Weaver-Agostoni, J. Cluster headache. Am. Family characterization. Brain 135, 3664–3675 (2012). function. Can. J. Neurol. Sci. 29, 33–40 (2002).
Physician 88, 122–128 (2013). 73. Robert, C. et al. Paraventricular hypothalamic 99. Strittmatter, M. et al. Altered activity of the
52. Leone, M. et al. The m‑chlorophenylpiperazine test regulation of trigeminovascular mechanisms involved sympathetic nervous system and changes in the
in cluster headache: A study on central serotoninergic in headaches. J. Neurosci. 33, 8827–8840 (2013). balance of hypophyseal, pituitary and adrenal
activity. Cephalalgia 17, 666–672 (1997). 74. May, A. & Goadsby, P. The enigma of the hormones in patients with cluster headache.
53. Goadsby, P. J. & Edvinsson, L. Human in vivo evidence interconnection of trigeminal pain and cranial autonomic Neuroreport 7, 1229–1234 (1996).
for trigeminovascular activation in cluster headache. symptoms. Cephalalgia 36, 727–729 (2015). 100. Leone, M. & Bussone, G. A review of hormonal findings
Neuropeptide changes and effects of acute attacks 75. May, A. & Goadsby, P. J. The trigeminovascular system in cluster headache. Evidence for hypothalamic
therapies. Brain 117, 427–434 (1994). in humans: pathophysiologic implications for primary involvement. Cephalalgia 13, 309–317 (1993).
54. Plosker, G. L. & McTavish, D. Sumatriptan: headache syndromes of the neural influences on the This is one of the first studies pointing towards
a reappraisal of its pharmacology and therapeutic cerebral circulation. J. Cereb. Blood Flow Metab. 19, the hypothalamus as a crucial player in the
efficacy in the acute treatment of migraine and cluster 115–127 (1999). pathophysiology of cluster headache.
headache. Drugs 47, 622–651 (1994). 76. Pietzsch, J. B., Garner, A., Gaul, C. & May, A. Cost- 101. Schulte, L. H. & May, A. Functional neuroimaging
55. Edvinsson, L. & Tfelt-Hansen, P. The blood-brain barrier effectiveness of stimulation of the sphenopalatine in migraine: chances and challenges. Headache 56,
in migraine treatment. Cephalalgia 28, 1245–1258 ganglion (SPG) for the treatment of chronic cluster 1474–1481 (2016).
(2008). headache: a model-based analysis based on the 102. Schulte, L. H. & May, A. The migraine generator
56. Dodick, D. W. & Martin, V. Triptans and CNS side- Pathway CH‑1 study. J. Headache Pain 16, 530 (2015). revisited: continuous scanning of the migraine cycle
effects: pharmacokinetic and metabolic mechanisms. 77. Ansarinia, M. et al. Electrical stimulation of over 30 days and three spontaneous attacks. Brain
Cephalalgia 24, 417–424 (2004). sphenopalatine ganglion for acute treatment of cluster 139, 1987–1993 (2016).
57. Jarrar, R. G., Black, D. F., Dodick, D. W. & Davis, D. H. headaches: Views and perspectives. Headache 50, 103. Malick, A. et al. Trigeminohypothalamic and
Outcome of trigeminal nerve section in the treatment of 1164–1174 (2010). reticulohypothalamic tract neurons in the upper cervical
chronic cluster headache. Neurology 60, 1360–1362 78. Schoenen, J. et al. Stimulation of the sphenopalatine spinal cord and caudal medulla of the rat.
(2003). ganglion (SPG) for cluster headache treatment. Pathway J. Neurophysiol. 84, 2078–2112 (2000).
58. Bartsch, T., Knight, Y. E. & Goadsby, P. J. Activation of CH‑1: a randomized, sham-controlled study. 104. Holland, P. & Goadsby, P. J. The hypothalamic
5‑HT1B/1D receptor in the periaqueductal gray inhibits Cephalalgia: Int. J. Headache 33, 816–830 (2013). orexinergic system: Pain and primary headaches.
nociception. Ann. Neurol. 56, 371–381 (2004). 79. Jürgens, T. P. et al. Long-term effectiveness of Headache 47, 951–962 (2007).
59. Tfelt-Hansen, P. C. Does sumatriptan cross the blood- sphenopalatine ganglion stimulation for cluster 105. Barloese, M. et al. Reduced CSF hypocretin‑1 levels
brain barrier in animals and man? J. Headache Pain headache. Cephalalgia 37, 423–434 (2017). are associated with cluster headache. Cephalalgia 35,
11, 5–12 (2010). Together with Ref. 78, these studies show the 869–876 (2015).
60. Goadsby, P. J. & Lipton, R. B. A review of paroxysmal effectiveness of modulating the parasympathetic 106. May, A. et al. Correlation between structural and
hemicranias, SUNCT syndrome and other short-lasting SPG in patients with cluster headache, which has functional changes in brain in an idiopathic headache
headaches with autonomic feature, including new cases. spurred interest in this structure as part of the syndrome. Nat. Med. 5, 836–838 (1999).
Brain 120, 193–209 (1997). pathophysiology of cluster headache. 107. May, A., Bahra, A., Büchel, C., Frackowiak, R. S. J.
This is a comprehensive review that lays 80. Guo, S. et al. Cranial parasympathetic activation & Goadsby, P. J. Hypothalamic activation in cluster
the foundations of the current concept of induces autonomic symptoms but no cluster headache attacks. Lancet 352, 275–278 (1998).
trigeminal‑autonomic headaches by meticulously headache attacks. Cephalalgia https://doi.org/10.1177/ This is the first imaging study to visualize the
defining a class of headaches based solely on their 0333102417738250 (2017). hypothalamus as an initiator of acute attacks.
clinical features. 81. Möller, M., Haji, A. A., Hoffmann, J. & May, A. 108. Sprenger, T. et al. Specific hypothalamic activation
61. Fanciullacci, M., Alessandri, M., Sicuteri, R. Peripheral provocation of cranial autonomic during a spontaneous cluster headache attack.
& Marabini, S. Responsiveness of the trigeminovascular symptoms is not sufficient to trigger cluster Neurology 62, 516–517 (2004).
system to nitroglycerine in cluster headache patients. headache attacks. Cephalalgia https://doi.org/10.1177/ 109. May, A., Bahra, A., Büchel, C., Frackowiak, R. S. J.
Brain 120, 283–288 (1997). 0333102417738248 (2017). & Goadsby, P. J. PET and MRA findings in cluster
62. Fanciullacci, M., Alessandri, M., Figini, M., Geppetti, P. 82. Goadsby, P. J. Cluster headache and the trigeminal- headache and MRA in experimental pain. Neurology
& Michelacci, S. Increase in plasma calcitonin gene- autonomic reflex: driving or being driven? Cephalalgia 55, 1328–1335 (2000).
related peptide from the extracerebral circulation https://doi.org/10.1177/0333102417738252 110. Arkink, E. B. et al. The anterior hypothalamus in cluster
during nitroglycerin-induced cluster headache attack. (2017). headache. Cephalalgia 37, 1039–1050 (2017).
Pain 60, 119–123 (1995). 83. Derbyshire, S. W. Exploring the pain ‘neuromatrix’. 111. Yang, F.‑C. et al. The pathophysiology of episodic
63. Neeb, L. et al. Corticosteroids alter CGRP and Curr. Rev. Pain 4, 467–477 (2000). cluster headache: Insights from recent neuroimaging
melatonin release in cluster headache episodes. 84. Sandrini, G. et al. Asymmetrical reduction of the research. Cephalalgia https://doi.org/10.1177/
Cephalalgia 35, 317–326 (2015). nociceptive flexion reflex threshold in cluster headache. 0333102417716932 (2017).
64. Neeb, L., Hellen, P., Hoffmann, J., Dirnagl, U. Cephalalgia 20, 647–652 (2000). 112. Lodi, R. et al. Study of hypothalamic metabolism
& Reuter, U. Methylprednisolone blocks interleukin 1 85. Sandrini, G. et al. Impairment of corneal pain in cluster headache by proton MR spectroscopy.
beta induced calcitonin gene related peptide release perception in cluster headache. Pain 47, 299–304 Neurology 66, 1264–1266 (2006).
in trigeminal ganglia cells. J. Headache Pain 17, 19 (1991). 113. Wang, S.‑J., Lirng, J.‑F., Fuh, J.‑L. & Chen, J.‑J.
(2016). 86. Nappi, G. et al. Impaired circadian rhythmicity of Reduction in hypothalamic H‑MRS metabolite ratios
65. Goadsby, P. J., Edvinsson, L. & Ekman, R. Vasoactive nociceptive reflex threshold in cluster headache. in patients with cluster headache. J. Neurol. Neurosurg.
peptide release in the extracerebral circulation of Headache 42, 125–131 (2002). Psychiatry 77, 622–625 (2006).
humans during migraine headache. Ann. Neurol. 28, 87. Ellrich, J., Ristic, D. & Yekta, S. S. Impaired thermal 114. Akram, H. et al. Ventral tegmental area deep brain
183–187 (1990). perception in cluster headache. J. Neurol. 253, stimulation for refractory chronic cluster headache.
66. Goadsby, P. J., Edvinsson, L. & Ekman, R. Release of 1292–1299 (2006). Neurology 86, 1676–1682 (2016).
vasoactive peptides in the extracerebral circulation 88. Perrotta, A. et al. Facilitated temporal processing of 115. Leone, M., Franzini, A., Broggi, G. & Bussone, G.
of humans and the cat during activation of the pain and defective supraspinal control of pain in cluster Hypothalamic stimulation for intractable cluster
trigeminovascular system. Ann. Neurol. 23, 193–196 headache. Pain 154, 1325–1332 (2013). headache: long-term experience. Neurology 67,
(1988). 89. Wang, R. et al. Cognitive processing of cluster headache 150–152 (2006).
67. Tajti, J., Tuka, B., Botz, B., Helyes, Z. & Vecsei, L. Role patients: evidence from event-related potentials. 116. Leone, M., Franzini, A. & Bussone, G. Stereotactic
of pituitary adenylate cyclase-activating polypeptide J. Headache Pain 15, 66 (2014). stimulation of posterior hypothalamic gray matter
in nociception and migraine. CNS Neurol. Disord. Drug 90. Holland, P. R. Modulation of trigeminovascular in a patient with intractable cluster headache. N. Engl.
Targets 14, 540–553 (2015). processing: novel insights into primary headache J. Med. 345, 1428–1429 (2001).
68. Amin, F. M. et al. Investigation of the pathophysiological disorders. Cephalalgia 29 (Suppl. 3), 1–6 (2009). This is the very first report of a successful
mechanisms of migraine attacks induced by pituitary 91. Sprenger, T. et al. Altered metabolism in frontal treatment of cluster headache by hypothalamic
adenylate cyclase-activating polypeptide‑38. Brain brain circuits in cluster headache. Cephalalgia 27, DBS and is also the first study to translate basic
137, 779–794 (2014). 1033–1042 (2007). science, that is, functional imaging results, into a
69. Tuka, B. et al. Release of PACAP‑38 in episodic cluster 92. Sprenger, T. et al. Opioidergic changes in the pineal treatment option.
headache patients — an exploratory study. gland and hypothalamus in cluster headache: A ligand 117. Fontaine, D. et al. Safety and efficacy of deep
J. Headache Pain 17, 69 (2016). PET study. Neurology 66, 1108–1110 (2006). brain stimulation in refractory cluster headache:
70. Sághy, É. et al. Stimulatory effect of pituitary adenylate 93. Yang, F. C. et al. Altered gray matter volume in a randomized placebo-controlled double-blind trial
cyclase-activating polypeptide 6–38, M65 and the frontal pain modulation network in patients followed by a 1‑year open extension. J. Headache Pain
vasoactive intestinal polypeptide 6–28 on trigeminal with cluster headache. Pain 154, 801–807 (2013). 11, 23–31 (2010).
sensory neurons. Neuroscience 308, 144–156 (2015). 94. Absinta, M. et al. Selective decreased grey matter 118. Leone, M., Franzini, A., Proietti Cecchini, A.
71. Akerman, S., Holland, P. R., Lasalandra, M. P. volume of the pain-matrix network in cluster headache. & Bussone, G. Success, failure, and putative
& Goadsby, P. J. Oxygen inhibits neuronal activation Cephalalgia 32, 109–115 (2012). mechanisms in hypothalamic stimulation for drug-
in the trigeminocervical complex after stimulation of 95. Teepker, M. et al. Diffusion tensor imaging in episodic resistant chronic cluster headache. Pain 154, 89–94
trigeminal autonomic reflex, but not during direct dural cluster headache. Headache 52, 274–282 (2012). (2013).
NATURE REVIEWS | DISEASE PRIMERS VOLUME 4 | ARTICLE NUMBER 18006 | 15
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
PRIMER
119. Hodge, C. J., Apkarian, A. V., Stevens, R., Vogelsang, G. 141. De Pue, A., Lutin, B. & Paemeleire, K. Chronic cluster 169. Lademann, V., Jansen, J.‑P., Evers, S. & Frese, A.
& Wisnicki, H. J. Locus coeruleus modulation of dorsal headache and the pituitary gland. J. Headache Pain Evaluation of guideline-adherent treatment in cluster
horn unit responses to cutaneous stimulation. Brain 17, 23 (2016). headache. Cephalalgia 36, 760–764 (2016).
Res. 204, 415–420 (1981). 142. Martins, I. P. Cyclic nocturnal awakening: a warning sign 170. Cohen, A. S., Burns, B. & Goadsby, P. J. High-flow
120. Bussone, G. et al. Brainstem auditory evoked potential of a cluster bout. Cephalalgia 35, 363–365 (2015). oxygen for treatment of cluster headache: a
(BAEPs) in cluster headache (CH): new aspects for a 143. Lai, T.‑H., Fuh, J.‑L. & Wang, S.‑J. Cranial autonomic randomized trial. JAMA 302, 2451–2457 (2009).
central theory. Headache 26, 67–69 (1986). symptoms in migraine: characteristics and comparison This is the first evidence-based study
121. Bussone, G. Cluster headache: from treatment to with cluster headache. J. Neurol. Neurosurg. Psychiatry demonstrating the efficacy of oxygen inhalation in
pathophysiology. Neurol. Sci. 29 (Suppl. 1), S1–S6 80, 1116–1119 (2009). aborting acute cluster headache attacks.
(2008). 144. Bahra, A. & Goadsby, P. J. Diagnostic delays and mis- 171. Petersen, A. S., Barloese, M. C., Lund, N. L.
122. Rocca, M. A. et al. Central nervous system management in cluster headache. Acta Neurol. Scand. & Jensen, R. H. Oxygen therapy for cluster headache.
dysregulation extends beyondthe pain-matrix network 109, 175–179 (2004). A mask comparison trial. A single-blinded, placebo-
in cluster headache. Cephalalgia 30, 1383–1391 145. Joshi, S., Rizzoli, P. & Loder, E. The comorbidity burden controlled, crossover study. Cephalalgia 37, 214–224
(2010). of patients with cluster headache: a population-based (2017).
123. Yang, F.‑C. et al. Altered hypothalamic functional study. J. Headache Pain 18, 76 (2017). 172. Ekbom, K. et al. Subcutaneous sumatriptan in the
connectivity in cluster headache: a longitudinal resting- 146. Jensen, R. M., Lyngberg, A. & Jensen, R. H. Burden acute treatment of cluster headache: a dose
state functional MRI study. J. Neurol. Neurosurg. of cluster headache. Cephalalgia 27, 535–541 (2007). comparison study. The Sumatriptan Cluster
Psychiatry 86, 437–445 (2014). 147. Sánchez Del Rio, M. et al. Errors in recognition and Headache Study Group. Acta Neurol. Scand. 88,
124. Qiu, E., Tian, L., Wang, Y., Ma, L. & Yu, S. Abnormal management are still frequent in patients with cluster 63–69 (1993).
coactivation of the hypothalamus and salience network headache. Eur. Neurol. 72, 209–212 (2014). 173. The Sumatriptan Cluster Headache Study Group.
in patients with cluster headache. Neurology 84, 148. Voiticovschi-Iosob, C. et al. Diagnostic and therapeutic Treatment of acute cluster headache with sumatriptan.
1402–1408 (2015). errors in cluster headache: a hospital-based study. N. Engl. J. Med. 325, 322–326 (1991).
125. Chou, K.‑H. et al. Bout-associated intrinsic functional J. Headache Pain 15, 56 (2014). 174. Leone, M. & Proietti Cecchini, A. Long-term use of
network changes in cluster headache: a longitudinal 149. Rozen, T. D. Cluster headache with aura. Curr. Pain daily sumatriptan injections in severe drug-resistant
resting-state functional MRI study. Cephalalgia 37, Headache Rep. 15, 98–100 (2011). chronic cluster headache. Neurology 86, 194–195
1152–1163 (2016). 150. Ferrari, A. et al. Impact of continuing or quitting (2016).
This study describes dynamic changes in functional smoking on episodic cluster headache: a pilot survey. 175. Rapoport, A. M. et al. Zolmitriptan nasal spray in the
connectivity in specific brain networks between J. Headache Pain 14, 48 (2013). acute treatment of cluster headache: a double-blind
cluster-bout periods, suggesting that these networks 151. Manzoni, G. C. Cluster headache and lifestyle: remarks study. Neurology 69, 821–826 (2007).
play an important part in the seasonal bout-like on a population of 374 male patients. Cephalalgia 19, 176. Cittadini, E. et al. Effectiveness of intranasal
occurrence of episodic cluster headache. 88–94 (1999). zolmitriptan in acute cluster headache: a randomized,
126. Montagna, P., Pierangeli, G. & Cortelli, P. The primary 152. Schurks, M., Kurth, T., Knorn, P., Pageler, L. placebo-controlled, double-blind crossover study.
headaches as a reflection of genetic darwinian adaptive & Diener, H. C. Predictors of hazardous alcohol Arch. Neurol. 63, 1537–1542 (2006).
behavioral responses: views and perspectives. consumption among patients with cluster headache. 177. Schuh-Hofer, S., Reuter, U., Kinze, S., Einhaupl, K. M.
Headache 50, 273–289 (2010). Cephalalgia 26, 623–627 (2006). & Arnold, G. Treatment of acute cluster headache with
127. Torelli, P. & Manzoni, G. Behavior during cluster 153. May, A. Illicit drugs and cluster headache: an inevitable 20 mg sumatriptan nasal spray — an open pilot study.
headache. Curr. Pain Headache Rep. 9, 113–119 discussion. Cephalalgia 32, 1021–1022 (2012). J. Neurol. 249, 94–99 (2002).
(2005). 154. Govare, A. & Leroux, E. Licit and illicit drug use in cluster 178. Van Vliet, J. A. et al. Intranasal sumatriptan in cluster
128. Schmahmann, J. D. & Sherman, J. C. The cerebellar headache. Curr. Pain Headache Rep. 18, 413 (2014). headache: randomized placebo-controlled double-
cognitive affective syndrome. Brain 121, 561–579 155. Rossi, P. et al. Illicit drug use in cluster headache patients blind study. Neurology 60, 630–633 (2003).
(1998). and in the general population: a comparative cross- 179. Bahra, A. et al. Oral zolmitriptan is effective in the
129. Schmahmann, J. D., Weilburg, J. B. & Sherman, J. C. sectional survey. Cephalalgia 32, 1031–1040 (2012). acute treatment of cluster headache. Neurology 54,
The neuropsychiatry of the cerebellum — insights from 156. Di Lorenzo, C. et al. The use of illicit drugs as self- 1832–1839 (2000).
the clinic. Cerebellum 6, 254–267 (2007). medication in the treatment of cluster headache: 180. Andersson, P. G. & Jespersen, L. T. Dihydroergotamine
130. Mehnert, J., Schulte, L., Timmann, D. & May, A. results from an Italian online survey. Cephalalgia 36, nasal spray in the treatment of attacks of cluster
Activity and connectivity of the cerebellum in trigeminal 194–198 (2016). headache. A double-blind trial versus placebo.
nociception. NeuroImage 150, 112–118 (2017). 157. Louter, M. A. et al. Cluster headache and depression. Cephalalgia 6, 51–54 (1986).
131. Morelli, N. et al. Brainstem activation in cluster Neurology 87, 1899–1906 (2016). 181. Magnoux, E. & Zlotnik, G. Outpatient intravenous
headache: an adaptive behavioural response? 158. Liang, J.‑F. et al. Cluster headache is associated dihydroergotamine for refractory cluster headache.
Cephalalgia 33, 416–420 (2013). with an increased risk of depression: a nationwide Headache 44, 249–255 (2004).
132. Lund, N., Barloese, M., Petersen, A., Haddock, B. population-based cohort study. Cephalalgia 33, 182. Nagy, A. J., Gandhi, S., Bhola, R. & Goadsby, P. J.
& Jensen, R. Chronobiology differs between men and 182–189 (2013). Intravenous dihydroergotamine for inpatient
women with cluster headache, clinical phenotype does 159. Levi, R., Edman, G. V., Ekbom, K. & Waldenlind, E. management of refractory primary headaches.
not. Neurology 88, 1069–1076 (2017). Episodic cluster headache. I: Personality and some Neurology 77, 1827–1832 (2011).
This is an important study depicting sex differences neuropsychological characteristics in male patients. 183. Mills, T. M. & Scoggin, J. A. Intranasal lidocaine for
in cluster headache symptoms. Headache 32, 119–125 (1992). migraine and cluster headaches. Ann. Pharmacother.
133. Bahra, A., May, A. & Goadsby, P. J. Cluster headache: 160. Italian Cooperative Study Group on the Epidemiology 31, 914–915 (1997).
a prospective clinical study with diagnostic implications. of Cluster Headache (ICECH). Case-control study 184. Robbins, L. Intranasal lidocaine for cluster headache.
Neurology 58, 354–361 (2002). on the epidemiology of cluster headache. II: Headache 35, 83–84 (1995).
134. Gaul, C. et al. Differences in clinical characteristics and Anthropometric data and personality profile. 185. Costa, A. et al. The effect of intranasal cocaine and
frequency of accompanying migraine features in Funct. Neurol. 15, 215–223 (2000). lidocaine on nitroglycerin-induced attacks in cluster
episodic and chronic cluster headache. Cephalalgia 32, 161. Muñoz, I. et al. Personality traits in patients with cluster headache. Cephalalgia 20, 85–91 (2000).
571–577 (2012). headache: a comparison with migraine patients. 186. Matharu, M. S., Levy, M. J., Meeran, K.
135. Snoer, A., Lund, N., Beske, R., Jensen, R. J. Headache Pain 17, 25 (2016). & Goadsby, P. J. Subcutaneous octreotide in cluster
& Barloese, M. Pre-attack signs and symptoms 162. Piacentini, S. H. M. J., Draghi, L., Cecchini, A. P. headache: randomized placebo-controlled double-
in cluster headache: characteristics and time & Leone, M. Personality disorders in cluster headache: blind crossover study. Ann. Neurol. 56, 488–494
profile. Cephalalgia https://doi.org/10.1177/ a study using the Millon Clinical Multiaxial Inventory-III. (2004).
0333102417726498 (2017). Neurol. Sci. 38, 181–184 (2017). 187. Bussone, G. et al. Double blind comparison of lithium
This study describes frequent symptoms that may 163. Chervin, R. D. et al. Sleep disordered breathing and verapamil in cluster headache prophylaxis.
precede attacks. Identification and recognition of in patients with cluster headache. Neurology 54, Headache 30, 411–417 (1990).
pre-attack symptoms will help delineate cluster 2302–2306 (2000). 188. Leone, M. et al. Verapamil in the prophylaxis of
headache pathophysiology and may enable earlier 164. Barloese, M. C. J., Jennum, P. J., Lund, N. T. episodic cluster headache: a double-blind study versus
abortive treatment. & Jensen, R. H. Sleep in cluster headache — beyond placebo. Neurology 54, 1382–1385 (2000).
136. Jurgens, T. P., Koch, H. J. & May, A. Ten years of a temporal rapid eye movement relationship? 189. Koppen, H. et al. Cardiac monitoring of high-dose
chronic cluster — attacks still cluster. Cephalalgia 30, Eur. J. Neurol. 22, 656–e640 (2015). verapamil in cluster headache: an international Delphi
1123–1126 (2010). 165. Evers, S., Barth, B., Frese, A., Husstedt, I.‑W. study. Cephalalgia 36, 1385–1388 (2016).
137. Evans, R. W. & Schürks, M. Alcohol and cluster & Happe, S. Sleep apnea in patients with cluster 190. Olesen, J., Tfelt-Hansen, P. & Welch, K. The
headaches. Headache 49, 126–129 (2009). headache: a case-control study. Cephalalgia 34, Headaches. (Lippincott Williams & Wilkins, 2006).
138. Headache Classification Committee of the International 828–832 (2014). 191. Ambrosini, A. et al. Suboccipital injection with a
Headache Society (IHS). The International Classification 166. Nilsson Remahl, A. I., Laudon Meyer, E., Cordonnier, C. mixture of rapid- and long-acting steroids in cluster
of Headache Disorders 3rd edn (beta version). & Goadsby, P. J. Placebo response in cluster headache headache: a double-blind placebo-controlled study.
Cephalalgia 33, 629–808 (2013). trials: a review. Cephalalgia 23, 504–510 (2003). Pain 118, 92–96 (2005).
139. [No authors listed.] ICHD / Guidelines. International 167. May, A. et al. EFNS guidelines on the treatment of 192. Leroux, E. et al. Suboccipital steroid injections for
Headache Society http://www.ihs-headache.org/ cluster headache and other trigeminal-autonomic transitional treatment of patients with more than two
ichd-guidelines (2013). cephalalgias. Eur. J. Neurol. 13, 1066–1077 (2006). cluster headache attacks per day: a randomised,
This is the website of the International Headache 168. Robbins, M. S., Starling, A. J., Pringsheim, T. M., double-blind, placebo-controlled trial. Lancet Neurol.
Society with the complete text of the current Becker, W. J. & Schwedt, T. J. Treatment of cluster 10, 891–897 (2011).
classification system in different languages. headache: the American Headache Society evidence- 193. Lambru, G., Shanahan, P., Watkins, L. & Matharu, M. S.
140. Cittadini, E. & Matharu, M. S. Symptomatic trigeminal based guidelines. Headache 56, 1093–1106 (2016). Occipital nerve stimulation in the treatment of
autonomic cephalalgias. Neurologist 15, 305–312 This is a very thorough and evidence-based medically intractable SUNCT and SUNA. Pain Physician
(2009). treatment guideline for cluster headache. 17, 29–41 (2014).
16 | ARTICLE NUMBER 18006 | VOLUME 4 www.nature.com/nrdp
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
PRIMER
194. Ekbom, K. Lithium for cluster headache: review cluster headache: a double-blind placebo-controlled headache (PREVA): a randomised controlled study.
of the literature and preliminary results of long-term cross-over study. Cephalalgia 22, 730–739 (2002). Cephalalgia 36, 534–546 (2015).
treatment. Headache 21, 132–139 (1981). 221. Martelletti, P. et al. Neuromodulation of chronic 244. Torkamani, M. et al. The neuropsychology of cluster
195. Steiner, T. J., Hering, R., Couturier, E. G. M., headaches: position statement from the European headache: cognition, mood, disability, and quality of life
Davies, P. T. G. & Whitmarsh, T. E. Double-blind Headache Federation. J. Headache Pain 14, 86 (2013). of patients with chronic and episodic cluster headache.
placebo-controlled trial of lithium in episodic cluster 222. Jürgens, T. P. et al. Stimulation of the sphenopalatine Headache 55, 287–300 (2015).
headache. Cephalalgia 17, 673–675 (1997). ganglion in intractable cluster headache: Expert 245. D’Amico, D. et al. Health-related quality of life in
196. Gallagher, R. M., Mueller, L. L. & Freitag, F. G. consensus on patient selection and standards of care. patients with cluster headache during active periods.
Divalproex sodium in the treatment of migraine Cephalalgia 34, 1100–1110 (2014). Cephalalgia 22, 818–821 (2002).
and cluster headaches. J. Am. Osteopath Assoc. 102, 223. Barloese, M. C. J. et al. Cluster headache attack 246. Saunders, K., Merikangas, K., Low, N. C. P.,
92–94 (2002). remission with sphenopalatine ganglion stimulation: Von Korff, M. & Kessler, R. C. Impact of comorbidity on
197. Hering, R. & Kuritzky, A. Sodium valproate in the experiences in chronic cluster headache patients headache-related disability. Neurology 70, 538–547
treatment of cluster headache: an open clinical trial. through 24 months. J. Headache Pain 17, 67 (2016). (2008).
Cephalalgia 9, 195–198 (1989). 224. Burns, B., Watkins, L. & Goadsby, P. J. Treatment of 247. Jürgens, T. P. et al. Impairment in episodic and chronic
198. El Amrani, M., Massiou, H. & Bousser, M. G. A negative intractable chronic cluster headache by occipital nerve cluster headache. Cephalalgia 31, 671–682 (2011).
trial of sodium valproate in cluster headache: stimulation in 14 patients. Neurology 72, 341–345 248. Abu Bakar, N. et al. The development and validation
methodological issues. Cephalalgia 22, 205–208 (2009). of the Cluster Headache Quality of life scale (CHQ).
(2002). 225. Fontaine, D. et al. Treatment of refractory chronic J. Headache Pain 17, 79 (2016).
199. Forderreuther, S., Mayer, M. & Straube, A. Treatment cluster headache by chronic occipital nerve stimulation. 249. Donnet, A. et al. Chronic cluster headache: a French
of cluster headache with topiramate: effects and Cephalalgia 31, 1101–1105 (2011). clinical descriptive study. J. Neurol. Neurosurg.
side‑effects in five patients. Cephalalgia 22, 186–189 226. Fontaine, D. et al. Occipital nerve stimulation improves Psychiatr. 78, 1354–1358 (2007).
(2002). the quality of life in medically-intractable chronic cluster 250. Palacios-Ceña, D. et al. Living with cluster headache:
200. Huang, W. Y., Lo, M. C., Wang, S. J., Tsai, J. J. & headache: results of an observational prospective a qualitative study of patients’ perspectives. Headache
Wu, H. M. Topiramate in prevention of cluster headache study. Cephalalgia 37, 1173–1179 (2017). 56, 1171–1182 (2016).
in the Taiwanese. Neurol. India 58, 284–287 (2010). 227. Miller, S., Watkins, L. & Matharu, M. Treatment of 251. Luerding, R. et al. Aggressiveness in different
201. Schuh-Hofer, S., Israel, H., Neeb, L., Reuter, U. intractable chronic cluster headache by occipital nerve presentations of cluster headache: results from
& Arnold, G. The use of gabapentin in chronic cluster stimulation: a cohort of 51 patients. Eur. J. Neurol. 24, a controlled multicentric study. Cephalalgia 32,
headache patients refractory to first-line therapy. 381–390 (2017). 528–536 (2012).
Eur. J. Neurol. 14, 694–696 (2007). 228. Leone, M., Proietti Cecchini, A., Messina, G. 252. Romero-Reyes, M., Pardi, V. & Akerman, S. A potent
202. Vukovic, V., Lovrencic-Huzjan, A., Budisic, M. & Franzini, A. Long-term occipital nerve stimulation for and selective calcitonin gene-related peptide (CGRP)
& Demarin, V. Gabapentin in the prophylaxis of cluster drug-resistant chronic cluster headache. Cephalalgia receptor antagonist, MK‑8825, inhibits responses
headache: an observational open label study. Acta Clin. 37, 756–763 (2017). to nociceptive trigeminal activation: Role of CGRP
Croat. 48, 311–314 (2009). 229. Schoenen, J., Roberta, B., Magis, D. & Coppola, G. in orofacial pain. Exp. Neurol. 271, 95–103 (2015).
203. Monstad, I. et al. Preemptive oral treatment with Noninvasive neurostimulation methods for migraine 253. Crowley, B. M. et al. Novel oxazolidinone calcitonin
sumatriptan during a cluster period. Headache 35, therapy: the available evidence. Cephalalgia 36, gene-related peptide (CGRP) receptor antagonists for
607–613 (1995). 1170–1180 (2016). the acute treatment of migraine. Bioorg. Med. Chem.
204. Zebenholzer, K., Wober, C., Vigl, M. & Wessely, P. 230. Magis, D. & Schoenen, J. Advances and challenges Lett. 25, 4777–4781 (2015).
Eletriptan for the short-term prophylaxis of cluster in neurostimulation for headaches. Lancet Neurol. 11, 254. Ho, T. W. et al. Randomized controlled trial of the CGRP
headache. Headache 44, 361–364 (2004). 708–719 (2012). receptor antagonist telcagepant for migraine
205. Mulder, L. J. & Spierings, E. L. Naratriptan in the This is an excellent review on the indications prevention. Neurology 83, 958–966 (2014).
preventive treatment of cluster headache. Cephalalgia for and efficacy of all current neuromodulation 255. Bigal, M. E. et al. Safety, tolerability, and efficacy of
22, 815–817 (2002). techniques in headache. TEV‑48125 for preventive treatment of high-frequency
206. Sicuteri, F. et al. Beneficial effect of capsaicin 231. Magis, D., Gérard, P. & Schoenen, J. Invasive occipital episodic migraine: A multicentre, randomised, double-
application to the nasal mucosa in cluster headache. nerve stimulation for refractory chronic cluster blind, placebo-controlled, phase 2b study. Lancet
Clin. J. Pain 5, 49–53 (1989). headache: what evolution at long-term? Strengths Neurol. 14, 1081–1090 (2015).
207. Fusco, B. M., Marabini, S., Maggi, C. A., Fiore, G. and weaknesses of the method. J. Headache Pain 17, 256. Sun, H. et al. Safety and efficacy of AMG 334 for
& Geppetti, P. Preventative effect of repeated nasal 8 (2016). prevention of episodic migraine: a randomised, double-
applications of capsaicin in cluster headache. Pain 59, 232. Magis, D. et al. Central modulation in cluster headache blind, placebo-controlled, phase 2 trial. Lancet Neurol.
321–325 (1994). patients treated with occipital nerve stimulation: 15, 382–390 (2016).
208. Marks, D. R. et al. A double-blind placebo-controlled an FDG-PET study. BMC Neurol. 11, 25 (2011). 257. Goadsby, P. J. & Bartsch, T. On the functional
trial of intranasal capsaicin for cluster headache. 233. Wilbrink, L. A. et al. Occipital nerve stimulation in neuroanatomy of neck pain. Cephalalgia 28 (Suppl. 1),
Cephalalgia 13, 114–116 (1993). medically intractable, chronic cluster headache. The 1–7 (2008).
209. Saper, J. R. et al. Intranasal civamide for the treatment ICON study: rationale and protocol of a randomised 258. Lambru, G. & Matharu, M. S. Peripheral
of episodic cluster headaches. Arch. Neurol. 59, trial. Cephalalgia 33, 1238–1247 (2013). neurostimulation in primary headaches. Neurol. Sci.
990–994 (2002). 234. Leone, M. Deep brain stimulation in headache. Lancet 35 (Suppl. 1), 77–81 (2014).
210. Leone, M., D’Amico, D., Moschiano, F., Fraschini, F. Neurol. 5, 873–877 (2006). 259. Schuster, N. M. & Rapoport, A. M. New strategies for
& Bussone, G. Melatonin versus placebo in the 235. Schoenen, J. et al. Hypothalamic stimulation in chronic the treatment and prevention of primary headache
prophylaxis of cluster headache: a double-blind pilot cluster headache: a pilot study of efficacy and mode of disorders. Nat. Rev. Neurol. 12, 635–650 (2016).
study with parallel groups. Cephalalgia 16, 494–496 action. Brain 128, 940–947 (2005).
(1996). 236. Matharu, M. S. & Zrinzo, L. Deep brain stimulation Author contributions
211. Pringsheim, T., Magnoux, E., Dobson, C. F., Hamel, E. in cluster headache: hypothalamus or midbrain Introduction (A.M.); Epidemiology (P.P.‑R. and D.M.);
& Aube, M. Melatonin as adjunctive therapy in the tegmentum? Curr. Pain Headache Rep. 14, 151–159 Mechanisms/pathophysiology (A.M. and S.‑J.W.); Diagnosis,
prophylaxis of cluster headache: a pilot study. (2010). screening and prevention (T.J.S.); Management (S.E. and
Headache 42, 787–792 (2002). 237. Clelland, C. D., Zheng, Z., Kim, W., Bari, A. D.M.); Quality of life (P.P.‑R.); Outlook (S.‑J.W. and A.M.);
212. Kowacs, P. A. et al. Warfarin as a therapeutic option & Pouratian, N. Common cerebral networks associated Overview of the Primer (all authors).
in the control of chronic cluster headache: a report of with distinct deep brain stimulation targets for cluster
three cases. J. Headache Pain 6, 417–419 (2005). headache. Cephalalgia 34, 224–230 (2014). Competing interests
213. Hakim, S. M. Warfarin for refractory chronic cluster 238. Fontaine, D. et al. Anatomical location of effective deep A.M. has been a consultant or speaker for Allergan, Autonomic
headache: a randomized pilot study. Headache 51, brain stimulation electrodes in chronic cluster Technologies, Desitin, Electrocore and Teva and is the Editor in
713–725 (2011). headache. Brain 133, 1214–1223 (2010). Chief for Cephalalgia. T.J.S. has acted as a consultant or has
214. Hering-Hanit, R. & Gadoth, N. Baclofen in cluster 239. Seijo, F. et al. Neuromodulation of the posterolateral served on the advisory boards of Allergan, Amgen, Autonomic
headache. Headache 40, 48–51 (2000). hypothalamus for the treatment of chronic refractory Technologies, Avanir, Dr. Reddy’s, Nocira, Novartis and Teva;
215. Leone, M. et al. Transdermal clonidine in the cluster headache: experience in five patients with has stock options in Nocira and Second Opinion; and has
prophylaxis of episodic cluster headache: an open a modified anatomical target. Cephalalgia 31, received royalties from UpToDate. D.M. has received research
study. Headache 37, 559–560 (1997). 1634–1641 (2011). and travel grants from ElectroCore LLC. P.P.‑R. has received
216. Tronvik, E. et al. Randomised trial on episodic cluster 240. Chabardès, S. et al. Endoventricular deep brain honoraria as a consultant or speaker from Allergan, Almirall,
headache with an angiotensin II receptor blocker. stimulation of the third ventricle: proof of concept and Chiesi, Eli Lilly, Novartis and Teva. S.E. has received honoraria
Cephalalgia 33, 1026–1034 (2013). application to cluster headache. Neurosurgery 79, as a speaker from or is a member of an advisory board for
217. Evers, S. Botulinum toxin and the management of 806–815 (2016). Allergan, Johnson & Johnson, Novartis, Reckitt Benckiser and
chronic headaches. Curr. Opin. Otolaryngol. Head Neck 241. Silberstein, S. D. et al. Non-invasive vagus nerve TAD Pharma. S.-J.W. has served on the advisory boards of
Surg. 12, 197–203 (2004). stimulation for the acute treatment of cluster headache: Daiichi-Sankyo, Eli Lilly and Taiwan Pfizer and has received
218. Sostak, P., Krause, P., Förderreuther, S., Reinisch, V. findings from the randomized, double-blind, sham- honoraria as a moderator from the Taiwan branches of Bayer,
& Straube, A. Botulinum toxin type‑A therapy in controlled ACT1 study. Headache 56, 1317–1332 Eisai, Eli Lilly and Pfizer.
cluster headache: an open study. J. Headache Pain 8, (2016).
236–241 (2007). 242. Goadsby, P. J. et al. Non-invasive vagus nerve Publisher’s note
219. Bratbak, D. F. et al. Pilot study of sphenopalatine stimulation for the acute treatment of episodic and Springer Nature remains neutral with regard to jurisdictional
injection of onabotulinumtoxinA for the treatment of chronic cluster headache: a randomized, double-blind, claims in published maps and institutional affiliations.
intractable chronic cluster headache. Cephalalgia 36, sham-controlled ACT2 study. Cephalalgia https://
503–509 (2016). doi.org/10.1177/0333102417744362 (2017). How to cite this article
220. Nilsson Remahl, A. I., Ansjon, R., Lind, F. 243. Gaul, C. et al. Non-invasive vagus nerve stimulation May, A. et al. Cluster headache. Nat. Rev. Dis. Primers 4,
& Waldenlind, E. Hyperbaric oxygen treatment of active for PREVention and Acute treatment of chronic cluster 18006 (2018).
NATURE REVIEWS | DISEASE PRIMERS VOLUME 4 | ARTICLE NUMBER 18006 | 17
©
2
0
1
8
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (843)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Better Than Alchemy WebDocument6 pagesBetter Than Alchemy WebSameerNo ratings yet
- Botany (Flower)Document15 pagesBotany (Flower)Louis Fetilo FabunanNo ratings yet
- 2C X 95CU POWER - Revised Datasheet Solar CableDocument1 page2C X 95CU POWER - Revised Datasheet Solar CableAashish MoyalNo ratings yet
- A Study On Customer Perception Towards Sri Vinayaka Automobiles Private LimitedDocument13 pagesA Study On Customer Perception Towards Sri Vinayaka Automobiles Private LimitedGmcrNo ratings yet
- The Five Stages of Team Development A Case StudyDocument7 pagesThe Five Stages of Team Development A Case StudyLili100% (2)
- Cpanel 11.25 - Cheat SheetDocument1 pageCpanel 11.25 - Cheat SheetIanNo ratings yet
- Comparative Homeland Security Global Lessons Wiley Series On Homeland Defense and Security Ebook PDF VersionDocument62 pagesComparative Homeland Security Global Lessons Wiley Series On Homeland Defense and Security Ebook PDF Versionjohn.le742100% (47)
- CBRN Protective Ensemble StandardDocument137 pagesCBRN Protective Ensemble Standarddhoo_babyNo ratings yet
- Historical Commentary On HBO's Chernobyl - Annotated Episode 5 ScriptDocument92 pagesHistorical Commentary On HBO's Chernobyl - Annotated Episode 5 ScriptMichael Long100% (1)
- Income Distribution and Poverty in The PhilippinesDocument14 pagesIncome Distribution and Poverty in The PhilippinesEd Leen Ü100% (6)
- What Is A Fruit: Suggestion: Access 'Vegetables" Select 'Tomato' Click 'Go'Document5 pagesWhat Is A Fruit: Suggestion: Access 'Vegetables" Select 'Tomato' Click 'Go'Al-juffrey Luis AmilhamjaNo ratings yet
- BGP Routing Protocol: BY: Gebretinsae GDocument87 pagesBGP Routing Protocol: BY: Gebretinsae GDereje SeyoumNo ratings yet
- Ilovepdf Merged MergedDocument431 pagesIlovepdf Merged MergedShreyash VermaNo ratings yet
- Legal Studies 10 20 Course OutlineDocument2 pagesLegal Studies 10 20 Course Outlineapi-124179415No ratings yet
- 8 Leadership Lessons From Nelson MandelaDocument2 pages8 Leadership Lessons From Nelson MandelaEli MoreiraNo ratings yet
- FER5100 Technical DatasheetDocument1 pageFER5100 Technical DatasheetblackboxdesignNo ratings yet
- Chapter 34 Exploration and Evaluation of Mineral ResourcesDocument2 pagesChapter 34 Exploration and Evaluation of Mineral ResourcesEllen MaskariñoNo ratings yet
- Chandan Itr 2form Downloaded 20-21Document33 pagesChandan Itr 2form Downloaded 20-21Ameet ChandanNo ratings yet
- American Marketing Association Social Media ToolkitDocument159 pagesAmerican Marketing Association Social Media ToolkitDana VanDen Heuvel100% (3)
- Affiliated To Senate of SeramporeDocument6 pagesAffiliated To Senate of SeramporeJaison Kaduvakuzhiyil VargheseNo ratings yet
- Apostolic AgeDocument6 pagesApostolic AgeMINCOR SS CC100% (1)
- Bahay KuboDocument4 pagesBahay KuboJerome Amor AclanNo ratings yet
- Patent Search WorkshopDocument4 pagesPatent Search WorkshopBindu SharmaNo ratings yet
- I Ching Foreword by Carl Gustav JungDocument16 pagesI Ching Foreword by Carl Gustav JungTuiVuelaNo ratings yet
- Ceramic Braces 809Document2 pagesCeramic Braces 809api-235269401No ratings yet
- Semester Viii: Total Quality ManagementDocument4 pagesSemester Viii: Total Quality ManagementNano GowthamNo ratings yet
- Class 6TH ScienceDocument73 pagesClass 6TH SciencerahulNo ratings yet
- India'S Standing in Pharma Industry: MBA (IB) 19-21 India & WtoDocument5 pagesIndia'S Standing in Pharma Industry: MBA (IB) 19-21 India & WtoAman AgarwalNo ratings yet
- Teknik Relaksasi Genggam Jari Terhadap Intensitas Nyeri Pada Pasien Post AppendiktomiDocument5 pagesTeknik Relaksasi Genggam Jari Terhadap Intensitas Nyeri Pada Pasien Post Appendiktomirahmawati ningsihNo ratings yet
- Mason C-RE HDB Test Report - Tensile 2016Document5 pagesMason C-RE HDB Test Report - Tensile 2016Eric Ng S LNo ratings yet