You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Biomedicines 10 03156Document19 pagesBiomedicines 10 03156Thành Nguyễn VănNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- To Compare The Total Cholesterol and HDL-cholesterol Before and After Ultra-Centrifugation in Lipemic SamplesDocument5 pagesTo Compare The Total Cholesterol and HDL-cholesterol Before and After Ultra-Centrifugation in Lipemic SamplesThành Nguyễn VănNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Standard Precautions: A Key Element of Infection Control Under Critical AppraisalDocument38 pagesStandard Precautions: A Key Element of Infection Control Under Critical AppraisalThành Nguyễn VănNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Revista de Senología y Patología MamariaDocument5 pagesRevista de Senología y Patología MamariaThành Nguyễn VănNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Outdoor Airborne Transmission of Coronavirus Among Apartments in High-Density CitiesDocument19 pagesOutdoor Airborne Transmission of Coronavirus Among Apartments in High-Density CitiesThành Nguyễn VănNo ratings yet
- Increased Erythrocytic Osmotic Fragility in Anemic Domestic Shorthair and Purebred CatsDocument20 pagesIncreased Erythrocytic Osmotic Fragility in Anemic Domestic Shorthair and Purebred CatsThành Nguyễn VănNo ratings yet
- HHS Public AccessDocument15 pagesHHS Public AccessThành Nguyễn VănNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Delick Pitch Deck by SlidesgoDocument52 pagesDelick Pitch Deck by SlidesgoThành Nguyễn VănNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Fashion Pitch Deck by SlidesgoDocument50 pagesFashion Pitch Deck by SlidesgoThành Nguyễn VănNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- NESTROFTpaperDocument5 pagesNESTROFTpaperThành Nguyễn VănNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Nutrition and HealthDocument7 pagesNutrition and HealthThành Nguyễn VănNo ratings yet
- Library Center by SlidesgoDocument42 pagesLibrary Center by SlidesgoThành Nguyễn VănNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Library Center by SlidesgoDocument42 pagesLibrary Center by SlidesgoThành Nguyễn VănNo ratings yet
- Fulltext - Hematology v3 Id1118Document3 pagesFulltext - Hematology v3 Id1118Thành Nguyễn VănNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Organic Compounds of S, Se, TeDocument84 pagesOrganic Compounds of S, Se, TeNickly Nick100% (1)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Aldehydes and KetonesDocument4 pagesAldehydes and KetonesAnonymous GO6JVW9Wud50% (2)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- G10-Science 4TH Finals-TqDocument4 pagesG10-Science 4TH Finals-TqYvette Marie Yaneza NicolasNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Penawaran CiputraDocument3 pagesPenawaran CiputrahandryhuaNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- PRICELIST JANUARI 2022 (AutoRecovered)Document26 pagesPRICELIST JANUARI 2022 (AutoRecovered)taufanmjNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- CI SSCK1623 Organic Chemistry For Engineering 20192020-2 PDFDocument5 pagesCI SSCK1623 Organic Chemistry For Engineering 20192020-2 PDFKavinesh GanesanNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Degarelix (SQ) : Flutamide, BicalutamideDocument5 pagesDegarelix (SQ) : Flutamide, BicalutamideGregNo ratings yet
- Studi Kualitatif Dan Kuantitatif Fitokimia Ekstrak Air Dan Ekstrak Etanol Daun Kirinyuh (Chromolaena Odorata L.) Yang Tumbuh Di Provinsi BaliDocument5 pagesStudi Kualitatif Dan Kuantitatif Fitokimia Ekstrak Air Dan Ekstrak Etanol Daun Kirinyuh (Chromolaena Odorata L.) Yang Tumbuh Di Provinsi BaliOkta OliviaNo ratings yet
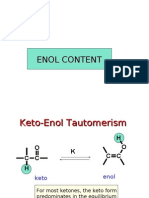
- Enol ContentDocument13 pagesEnol Contentsally gomaa100% (2)
- Nucleic Acids and Protein Synthesis RevisedDocument60 pagesNucleic Acids and Protein Synthesis Revisedemanuel coatesNo ratings yet
- Density Values of Several PlasticsDocument4 pagesDensity Values of Several PlasticsAbdullah Al AsikNo ratings yet
- Integración Metabólica y Vías UnidireccionalesDocument31 pagesIntegración Metabólica y Vías UnidireccionalesFabiola AmigoNo ratings yet
- Biochem Lab Activity 5Document47 pagesBiochem Lab Activity 5Nafeesa Cadir100% (1)
- Key Hormones Brain Metabceu2018Document8 pagesKey Hormones Brain Metabceu2018Kim RamosNo ratings yet
- KarbohidratDocument44 pagesKarbohidratJiyuuNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- MCQ - Halo Alkanes& Haloarenes: Velammal Vidyalaya-Viraganoor Sub-Xii ChemistryDocument12 pagesMCQ - Halo Alkanes& Haloarenes: Velammal Vidyalaya-Viraganoor Sub-Xii ChemistryKrishna Moorthy RamaiahNo ratings yet
- Desmet Purifine1Document3 pagesDesmet Purifine1ricm152No ratings yet
- Parasympathomimetics and ParasympatholyticsDocument16 pagesParasympathomimetics and ParasympatholyticsSalona Roy100% (4)
- Biochemistry SamplexDocument12 pagesBiochemistry SamplexJo Anne75% (4)
- Chapter 21Document52 pagesChapter 21aggelisgeorge8546No ratings yet
- 1 of 33 © Boardworks LTD 2009Document33 pages1 of 33 © Boardworks LTD 2009gabbbbbbbbbbbbbbbbNo ratings yet
- Table of PKa and PI ValuesDocument12 pagesTable of PKa and PI ValuesMariel Defensor ContiNo ratings yet
- Antioxidants For Fuel ApplicationsDocument35 pagesAntioxidants For Fuel ApplicationsVictor Castrejon100% (1)
- III) GOC-Some Basic Principles & Techniques: 1. Priority Order F.G. Multiple Bond SubstituentDocument15 pagesIII) GOC-Some Basic Principles & Techniques: 1. Priority Order F.G. Multiple Bond SubstituentSHIVAMNo ratings yet
- Harga Pihak 3Document16 pagesHarga Pihak 3Aprillian AptNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Common Name 11thDocument16 pagesCommon Name 11thCheryl ChaudhariNo ratings yet
- Organic Chemistry - WikipediaDocument11 pagesOrganic Chemistry - Wikipediatsvmpm1765No ratings yet
- List of Quality Control Orders Notified in Gazette of India To Make The Standards Mandatory - Ministry of Chemicals and FertilizersDocument14 pagesList of Quality Control Orders Notified in Gazette of India To Make The Standards Mandatory - Ministry of Chemicals and FertilizersELP LawNo ratings yet
- Biochemistry I BSC 211: LipidsDocument16 pagesBiochemistry I BSC 211: LipidsKelvin ChipezeniNo ratings yet
- Myers Chem 115: ReductionDocument18 pagesMyers Chem 115: ReductionviejayNo ratings yet
- ICH Quality Guidelines: An Implementation GuideFrom EverandICH Quality Guidelines: An Implementation GuideAndrew TeasdaleNo ratings yet