You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Permaculture - Plants Suitable For Ground Cover (P) - Plants For A FutureDocument2 pagesPermaculture - Plants Suitable For Ground Cover (P) - Plants For A Futurecontadino_impazzitoNo ratings yet
- History TakingDocument51 pagesHistory TakingJAMES TONNY OKINYINo ratings yet
- Mary Szybist On Visual Poetry Compressed PDFDocument5 pagesMary Szybist On Visual Poetry Compressed PDFcarlos.enrique.fonseca1440No ratings yet
- FCE Reading and Use of English - Practice Test 14Document13 pagesFCE Reading and Use of English - Practice Test 14Andrea LNo ratings yet
- 1926 PapionianDocument108 pages1926 PapionianPLCS_FoundationNo ratings yet
- Grade 7-Advanced Science Environmental ScienceDocument8 pagesGrade 7-Advanced Science Environmental ScienceChrisel Luat LopezNo ratings yet
- Datasheet - 74LS283 - Somador Binário Completo de 4 BitsDocument7 pagesDatasheet - 74LS283 - Somador Binário Completo de 4 BitsLucas CarvalhoNo ratings yet
- Sarmatian Swords 2 - ROMECDocument12 pagesSarmatian Swords 2 - ROMECkulcsarv100% (2)
- Understanding Blow Molding: Norman C. LeeDocument11 pagesUnderstanding Blow Molding: Norman C. LeeKiran ModakNo ratings yet
- Efek Ramadan Dan DispepsiaDocument8 pagesEfek Ramadan Dan DispepsiayafanitaizzatiNo ratings yet
- Reference Ranges For Serum Insulin-Like Growth Factor I (IGF-I) in Healthy Chinese AdultsDocument15 pagesReference Ranges For Serum Insulin-Like Growth Factor I (IGF-I) in Healthy Chinese AdultsyafanitaizzatiNo ratings yet
- 997-Article Text-4321-1-10-20220730Document7 pages997-Article Text-4321-1-10-20220730yafanitaizzatiNo ratings yet
- Reliability of Mini Nutritional Assessment in Hemodialysis Compared With Subjective Global AssessmentDocument6 pagesReliability of Mini Nutritional Assessment in Hemodialysis Compared With Subjective Global AssessmentyafanitaizzatiNo ratings yet
- The Predictive Value of Malnutrition For Functional and Cognitive Status in Elderly Hemodialysis PatientsDocument8 pagesThe Predictive Value of Malnutrition For Functional and Cognitive Status in Elderly Hemodialysis PatientsyafanitaizzatiNo ratings yet
- Giglio 2018Document11 pagesGiglio 2018yafanitaizzatiNo ratings yet
- Prevalence of Sarcopenia and Its Association WithDocument9 pagesPrevalence of Sarcopenia and Its Association WithyafanitaizzatiNo ratings yet
- Abstracts Clinical Nutrition ESPEN 40 (2020) 412 E690Document2 pagesAbstracts Clinical Nutrition ESPEN 40 (2020) 412 E690yafanitaizzatiNo ratings yet
- Modified Mininutritional Assessment Can Effectively Assess The Nutritional Status of Patients On HemodialysisDocument9 pagesModified Mininutritional Assessment Can Effectively Assess The Nutritional Status of Patients On HemodialysisyafanitaizzatiNo ratings yet
- Kairo AllDocument6 pagesKairo AllyafanitaizzatiNo ratings yet
- Unit 2 SignalsDocument3 pagesUnit 2 SignalsDigitallogicdlNo ratings yet
- 8000series Tech Datasheet 2018Document3 pages8000series Tech Datasheet 2018lucky414No ratings yet
- Amotec 12864Q DisplayDocument17 pagesAmotec 12864Q DisplayEdgarNo ratings yet
- Keeling 1960 PDFDocument4 pagesKeeling 1960 PDFErick AmâncioNo ratings yet
- SEC - Connection Guidelines - v3 - CleanDocument54 pagesSEC - Connection Guidelines - v3 - CleanFurqan HamidNo ratings yet
- Rundown ICTSD 2018 - (Latest)Document9 pagesRundown ICTSD 2018 - (Latest)Annisa Farida HayuningsihNo ratings yet
- Camera CalibrationDocument11 pagesCamera CalibrationFabien MairesseNo ratings yet
- Bubble Growth in A Two-Dimensional Viscoelastic Foam: S.L. Everitt, O.G. Harlen, H.J. WilsonDocument14 pagesBubble Growth in A Two-Dimensional Viscoelastic Foam: S.L. Everitt, O.G. Harlen, H.J. Wilsonliviagoncalves197271No ratings yet
- Dr. M. Syed Jamil Asghar: Paper Published: 80Document6 pagesDr. M. Syed Jamil Asghar: Paper Published: 80Awaiz NoorNo ratings yet
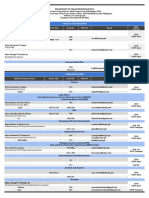
- Updated DOTr Directory As of 29 October 2021Document9 pagesUpdated DOTr Directory As of 29 October 2021Twinkle MiguelNo ratings yet
- BB204-Toddler Bed Assembly InstructionsDocument10 pagesBB204-Toddler Bed Assembly InstructionsCaloi PastorfideNo ratings yet
- Material Balance & Energy Balance - Reactor-2Document32 pagesMaterial Balance & Energy Balance - Reactor-2Xy karNo ratings yet
- BotanyDocument11 pagesBotanyGirish GuptaNo ratings yet
- BCB NO1) Bearing CatalogDocument17 pagesBCB NO1) Bearing CatalogGabriela TorresNo ratings yet
- AnorexiaDocument1 pageAnorexiaCHIEF DOCTOR MUTHUNo ratings yet
- 1 Stack Testing Source Policy - RA 8749 Legal Oct 2019 Updates - Engr. Jundy Del SocorroDocument80 pages1 Stack Testing Source Policy - RA 8749 Legal Oct 2019 Updates - Engr. Jundy Del SocorroJayson ResultayNo ratings yet
- Tuf Pneumatic Long Nose Hog Ring Gun Sc77xeDocument5 pagesTuf Pneumatic Long Nose Hog Ring Gun Sc77xearturoNo ratings yet
- Unit P1, P1.1: The Transfer of Energy by Heating ProcessesDocument9 pagesUnit P1, P1.1: The Transfer of Energy by Heating ProcessesTemilola OwolabiNo ratings yet
- GFRC Floating Concrete Hearth For Concrete Wood FiDocument11 pagesGFRC Floating Concrete Hearth For Concrete Wood FiJuliano. PQMNo ratings yet
- Cyclic VoltammetryDocument4 pagesCyclic Voltammetryreddynivas100% (1)
- Lighting Movements-The Fox On The FairwayDocument1 pageLighting Movements-The Fox On The FairwayabneypaigeNo ratings yet