You might also like
- sergii,+Journal+editor,+03Hamed Articulo 2Document8 pagessergii,+Journal+editor,+03Hamed Articulo 2anye daniela gilNo ratings yet
- Mirror Therapy Feedback For Selective Motor Control of The Upper Extremities in Spastic Hemiplegic Cerebral Palsy: A Randomized Controlled TrialDocument4 pagesMirror Therapy Feedback For Selective Motor Control of The Upper Extremities in Spastic Hemiplegic Cerebral Palsy: A Randomized Controlled TrialPaula Tirado GuallarNo ratings yet
- Papn MS Id 000156Document7 pagesPapn MS Id 000156niekoNo ratings yet
- (129 136) V9N5PTDocument8 pages(129 136) V9N5PTAqila NurNo ratings yet
- Exercise Training Program in Children and Adolescents With Cerebral PalsyDocument7 pagesExercise Training Program in Children and Adolescents With Cerebral PalsyValentina SiegmundNo ratings yet
- Children 09 01470Document10 pagesChildren 09 01470Christhoper HermosillaNo ratings yet
- Pedia TriDocument6 pagesPedia TriRIZHAN ATHAYANo ratings yet
- Journal Presentation by 18PT3015 PEDDocument20 pagesJournal Presentation by 18PT3015 PEDAbdul KhadeerNo ratings yet
- Gait & Posture: Yoyo T.Y. Cheng, William W.N. Tsang, Catherine Mary Schooling, Shirley S.M. FongDocument7 pagesGait & Posture: Yoyo T.Y. Cheng, William W.N. Tsang, Catherine Mary Schooling, Shirley S.M. FongDiego CampillayNo ratings yet
- Effects of Modified Adeli Suit Therapy On Improvement of Gross Motor Function in Children With Cerebral Palsy (2011)Document6 pagesEffects of Modified Adeli Suit Therapy On Improvement of Gross Motor Function in Children With Cerebral Palsy (2011)caterina1990No ratings yet
- A Study To Find Out The Effect of Arm Movement Through Sensory Based Game On Improving Postural Control in Spastic Diplegic Cerebral PalsyDocument6 pagesA Study To Find Out The Effect of Arm Movement Through Sensory Based Game On Improving Postural Control in Spastic Diplegic Cerebral PalsyEditor IJTSRDNo ratings yet
- 51 55Document5 pages51 55SuniNo ratings yet
- Original Article: Effects of Neurodevelopmental Therapy On Gross Motor Function in Children With Cerebral PalsyDocument6 pagesOriginal Article: Effects of Neurodevelopmental Therapy On Gross Motor Function in Children With Cerebral PalsyIkhwatul FitriNo ratings yet
- (31 36) V9N5PTDocument6 pages(31 36) V9N5PTASD2019No ratings yet
- Medicina: Ffect of A Combined Stretching and StrengthDocument12 pagesMedicina: Ffect of A Combined Stretching and StrengthKimum KimúmNo ratings yet
- Exercise Interventions Improve Postural Control in Children With Cerebral Palsy: A Systematic ReviewDocument17 pagesExercise Interventions Improve Postural Control in Children With Cerebral Palsy: A Systematic ReviewEmad Eldin Mohamed AbdelatiefNo ratings yet
- Effectiveness of Proprioceptive Training Over Strength Training in Improving The Balance of Cerebral Palsy Children With Impaired BalanceDocument14 pagesEffectiveness of Proprioceptive Training Over Strength Training in Improving The Balance of Cerebral Palsy Children With Impaired BalanceDr. Krishna N. SharmaNo ratings yet
- Comparing The Effects of Aquatic and Land-Based Exercises On Balance and Walking in Spastic Diplegic Cerebral Palsy ChildrenDocument8 pagesComparing The Effects of Aquatic and Land-Based Exercises On Balance and Walking in Spastic Diplegic Cerebral Palsy ChildrenJorgeAdalbertoCabralPerezNo ratings yet
- CP Research News 2020 May 4Document10 pagesCP Research News 2020 May 4Ana paula CamargoNo ratings yet
- Virtual Reality PaperDocument14 pagesVirtual Reality Paperwalaa eldesoukeyNo ratings yet
- Basso Etal++2015Document11 pagesBasso Etal++2015Violeta Aguayo MüllerNo ratings yet
- Effects of Mental Imagery Technique in Addition To Conventional Physical Therapy To Improve Hand Functions in Chronic Stroke PatientDocument7 pagesEffects of Mental Imagery Technique in Addition To Conventional Physical Therapy To Improve Hand Functions in Chronic Stroke PatientMuhajir AjiNo ratings yet
- DMD 2Document4 pagesDMD 2pkhqkgqm85No ratings yet
- Durairaj Satheeskumar, Ku Dhaneshkumar, K Rajasenthil: KeywordsDocument5 pagesDurairaj Satheeskumar, Ku Dhaneshkumar, K Rajasenthil: KeywordsEmad Eldin Mohamed AbdelatiefNo ratings yet
- Six-Month Follow-Up of Kinesitherapy For Cerebral Motor Disorders in Early ChildhoodDocument8 pagesSix-Month Follow-Up of Kinesitherapy For Cerebral Motor Disorders in Early ChildhoodIJAR JOURNALNo ratings yet
- Strength Training Adolescent Learners With Cerebral Palsy: Randomized ControlledDocument9 pagesStrength Training Adolescent Learners With Cerebral Palsy: Randomized ControlledtiaraaaindahNo ratings yet
- Comparative Effect of Vision Deprived Balance Training Over Free Vision Balance Training Among Stroke SubjectsDocument8 pagesComparative Effect of Vision Deprived Balance Training Over Free Vision Balance Training Among Stroke SubjectsijphyNo ratings yet
- Effectiveness of Sensory Integration Therapy (Vestibular & Proprioception Input) On Gross Motor Functioning in Developmental Delayed and Spastic Diplegic CP ChildrenDocument6 pagesEffectiveness of Sensory Integration Therapy (Vestibular & Proprioception Input) On Gross Motor Functioning in Developmental Delayed and Spastic Diplegic CP ChildrenYanuar Adi SanjayaNo ratings yet
- Dementia, Physical Fitness and Cognitive Function Research PDFDocument9 pagesDementia, Physical Fitness and Cognitive Function Research PDFdevdsantoshNo ratings yet
- Hippotherapy-An Intervention ToDocument11 pagesHippotherapy-An Intervention ToPracticas tresNo ratings yet
- Develop Med Child Neuro - 2014 - Dewar - Exercise Interventions Improve Postural Control in Children With Cerebral Palsy ADocument17 pagesDevelop Med Child Neuro - 2014 - Dewar - Exercise Interventions Improve Postural Control in Children With Cerebral Palsy AEvelyn_D_az_Ha_8434No ratings yet
- Comparison of Different Therapy Approaches in Children With Down SyndromeDocument6 pagesComparison of Different Therapy Approaches in Children With Down SyndromeRosy OktaridaNo ratings yet
- Archive of SID: Research ArticleDocument8 pagesArchive of SID: Research ArticleAnushka RaipureNo ratings yet
- Effect of Passive Range of MotionDocument13 pagesEffect of Passive Range of Motionanggaarfina051821No ratings yet
- SUMBER Eom2014Document6 pagesSUMBER Eom2014Felix Valerian HalimNo ratings yet
- Effects of Hippotherapy and Therapeutic Horseback Riding On Postural Control or Balance in Children With Cerebral Palsy: A Meta-AnalysisDocument8 pagesEffects of Hippotherapy and Therapeutic Horseback Riding On Postural Control or Balance in Children With Cerebral Palsy: A Meta-AnalysisEduardo EstevamNo ratings yet
- Effect of Core Stability Exercises and Treadmill Training On Balance in Children With Down Syndrome - Randomized Controlled TrialDocument10 pagesEffect of Core Stability Exercises and Treadmill Training On Balance in Children With Down Syndrome - Randomized Controlled TrialGayuh Candra BuanaNo ratings yet
- gmTIMP CorrelationDocument7 pagesgmTIMP CorrelationArtur SalesNo ratings yet
- 7608-Article Text-13581-1-10-20210613Document20 pages7608-Article Text-13581-1-10-20210613SuniNo ratings yet
- Tdcs Inglês 1Document8 pagesTdcs Inglês 1Augusto ManoelNo ratings yet
- Cureus 0014 00000030571Document11 pagesCureus 0014 00000030571zizee61No ratings yet
- Abstracts S3: A G A I e F H A A B A A A C B D A e F A A HDocument2 pagesAbstracts S3: A G A I e F H A A B A A A C B D A e F A A HRadu AvramNo ratings yet
- Stroke 2 RCTDocument6 pagesStroke 2 RCTArdhyan ArdhyanNo ratings yet
- ptrs009 01 08Document11 pagesptrs009 01 08mohamedsalahudeen193No ratings yet
- Kristenen, NeckmusclebalanceDocument9 pagesKristenen, NeckmusclebalancePhooi Yee LauNo ratings yet
- Visual AcuityDocument5 pagesVisual AcuityAmr Mohamed GalalNo ratings yet
- Jurnal Propriosepsi GeriatriDocument9 pagesJurnal Propriosepsi GeriatriIra AdventiaNo ratings yet
- Physiotherapy: J o U R N A L o FDocument10 pagesPhysiotherapy: J o U R N A L o FImran TarmiziNo ratings yet
- A Chinese Mind-Body Exercise Improves Self-Control of Children With Autism: A Randomized Controlled TrialDocument12 pagesA Chinese Mind-Body Exercise Improves Self-Control of Children With Autism: A Randomized Controlled TrialNicolas SantibañezNo ratings yet
- 2015 Article 156Document9 pages2015 Article 156Rinto Sapta Andreas SimanjuntakNo ratings yet
- Comparison Between The Effect of NeurodevelopmentaDocument9 pagesComparison Between The Effect of NeurodevelopmentaDellNo ratings yet
- Combined Effects of Mirror Therapy and Exercises On The Upper Extremities in Children With Unilateral Cerebral Palsy: A Randomized Controlled TrialDocument13 pagesCombined Effects of Mirror Therapy and Exercises On The Upper Extremities in Children With Unilateral Cerebral Palsy: A Randomized Controlled Trialdwi agnasariNo ratings yet
- Effect of Manipulating Object Shape Size and Weight Combined With Handarm Bimanual Intensive Training Habit in Improving Upper Ext 2165 7025 1000338Document8 pagesEffect of Manipulating Object Shape Size and Weight Combined With Handarm Bimanual Intensive Training Habit in Improving Upper Ext 2165 7025 1000338Run CapNo ratings yet
- Sensorimotor Training For BalanceDocument7 pagesSensorimotor Training For BalanceAgatha SharmaNo ratings yet
- Journal PPT - Imt 3Document39 pagesJournal PPT - Imt 3Iqbal KhanNo ratings yet
- Maik SLR and Slump Stretching With LBP Neural TensionDocument9 pagesMaik SLR and Slump Stretching With LBP Neural TensionFallahPhysioNo ratings yet
- Mechanical Vestibular Stimulation Versus Traditional Balance ExercisesDocument7 pagesMechanical Vestibular Stimulation Versus Traditional Balance ExercisesPrabanandaAdistanaNo ratings yet
- Effect of Regular Aerobic Exercises On Behavioral, Cognitive and Psychological Response in Patients With Attention Deficit-Hyperactivity DisorderDocument6 pagesEffect of Regular Aerobic Exercises On Behavioral, Cognitive and Psychological Response in Patients With Attention Deficit-Hyperactivity DisorderRaoof ARIFNo ratings yet
- Psychophysiological assessment of human cognition and its enhancement by a non-invasive methodFrom EverandPsychophysiological assessment of human cognition and its enhancement by a non-invasive methodNo ratings yet
- Focus On FunctionDocument18 pagesFocus On FunctionDaniela NevesNo ratings yet
- Neurodevelopmental Treatment Approaches For Children With Cerebral PalsyDocument24 pagesNeurodevelopmental Treatment Approaches For Children With Cerebral PalsyDaniela NevesNo ratings yet
- Neurodevelopmental Treatment (Bobath)Document8 pagesNeurodevelopmental Treatment (Bobath)Daniela NevesNo ratings yet
- Abnormal Sitting Pressures of Hemiplegic CerebralDocument2 pagesAbnormal Sitting Pressures of Hemiplegic CerebralDaniela NevesNo ratings yet
- A Summer Internship Project ON " To Study The Supply Chain Management On Amul Fresh Products" AT GCMMF, AmulDocument19 pagesA Summer Internship Project ON " To Study The Supply Chain Management On Amul Fresh Products" AT GCMMF, AmulweetrydhNo ratings yet
- Timber, PVCu and aluminium window and door hardware systemsDocument24 pagesTimber, PVCu and aluminium window and door hardware systemsOmul Fara NumeNo ratings yet
- 20ME901 Automobile Engineering Unit 3Document74 pages20ME901 Automobile Engineering Unit 36044 sriramNo ratings yet
- 2010-12 600 800 Rush Switchback RMK Service Manual PDFDocument430 pages2010-12 600 800 Rush Switchback RMK Service Manual PDFBrianCook73% (11)
- City MSJDocument50 pagesCity MSJHilary LedwellNo ratings yet
- spl400 Stereo Power Amplifier ManualDocument4 pagesspl400 Stereo Power Amplifier ManualRichter SiegfriedNo ratings yet
- Millennium Separation ReportDocument3 pagesMillennium Separation ReportAlexandra AkeNo ratings yet
- Presentation 1Document20 pagesPresentation 1nikitakhanduja1304No ratings yet
- Mind Map On The History of Science, Technology and SocietyDocument1 pageMind Map On The History of Science, Technology and SocietyJohn Michael Vincent CarreonNo ratings yet
- GVB 1Document8 pagesGVB 1Aaron SylvestreNo ratings yet
- Analysis and Design of Multi Storey Building by Using STAAD ProDocument5 pagesAnalysis and Design of Multi Storey Building by Using STAAD Prolikith rockNo ratings yet
- CHEMICAL ANALYSIS OF WATER SAMPLEDocument5 pagesCHEMICAL ANALYSIS OF WATER SAMPLEAiron Fuentes EresNo ratings yet
- United Airlines Case Study: Using Marketing to Address External ChallengesDocument4 pagesUnited Airlines Case Study: Using Marketing to Address External ChallengesSakshiGuptaNo ratings yet
- Agilent Cool On-Column Operation ManualDocument42 pagesAgilent Cool On-Column Operation Manualdmcevoy1965No ratings yet
- Complete Guide To E-Commerce TechnologyDocument420 pagesComplete Guide To E-Commerce Technologypilatus100% (4)
- Types of NumbersDocument11 pagesTypes of NumbersbrajanosmaniNo ratings yet
- Software Client Linux 21 01Document81 pagesSoftware Client Linux 21 01BronskyNo ratings yet
- SHORT STORY Manhood by John Wain - Lindsay RossouwDocument17 pagesSHORT STORY Manhood by John Wain - Lindsay RossouwPrincess67% (3)
- S06 - 1 THC560 DD311Document128 pagesS06 - 1 THC560 DD311Canchari Pariona Jhon AngelNo ratings yet
- British Isles Composition GuideDocument4 pagesBritish Isles Composition GuidesonmatanalizNo ratings yet
- C-Dot Max-XlDocument39 pagesC-Dot Max-XlGourav Roy100% (3)
- INVENTORY MANAGEMENT TechniquesDocument24 pagesINVENTORY MANAGEMENT TechniquesWessal100% (1)
- Starting A Business Candle Making 2009Document2 pagesStarting A Business Candle Making 2009Carlo Fabros Junio100% (4)
- Komatsud65ex 16dozerbulldozerservicerepairmanualsn80001andup 200727063646Document26 pagesKomatsud65ex 16dozerbulldozerservicerepairmanualsn80001andup 200727063646juan santa cruzNo ratings yet
- Rotational Equilibrium SimulationDocument3 pagesRotational Equilibrium SimulationCamille ManlongatNo ratings yet
- Reversing a String in 8086 Micro Project ReportDocument4 pagesReversing a String in 8086 Micro Project ReportOm IngleNo ratings yet
- LNG Vaporizers Using Various Refrigerants As Intermediate FluidDocument15 pagesLNG Vaporizers Using Various Refrigerants As Intermediate FluidFrandhoni UtomoNo ratings yet
- Admission Procedure For International StudentsDocument8 pagesAdmission Procedure For International StudentsAndreea Anghel-DissanayakaNo ratings yet
- Cyber Security 2017Document8 pagesCyber Security 2017Anonymous i1ClcyNo ratings yet
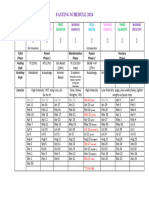
- Moon Fast Schedule 2024Document1 pageMoon Fast Schedule 2024mimiemendoza18No ratings yet