You might also like
- Mucormycosis ManagementDocument3 pagesMucormycosis Managementparteek bajwaNo ratings yet
- ANTIFUNGALSDocument11 pagesANTIFUNGALSCalvoh Asap BiketiNo ratings yet
- Department of Health and Family Welfare Govt. of West BengalDocument35 pagesDepartment of Health and Family Welfare Govt. of West Bengalswagato deyNo ratings yet
- Tocilizumab in Covid-19 PatientsDocument8 pagesTocilizumab in Covid-19 Patientsdrmarcellino_msNo ratings yet
- How COVID-19 Has Changed The Management of Glomerular DiseasesDocument4 pagesHow COVID-19 Has Changed The Management of Glomerular DiseasesHendri WahyudiNo ratings yet
- How COVID-19 Has Changed The Management of Glomerular DiseasesDocument4 pagesHow COVID-19 Has Changed The Management of Glomerular DiseasesLouie MercadoNo ratings yet
- Corticosteroids: Ghadi Mahmoud Elbarghathi Roll Number: 1950 5 Year 2021-2022Document26 pagesCorticosteroids: Ghadi Mahmoud Elbarghathi Roll Number: 1950 5 Year 2021-2022Ghadi ElbarghathiNo ratings yet
- Mucormycosis in EntDocument33 pagesMucormycosis in EntNandini GuptaNo ratings yet
- EVMS Critical Care COVID-19 Protocol PDFDocument18 pagesEVMS Critical Care COVID-19 Protocol PDFGreyWolf1776No ratings yet
- Pragesh Mucor ArticalDocument6 pagesPragesh Mucor ArticalShobhitNo ratings yet
- NAG Filariasis As of Nov 2017Document2 pagesNAG Filariasis As of Nov 2017Rhod Bernaldez EstaNo ratings yet
- 2 Epitaxis Covid19Document3 pages2 Epitaxis Covid19andinNo ratings yet
- Mucormycosis Advisory From Icmr in Covid19 TimeDocument1 pageMucormycosis Advisory From Icmr in Covid19 Timeprashant_rmlnluNo ratings yet
- 07 - 10 - 21 Treatment of Covid 19 InfectionDocument26 pages07 - 10 - 21 Treatment of Covid 19 InfectionStonefalconNo ratings yet
- COVID-19 Treatment Guidelines: Clinical ManagementDocument6 pagesCOVID-19 Treatment Guidelines: Clinical ManagementPetra SpringNo ratings yet
- AspergillosisDocument6 pagesAspergillosisdisk_la_poduNo ratings yet
- (1479683X - European Journal of Endocrinology) ENDOCRINOLOGY IN THE TIME OF COVID-19 - Management of Adrenal InsufficiencyDocument8 pages(1479683X - European Journal of Endocrinology) ENDOCRINOLOGY IN THE TIME OF COVID-19 - Management of Adrenal Insufficiencysanti lestariNo ratings yet
- Sino-Orbital Mucormycosis in A COVID-19 Patient: A Case ReportDocument5 pagesSino-Orbital Mucormycosis in A COVID-19 Patient: A Case Reportkarol castellonNo ratings yet
- Palliative COVID 19Document4 pagesPalliative COVID 19Lasmarihot PasaribuNo ratings yet
- Annrheumdis 2020 218479.fullDocument9 pagesAnnrheumdis 2020 218479.fullhilya ayme narvayNo ratings yet
- Glucocorticoids and TCZ in COVID-19Document9 pagesGlucocorticoids and TCZ in COVID-19Silvio LimaNo ratings yet
- Fleseriu@ohsu - Edu: Via Free AccessDocument13 pagesFleseriu@ohsu - Edu: Via Free AccessJorge Eduardo Sánchez MoralesNo ratings yet
- Anthelmentics Version 2Document21 pagesAnthelmentics Version 2N Gv FcNo ratings yet
- (1479683X - European Journal of Endocrinology) ENDOCRINOLOGY IN THE TIME OF COVID-19 - Management of Diabetes Insipidus and HyponatraemiaDocument7 pages(1479683X - European Journal of Endocrinology) ENDOCRINOLOGY IN THE TIME OF COVID-19 - Management of Diabetes Insipidus and HyponatraemiaAriesta PermatasariNo ratings yet
- Medical Management of MucormycosisDocument19 pagesMedical Management of MucormycosisNayan GuptaNo ratings yet
- Day 1 Day 9Document1 pageDay 1 Day 9abdul hamidNo ratings yet
- Evms Critical Care Covid-19 Management Protocol: Paul Marik, MDDocument9 pagesEvms Critical Care Covid-19 Management Protocol: Paul Marik, MDJohn GaltNo ratings yet
- A Protocol of Infection Control For Mechanical Thrombectomy in Possible COVID-19 Patients: Tokai University COVID-19 ManualDocument5 pagesA Protocol of Infection Control For Mechanical Thrombectomy in Possible COVID-19 Patients: Tokai University COVID-19 ManualMartha OktaviaNo ratings yet
- Surgery in Covid-19 PandemicDocument49 pagesSurgery in Covid-19 PandemicEmmanuel DanielsNo ratings yet
- MSKcorticosteroidguidanceDocument7 pagesMSKcorticosteroidguidanceKarthikeyan DNo ratings yet
- Critical Covid ICUDocument41 pagesCritical Covid ICULia Damayanti EgcNo ratings yet
- Clin Infect Dis 2009Document59 pagesClin Infect Dis 2009cdsaludNo ratings yet
- Evms Critical Care Covid-19 Management Protocol: Paul Marik, MDDocument11 pagesEvms Critical Care Covid-19 Management Protocol: Paul Marik, MDPrashanta Barman Palas100% (1)
- Consortium ProtocolDocument16 pagesConsortium Protocolthe kingfishNo ratings yet
- L11 Medically Compromised Patients 2Document59 pagesL11 Medically Compromised Patients 2elle70503No ratings yet
- Experience With IV Metronidazole To Treat Moderate To Severe Amebiasis in JapanDocument5 pagesExperience With IV Metronidazole To Treat Moderate To Severe Amebiasis in JapanRobin ScherbatskyNo ratings yet
- An Institutional Study On Covid-19 Associated Rhino-Orbital-Cerebral MucormycosisDocument8 pagesAn Institutional Study On Covid-19 Associated Rhino-Orbital-Cerebral MucormycosisIJAR JOURNALNo ratings yet
- EVMS Critical Care COVID-19 ProtocolDocument17 pagesEVMS Critical Care COVID-19 ProtocolDavid GuzmanNo ratings yet
- Webinar-Epicare-April 9 ASMs Covid-19 InteractionsDocument12 pagesWebinar-Epicare-April 9 ASMs Covid-19 InteractionsDiana ZețuNo ratings yet
- 31 - Antimicrobial Drugs III (Antifungals) LectureDocument35 pages31 - Antimicrobial Drugs III (Antifungals) LectureSwara SawantNo ratings yet
- DraftDocument3 pagesDraftEvelyn LimNo ratings yet
- Oral Mucositis:: Complicating ChemotherapyDocument35 pagesOral Mucositis:: Complicating ChemotherapySomesh KumarNo ratings yet
- Jama Murthy 2020 It 200008Document2 pagesJama Murthy 2020 It 200008jorgeNo ratings yet
- COVID-19 InterimGuidelines Treatment ENGDocument24 pagesCOVID-19 InterimGuidelines Treatment ENGHouda LaatabiNo ratings yet
- 6.antifungal AgentsDocument51 pages6.antifungal Agentsmulatumelese0% (1)
- Prone Position Guidelines-2Document14 pagesProne Position Guidelines-2SAMINo ratings yet
- University of Maryland Medical Center Fluconazole (Diflucan®)Document6 pagesUniversity of Maryland Medical Center Fluconazole (Diflucan®)damondouglasNo ratings yet
- EVMS Critical Care COVID 19 Protocol 4 2 2020-RevisedDocument11 pagesEVMS Critical Care COVID 19 Protocol 4 2 2020-RevisedGabriellaNo ratings yet
- Anti Fungal Drugs: Dr. Jahid Assistant Professor (Unit Pharmacology) CucmsDocument70 pagesAnti Fungal Drugs: Dr. Jahid Assistant Professor (Unit Pharmacology) Cucmslailatul husnaNo ratings yet
- Edited COVID19 HANDOUT Requina SindiongDocument5 pagesEdited COVID19 HANDOUT Requina SindiongJannen CasasNo ratings yet
- ASTHMA RestriveraDocument18 pagesASTHMA RestriveraAoi ShinNo ratings yet
- Orthodontic Treatment of Patients With Medical DisordersDocument17 pagesOrthodontic Treatment of Patients With Medical DisordersJayshri SingviNo ratings yet
- 10 1136@bmj m1963Document5 pages10 1136@bmj m1963martin quispeNo ratings yet
- Papers Intervencion CovidDocument6 pagesPapers Intervencion Coviddayllyn iglesiasNo ratings yet
- COVID 19 and VTE - PPTDocument25 pagesCOVID 19 and VTE - PPT8w46zmqr58No ratings yet
- EVMS Critical Care COVID-19 ProtocolDocument38 pagesEVMS Critical Care COVID-19 ProtocolDrivailaNo ratings yet
- Anesth Analg 2019 129 6 1504-11Document8 pagesAnesth Analg 2019 129 6 1504-11Fernando SousaNo ratings yet
- LF Anil KRDocument122 pagesLF Anil KRanil sahNo ratings yet
- Summary Review Orig1s000SumRDocument26 pagesSummary Review Orig1s000SumRAlvaro MuñozNo ratings yet
- COVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19From EverandCOVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19No ratings yet
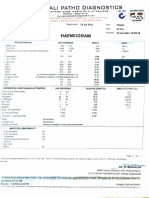
- Gitanjali Patho Diagnostics: HaemogramDocument6 pagesGitanjali Patho Diagnostics: HaemogramShivenra RajNo ratings yet
- Monthly Statement: This Month's SummaryDocument3 pagesMonthly Statement: This Month's SummaryShivenra RajNo ratings yet
- Name Lab No. Mrs - Utkarsha Singh 316877859 Age: 30 Years Gender: Female A/c Status P Ref By: Dr. SELF Collected Received Reported Report StatusDocument1 pageName Lab No. Mrs - Utkarsha Singh 316877859 Age: 30 Years Gender: Female A/c Status P Ref By: Dr. SELF Collected Received Reported Report StatusShivenra RajNo ratings yet
- Organism: Enterococcus Faecalis - 10000 Colonies/ml GrownDocument2 pagesOrganism: Enterococcus Faecalis - 10000 Colonies/ml GrownShivenra RajNo ratings yet
- Special Consideration in Neonatal Resuscitation - 2022 - Seminars in PerinatologDocument8 pagesSpecial Consideration in Neonatal Resuscitation - 2022 - Seminars in PerinatologEduardo Rios DuboisNo ratings yet
- Manual of Homeopathic Practice (1876)Document864 pagesManual of Homeopathic Practice (1876)Dr. JimNo ratings yet
- THE Center: Anxiety DisordersDocument13 pagesTHE Center: Anxiety DisordersOti VuraNo ratings yet
- Glucose KitDocument2 pagesGlucose KitJuan Enrique Ramón OrellanaNo ratings yet
- Assessor Guide EntryLevelSHCODocument12 pagesAssessor Guide EntryLevelSHCOEka BNo ratings yet
- American Soc. of Addiction Medicine Naloxone StatementDocument5 pagesAmerican Soc. of Addiction Medicine Naloxone Statementwebmaster@drugpolicy.orgNo ratings yet
- Table 5.1-2 Minnesota Multiphasic Personality Inventory Validity and Clinical Scales ValidityDocument4 pagesTable 5.1-2 Minnesota Multiphasic Personality Inventory Validity and Clinical Scales ValidityReisya GinaNo ratings yet
- Tarea Nâ°1.es - en Derecho Civil Legalmente RubiaDocument5 pagesTarea Nâ°1.es - en Derecho Civil Legalmente RubiaMax Alva SolisNo ratings yet
- MGT 338 Employability & Entrepreneurship: 1.0 Executive SummaryDocument21 pagesMGT 338 Employability & Entrepreneurship: 1.0 Executive Summaryeggie dan100% (1)
- Referat Limba Engleză-Zidaroiu Ionuț-EduardDocument6 pagesReferat Limba Engleză-Zidaroiu Ionuț-EduardEduard IonutNo ratings yet
- Contingency PlansDocument8 pagesContingency PlansNoel GalangNo ratings yet
- Business Studies 05Document22 pagesBusiness Studies 05Nepomuk Balthasar HaindlNo ratings yet
- Analisis Keberhasilan Implementasi RME Mutu PelayananDocument8 pagesAnalisis Keberhasilan Implementasi RME Mutu PelayananWinda PurbaNo ratings yet
- Tranexamic Acid MouthwashDocument1 pageTranexamic Acid MouthwashTalal MazharNo ratings yet
- Ansi+asse+z359 13-2013Document54 pagesAnsi+asse+z359 13-2013Oscar Casso100% (1)
- The Amazing DeclineDocument26 pagesThe Amazing DeclineSuzanne HumphriesNo ratings yet
- 10Document19 pages10Bruno100% (3)
- Veterinary Clinical Diagnosis DVM 2022-23Document51 pagesVeterinary Clinical Diagnosis DVM 2022-23MilkiyasNo ratings yet
- Overconfidence As A Cause of Diagnostic Error in Medicine PDFDocument22 pagesOverconfidence As A Cause of Diagnostic Error in Medicine PDFIulianZaharescuNo ratings yet
- Req. #1: EMPLOYEES Toyota Workers Say Bosses Have Ignored Safety Concerns For YearsDocument8 pagesReq. #1: EMPLOYEES Toyota Workers Say Bosses Have Ignored Safety Concerns For YearsbellalitNo ratings yet
- New Mcgraw Hill EducationDocument132 pagesNew Mcgraw Hill EducationAlexandru LeșanNo ratings yet
- Latest ELC501 Final ExamDec2015Document13 pagesLatest ELC501 Final ExamDec2015ikmal0% (1)
- Reflection Essay - HRM533Document9 pagesReflection Essay - HRM533Mazatul NadirahNo ratings yet
- Journal of Public Procurement: Article InformationDocument38 pagesJournal of Public Procurement: Article Informationwalelgn eyayuNo ratings yet
- Complicated GrievingDocument117 pagesComplicated GrievingEra Galuh100% (1)
- Migrants' Election ManifestoDocument2 pagesMigrants' Election ManifestoMimi Panes - CorosNo ratings yet
- 12 Compulsive Activities ChecklistDocument8 pages12 Compulsive Activities ChecklistShrey BadrukaNo ratings yet
- Freud's Psychosexual Stages of DevelopmentDocument30 pagesFreud's Psychosexual Stages of DevelopmentjessaNo ratings yet
- Vitalsigns PDFDocument36 pagesVitalsigns PDFSuneel Kumar PrajapatiNo ratings yet
- Paper7 Syl22 Dec23 Set2 SolDocument20 pagesPaper7 Syl22 Dec23 Set2 SolAkash AgarwalNo ratings yet